
With all the news on the rollout of Covid-19 immunizations, we’ve been seeing a lot of injection administrations on TV recently. Some of the videos make me cringe. How about you? I couldn’t believe how many times I saw the one where the vaccine is visibly dripping down the outside of the patient’s arm, obviously resulting in a sub-therapeutic dose. Or a new one this week where the injector palpates the injection area with a gloved hand before giving the needle.
But who am I to be questioning injection technique? Well, I was one of the first pharmacists in Atlantic Canada to be trained to administer injections by a wonderful group of Public Health nurses using a detailed program from Dalhousie University in Nova Scotia. At the same time, we were trained to deliver the program to other pharmacists. Along with a team of nurses, I trained about half of the pharmacists in our province over the following years, presenting the program every few months. I also helped test the students at the end of each program, and this has made me very picky about technique!
As an instructor I essentially had an in-depth review every few months as we explained and demonstrated ideal injection techniques and certified pharmacists to administer IM and SC injections in the arm. Researchers tell us that we forget information over time, and it’s true. When teaching the program, I would sometimes realize that I had dropped some small part of the ideal technique, like landmarking every time, for example. Teaching had become a regular refresher for me – something that, to my knowledge, is not required in any profession.
How to get that “didn’t feel a thing” reaction
I also have a personal quirk about not wanting to inflict pain on others. So I did additional research on how to minimize the pain of an injection. From my own experience receiving yearly flu shots, I knew needles could be almost pain-free or quite painful, depending on small details of the administration technique. My own patients would often comment that they “didn’t feel a thing.” I remember telling one elderly gentleman he could move to the observation area when I’d finished, and he asked “Aren’t you going to give me my needle?” and, if I had, he argued, where was it? (in the sharps container, of course!) He had been distracted, chatting with one of my assistants. So, it seems that what I learned had worked and I passed along these techniques to my students. Perhaps there will be some fresh ideas you can use here too.
Get more tips like this for Nurse Practitioners delivered to your inbox biweekly. Sign up here.
Some of my tips came from other injectors or articles and studies I read, some were included in our course, and I learned a lot from the co-presenters of our injection program too! But in spite of my training, little things still went wrong occasionally and I would further improve my technique so it wouldn’t happen again. So, in the spirit of learning from each other, here are some thoughts on working toward an ideal injection technique that is effective, pain-free, and safe for the patient and the injector.
Ensure the injection reaches the correct location
-
- Landmark every time – It seems very few injectors landmark, even though it is
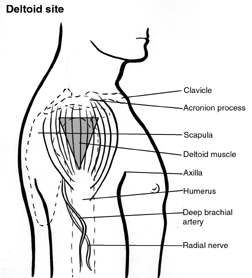 recommended to do this every time. An IM arm injection is intended for the deltoid, a virtually invisible muscle under the skin. Too high, it will be given into the tendon or shoulder capsule. Too low and you could hit the brachial nerve or a major artery. To be fully effective, an IM vaccine must be injected into the muscle. The deltoid is landmarked by measuring three finger-widths down from the acromion process in the shoulder and visualizing an inverted triangle with its wide top just below your third finger and its bottom point level with the underarm. Don’t skip this step.
recommended to do this every time. An IM arm injection is intended for the deltoid, a virtually invisible muscle under the skin. Too high, it will be given into the tendon or shoulder capsule. Too low and you could hit the brachial nerve or a major artery. To be fully effective, an IM vaccine must be injected into the muscle. The deltoid is landmarked by measuring three finger-widths down from the acromion process in the shoulder and visualizing an inverted triangle with its wide top just below your third finger and its bottom point level with the underarm. Don’t skip this step. - Be at your patient’s level when injecting into the deltoid – Standing changes your point of view and increases the risk of giving a needle higher than the target zone. My last IM injection (shingles vaccine, 2nd dose) was only 1½ “finger widths” down from the acromion process – well above the target zone – and might have explained the nasty reaction I had from it. The injector was standing and didn’t landmark, while I was seated.
- Use the correct length needle – 1 to-1.5-inch needles are recommended for adult IM injections. If a shorter needle is used, the vaccine might not reach the muscle, landing in the sub-cutaneous space instead, especially in a heavy person with more sub-cutaneous fat tissue. Here’s why I mention this: Many people in a community I started working in didn’t believe flu shots worked. I wondered why. An order from a local doctor’s office for 400 half-inch needles at the start of flu season provided a likely explanation.
- Don’t have your thumb/finger on the plunger until the needle is fully inserted (I saw a lot of this on TV too) – This makes it very easy to accidentally put pressure on the plunger too soon. This is a likely explanation for the TV catastrophe of vaccine running down the outside of the patient’s arm. Think of it as having your finger on the trigger before you’re ready to shoot!
