
There is a well-recognized maternal health crisis in the United States. In 2020, 861 women* died of pregnancy-related complications. This rate remains higher than that of any other resource-rich country.1 Alarming disparities exist, with non-Hispanic Black women and American Indian/Alaska Native (AI/AN) women having significantly higher pregnancy-related mortality rates than non-Hispanic White women.1 Severe maternal morbidity (SMM) is part of this maternal health crisis. As with pregnancy-related deaths, rates of SMM are increasing and racial and ethnic disparities continue.2,3
The National Association of Nurse Practitioners in Women’s Health (NPWH) asserts that board-certified women’s health nurse practitioners (WHNP-BCs) are crucial partners in addressing the crisis. WHNP-BCs are clinical experts in providing routine and complex women’s and gender-related healthcare, promoting healthy behaviors before, during, and after pregnancy; preventing development of risk factors for maternal health complications prior to pregnancy; identifying and addressing existing risk factors prior to and during pregnancy and postpartum; and optimizing maternal health outcomes.4 They provide this care in a variety of settings, which include private practice offices, community health centers, health departments, rural health clinics, military facilities, corrections facilities, antepartum testing/fetal evaluation centers, inpatient hospital settings, and clients’ homes, and through telehealth.5
The WHNP is the only nurse practitioner population focus to hold enumerated competencies in providing high-risk pregnancy and postpartum care.6 WHNP signifies nurse practitioners who have completed graduate-level nursing programs that, in addition to preparing the graduate to meet nurse practitioner core competencies, give them the expanded depth and breadth of knowledge and skills necessary to provide primary care meeting the distinct needs of this population from puberty through their adult lifespan.4,6 Only individuals who have completed a nationally accredited graduate or postgraduate WHNP program are eligible to sit for the national certification examination and to use the title WHNP-BC.7 WHNPs are highly qualified to provide both routine and high-risk pregnancy and postpartum care including identification and mitigation of factors that may place an individual at increased risk for maternal complications. They collaborate with others on the healthcare team to foster optimal patient outcomes.
WHNPs who specialize in high-risk antepartum and postpartum care are particularly well suited to enhance health outcomes when there are identified maternal morbidity and mortality risks.6 The WHNP provides and coordinates this care in both outpatient and inpatient settings and can facilitate a seamless transition to well care and ongoing specialty care.
NPWH emphasizes that a multidisciplinary, community-wide, and systems-level approach is essential to alleviate the current maternal health crisis. WHNPs must be on the team not only to provide expert direct care but also to lead quality improvement initiatives, participate in research, and represent their unique perspective on maternal mortality review committees, perinatal quality collaboratives, and other national, regional, state, and local efforts seeking to improve maternal health.
NPWH advocates for health policies at all levels that ensure WHNPs are included in maternal health initiatives. NPWH seeks to educate policy makers, healthcare systems and hospitals, employers, payors, patients, and other stakeholders in maternal health that having board-certified WHNPs on the team strengthens the country’s crucial efforts to solve the maternal health crisis and save lives.
Background
In the US, a pregnancy-related death is defined as one that occurs during pregnancy or within 12 months of the end of a pregnancy causally related to the pregnancy. This causality refers to deaths related to a pregnancy complication, a chain of events initiated by pregnancy, or aggravation of an unrelated condition by the physiologic effects of pregnancy.8 A death is considered preventable if it is determined that the death may have been averted through one or more changes to community, health facility, patient, provider, and/or systems-level factors.9 The Centers for Disease Control and Prevention estimates that 3 in 5 pregnancy-related deaths in the US are preventable.8
Maternal mortality review committees have facilitated the identification and further specification of factors that may contribute to preventable pregnancy-related deaths, including those at the community (eg, unstable housing, lack of transportation), health facility (eg, lack of appropriate personnel or services, lack of guiding protocols), patient or family (eg, lack of knowledge of warning signs, nonadherence to medical regimens or advice), provider (eg, missed or delayed diagnosis, lack of continuity of care), and systems levels (eg, lack of guiding policies, procedures, or standards, inadequate case coordination).8 Thus, to eliminate preventable pregnancy-related deaths, especially when there are disparities, strategies must be engaged at several levels and multiple factors addressed.
The major causes of pregnancy-related deaths that occur while the individual is pregnant are hemorrhage, cardiovascular conditions, and other medical conditions such as blood disorders, immune disorders, and kidney disease.8 Hemorrhage and amniotic fluid embolism are major causes on the day of delivery. During the postpartum period, the causes of pregnancy-related deaths vary from the first several days through the first year (Box).8,10
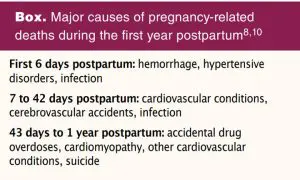
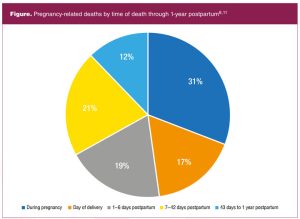
Of note, over 50% of pregnancy-related deaths occur postpartum (Figure).8,11
As another component of the maternal health crisis, SMM has no clearly established definition, but traditionally it includes unintended outcomes of the process of labor and delivery that result in significant short-term or long-term consequences to the individual’s health.2 Recently, the importance of expanding the definition of and data analysis for SMM to include complications requiring hospitalization that occur during pregnancy and beyond delivery to 42 days postpartum is being recognized.12 Severe complications may be considered near misses for pregnancy-related deaths because without early identification and treatment, death would have occurred in some cases.2 In 2017, there were over 25,000 hospital deliveries with a diagnosis or complication constituting an SMM. The five most common complications were disseminated intravascular coagulation, hysterectomy, acute kidney failure, sepsis, and adult respiratory distress syndrome.13 The rates of SMM among hospital deliveries for non-Hispanic Black and AI/AN women were more than 1.5 times as high as those for White, Hispanic, Asian/Pacific Islander, and women of other races and ethnicities.13
The 2017 data did not include SMM cases during the prenatal period or postpartum after hospital discharge. Transfusion, sepsis, thrombotic embolism, and adult respiratory distress syndrome are the SMM conditions most associated with the prenatal period. The most common SMM cases added when including the first 42 days postpartum after hospital discharge involve pulmonary edema, sepsis, and thrombotic embolism.13
Attention to health prior to pregnancy, during pregnancy, during birth, during the full year postpartum, and interpregnancy is critical to improve maternal health outcomes. WHNPs are essential maternity care team members, with competencies in providing expert clinical care to foster improved outcomes throughout the maternal health continuum. They have distinct competencies to provide uncomplicated and complex care independently and collaboratively for patients across this continuum.6
As well, growth in the number of WHNPs situates them to meet the increasing demand for women’s and gender-related healthcare providers across the country. According to the National Certification Corporation, the certifying body for the WHNP population focus, there were 12,369 certified WHNPs in the US at the close of 2021.14 The Health Resources and Service Administration projects that the supply of WHNPs will grow to 20,020 by 2030 if the number of annual new WHNP entrants remains unchanged.15 Conversely, a continuing decrease is projected in the number of obstetricians between now and 2030.15,16 A deliberate consideration for utilizing WHNPs as maternity care providers can lessen the gap between supply and demand for all aspects of healthcare that influence maternal health and especially for people in rural and underserved areas.
Prepregnancy and interpregnancy care
Maternal health outcomes cannot be significantly improved if the focus is only on the time of pregnancy and birth. Factors that contribute to poor outcomes include health behaviors, health conditions, and environmental and social issues that are often present well before a pregnancy.13 A comprehensive approach addressing health before and between pregnancies is essential.
Prepregnancy care provides the opportunity to assess for and address identified risk factors for maternal complications prior to pregnancy, promote healthy lifestyles, administer recommended immunizations, and counsel about and provide contraception if desired in a manner tailored to each individual’s needs.17 Interpregnancy care, or the care provided between pregnancies, has the same goals and extends care beyond the postpartum period.18
WHNPs are at the forefront of providing healthcare services in this realm because they routinely see reproductive-age patients for well-care and other episodic visits. They can identify, assess, manage or comanage, and coordinate care for health conditions such as cardiovascular disease, hypertension, diabetes, unhealthy weight, substance use disorders, mental health disorders, and intimate partner violence that have implications for maternal complications, thus allowing implementation of optimal management prior to pregnancy.12 With expert knowledge of the implications of previous complications such as postpartum depression, preeclampsia, gestational diabetes, and thromboembolism, WHNPs are skilled at identifying these risks and initiating attention to prevention and management strategies important to the health of future pregnancies.18 Further, they assess for social and structural determinants of health to determine the need for additional support through housing, access to food, transportation, and financial resources. WHNPs engage in interdisciplinary collaboration to optimize outcomes.
Prenatal care
Coordination of equitable prenatal care includes ensuring that each pregnant person has access to resources and the level of care that will meet their individual needs. Appropriate levels of care during pregnancy are determined through early and ongoing risk assessment to prevent, recognize, and treat conditions associated with maternal morbidity and mortality.19 The provision of effective, efficient, risk-appropriate prenatal care is facilitated when the capabilities and expertise of healthcare providers are matched with the patient’s circumstances and needed level of care.19
The WHNP has the knowledge and ability to identify risk factors and health conditions that require immediate intervention, comanagement, consultation, and/or referral to a higher level of care. Early identification of high-risk pregnancies allows prevention and treatment of conditions associated with maternal morbidity and mortality. Risk assessment facilitates development of a plan of care, including referral and consultation as appropriate, among healthcare providers of basic, specialty, and subspecialty prenatal care on the basis of the patient’s circumstances and the capability of the individual healthcare providers.19
Importantly, WHNPs comanage care for patients with high-risk prenatal conditions in collaboration with other healthcare team members (eg, obstetricians, maternal-fetal medicine specialists, cardiologists, mental health professionals) in both inpatient and outpatient settings. WHNPs provide care in antepartum triage units and as hospitalists for antepartum patients as members of high-risk maternal healthcare teams. WHNPs are maternity care providers who partner with intrapartum care providers such as obstetricians and midwives as patients transition from antepartum to giving birth and into the postpartum period.
Postpartum care
Healthcare should be individualized and ongoing during the first year postpartum, with attention to medical, mental, and behavioral health needs and social and material support. As noted earlier, this is critical because more than one-half of pregnancy-related deaths occur in the first year postpartum and up to 40% occur in the first 6 weeks postpartum.8,11 The American College of Obstetricians and Gynecologists recommends contact with a healthcare provider within the first 3 weeks postpartum and a comprehensive visit no later than 12 weeks postpartum to best meet the needs of women in the postpartum period. WHNPs have the expertise to assess for and address acute postpartum issues (eg, hypertension, mental health, social support needs) during early postpartum visits and provide continuity of care at the comprehensive postpartum visit.
Unfortunately, as many as 40% of women do not attend a postpartum visit.20 These are often individuals with limited resources who may be the most vulnerable to complications. WHNPs are key healthcare providers for this group. The growing number of WHNP postpartum hospitalists are particularly valuable in reaching patients prior to hospital discharge to assess for and mitigate risk factors, identify potential for postpartum complications, address resource needs, and arrange follow-up.21 WHNPs in perinatal substance use disorder clinics provide essential care during pregnancy that extends through the first year postpartum when frequent healthcare contact is essential.22 WHNPs are able to provide, comanage, and coordinate ongoing care for all patients postpartum through transition to well care and specialty care, collaborate in management of pre-existing chronic health conditions, and coordinate referrals to community resources for social and material support.
Implications for improving maternal health outcomes
WHNPs are crucial partners in addressing the maternal health crisis. They are clinical experts in promoting healthy behaviors before, during, and after pregnancy; preventing development of risk factors for maternal health complications prior to pregnancy; identifying and addressing existing risk factors prior to and during pregnancy and postpartum; and optimizing maternal health outcomes. They provide this care in a variety of settings independently and collaboratively with other healthcare team members. WHNPs are able to lead quality improvement initiatives and development of models of care that are tailored to unique needs within communities, which is especially important in areas where there are shortages and disparities in women’s healthcare. Telehealth and remote monitoring, attention to reducing barriers to care related to social and structural determinants of health, and development of interdisciplinary partnerships are all strategies in which the WHNP participates to improve maternal health outcomes. Beyond direct patient care, WHNPs are highly qualified to represent their unique perspective on maternal mortality review committees and other national, regional, state, and local committees seeking to improve maternal health. WHNPs with research backgrounds are essential leaders for studies that address the maternal health crisis.
Recommendations
NPWH will provide leadership to ensure:
- Maternal health stakeholders (eg, healthcare providers, policy makers, patients) are informed about the distinctive qualifications of board-certified WHNPs that make them crucial partners in addressing the maternal health crisis.
- Board-certified WHNPs are represented on initiatives, commissions, and collaborations that promote maternal health and access to quality care throughout the reproductive-age continuum.
- Collaborative engagement with other professional organizations continues to advance the development, implementation, and evaluation of multidisciplinary best practices that include WHNPs to eliminate preventable maternal morbidity and mortality.
- Continuing education programs and other evidence-based resources are available to WHNPs and WHNP program faculty to update knowledge regarding evidence-based strategies to promote maternal health.
References
- Hoyert DL. Maternal mortality rates in the United States, 2020. NCHS Health E-Stats. 2022.
- American College of Obstetricians and Gynecologists; Society for Maternal-Fetal Medicine. Obstetric Care Consensus No. 5. Severe maternal morbidity: screening and review. Obstet Gynecol. 2016;128(3):e54-e60.
- Brown CC, Adams CE, George KE, Moore JE. Associations between comorbidities and severe maternal morbidity. Obstet Gynecol. 2020;136(5):892-901.
- National Association of Nurse Practitioners in Women’s Health. White paper: The essential role of women’s health nurse practitioners.
- National Association of Nurse Practitioners in Women’s Health. 2018 NPWH women’s health nurse practitioner workforce demographics and compensation survey: Highlights report. November 2, 2019.
- National Association of Nurse Practitioners in Women’s Health. Women’s Health Nurse Practitioner: Guidelines for Practice and Education, 8th ed. Washington, DC: NPWH; 2020.
- National Certification Corporation. 2022 Candidate Guide Women’s Health Care Practitioner WHNP-BC. Chicago, IL: NCC; 2022.
- Petersen EE, Davis NL, Goodman D, et al. Vital signs: pregnancy-related deaths, United States, 2011-2015, and strategies for prevention, 13 states, 2013-2017. MMWR Morb Mortal Wkly Rep. 2019;68(18):423-429.
- Metz TD. Eliminating preventable maternal deaths in the United States: progress made and next steps. Obstet Gynecol. 2018;132(4):1040-1045.
- Smid MC, Maeda J, Stone NM, et al. Standardized criteria for review of perinatal suicides and accidental drug-related deaths. Obstet Gynecol. 2020;136(4):645-653.
- Davis NL, Smoots AN, Goodman DA; Centers for Disease Control and Prevention. Pregnancy-related deaths: data from 14 U.S. maternal mortality review committees, 2008-2017. Reviewed September 4, 2019.
- Declercq ER, Cabral HJ, Cui X, et al. Using longitudinally linked data to measure severe maternal morbidity. Obstet Gynecol. 2022;139(2):165-171.
- Office of the Surgeon General. The Surgeon General’s call to action to improve maternal health [Internet]. Washington, DC: US Department of Health and Human Services; 2020.
- National Certification Corporation. About NCC. Currently certified by examination. 2022.
- US Department of Health and Human Services, Health Resources and Services Administration, Bureau of Health Workforce. National Center for Health Workforce Analysis. Projections of Supply and Demand for Women’s Health Service Providers: 2018-2030. March 2021.
- Burlone S, Moore L, Johnson W. Overcoming barriers to accessing obstetric care in underserved communities. Obstet Gynecol. 2019;134(2):271-275.
- American College of Obstetricians and Gynecologists. Committee opinion no. 762. Prepregnancy counseling. Obstet Gynecol. 2019;133(1):e78-e89.
- American College of Obstetricians and Gynecologists; Society for Maternal Fetal Medicine. Obstetric Care Consensus No. 8. Interpregnancy care. Obstet Gynecol. 2019;133(1):e51-e72.
- AAP Committee on Fetus and Newborn; ACOG Committee on Obstetric Practice. Guidelines for Perinatal Care, 8th ed. Elk Grove Village, IL: American Academy of Pediatrics; Washington, DC: American College of Obstetricians and Gynecologists; 2017.
- American College of Obstetricians and Gynecologists. Committee opinion no. 736. Optimizing postpartum care. Obstet Gynecol. 2018;131(5):e140-e150.
- Nagtalon-Ramos J, Reymann K, Wood A. Development of the WHNP postpartum hospitalist role: perspectives from Philadelphia. Womens Healthcare. 2022;10(1):22-31.
- American College of Obstetricians and Gynecologists. Committee opinion no. 711. Opioid use and opioid use disorder in pregnancy. Obstet Gynecol. 2017;130(2):e81-e94.
NPWH gratefully acknowledges Aundria Cannon, MSN, WHNP-BC; Jennifer Hawn, MSN, WHNP-BC; Beth Kelsey, EdD, APRN, WHNP-BC; Sue Kendig, JD, WHNP-BC; Komkwuan Paruchabutr, DNP, FNP-BC, WHNP-BC, CNM; Amanda Sauer, MSN, WHNP-BC; and Lisa Hammond, MSN, CRNP, WHNP-BC, for their contributions as writing group members for this position statement.
Approved by NPWH Board of Directors: June 16, 2022