Make it as pain-free as possible
- Let the alcohol dry – This is pretty basic but, surprisingly, often skipped. It only takes a few extra seconds and you can use this time to give post-injection advice or just explain that you’re doing everything possible to make their injection pain-free.
- Insert and remove the needle quickly – a slow needle is a painful one. Think of a paper cut or a small cut with a sharp knife. If it’s quick, you don’t even realize you’ve been cut until you see the blood! Although advice varies on how fast the medication should be dispensed, I could never find any science to say you shouldn’t inject quickly also. I generally would be in, dispense, and out of the arm in less than 2 seconds for flu shots. And the syringe would be into the sharps container in less than 3!
- Distract – Although some patients prefer to know when it’s coming, having their attention elsewhere actually reduces the perception of pain. Telling them to take a deep breath may be all that’s needed (or available) but I can tell you from experience, a simple drawing app on a tablet works amazingly well to distract children. After the injection (when they don’t like you anymore), offering to send their drawing to mommy’s computer provides a second distraction and turns you into a cool person!
- Make sure the arm is relaxed – I felt an actual “crunch” once when I gave an injection to a guy who was obviously a body-builder. He seemed relaxed, but wasn’t. He told me it was the most painful injection he’d ever received – ouch! I really felt bad. But I never forgot to ensure the arm was relaxed after that.
- Apply pressure around the injection area – Your brain can only handle a limited number of signals at once. Just a slight pressure on the skin can lessen the perception of pain significantly. Think of it as a subconscious form of distraction. My nurse colleagues would demonstrate a technique of landmarking just before injecting then sliding the hand toward the side of the injection site to apply light pressure for distraction. Pressure on the injection site with a cotton ball immediately after removing the needle also lessens the perception of pain.
Make it safe for you and your patient
- Keep everything aseptic – I know this is a no-brainer, but I couldn’t believe my eyes when I saw an injector palpating the injection site with a gloved hand before injecting on a TV video. In another news clip, the injector pushes the patient’s sleeve back from the target site immediately before injecting. I’m starting to wonder whether reporters are trying to find the worst examples of technique possible.
- Never recap a dirty needle; instead put it immediately into a sharps container – This is for your protection as well as your patient’s. Needle sticks happen all too often and can cause infection as well as inflict physical damage. I think this is basic knowledge (and reason to fail our injection course!), yet after my last flu shot, the injector carefully replaced the cap on the needle and placed it on the table. How do some of us forget these important things? It’s all in our human nature, I guess. Scientists describe the “curve of forgetting” where we gradually lose information we’ve learned if we don’t review it and no-one reminds us.
- Landmark every time – It seems very few injectors landmark, even though it is
Learn from mistakes
Some errors are due to lack of knowledge too, like the problem I had once when using a syringe with a pre-attached needle. I didn’t realize they could become loose during transport until, to my total horror, one came apart during an injection, leaving me with just the syringe in hand, the needle still in the patient’s arm and vaccine all over the place. I died a thousand deaths and, although the patient seemed to be OK with it all, I insisted that the injection plus its “re-do” were no charge! So, here’s a tip you might not have been taught: Always tighten the needle attachment if using a pre-assembled needle and syringe.
I’ve given thousands of injections that were perfect and almost pain-free, but it’s always the things that didn’t quite go right that stick in your memory, isn’t it. However, any error or near miss means your procedure needs to be improved or changed. We can never stop working toward improvement.
I’m a strong believer in learning from mistakes and sharing lessons learned so others can learn from them too. This is the premise behind the Institute for Safe Medication Practices (ISMP) – anonymous reporting and sharing of errors so all can learn and continually improve. If something goes wrong for one person, it could easily happen to another. Improving technique and policies must be a continuous effort for every health professional. If you’re not familiar with ISMP, check them out online at Ismp.org.
Jeannie Collins Beaudin is a recently retired Canadian community pharmacist with  40 years of experience, including specialization in compounding pharmacy, and hormone assessment and management. In addition to publishing her book, Can I Speak to the Hormone Lady? Managing Menopause and Hormone Imbalances in 2018, she has written articles and blogs for Pharmacy Practice + Business since 2006, peer reviewed educational programs for Canadian pharmacists since 1998 and publishes a weekly health blog found on her website.
40 years of experience, including specialization in compounding pharmacy, and hormone assessment and management. In addition to publishing her book, Can I Speak to the Hormone Lady? Managing Menopause and Hormone Imbalances in 2018, she has written articles and blogs for Pharmacy Practice + Business since 2006, peer reviewed educational programs for Canadian pharmacists since 1998 and publishes a weekly health blog found on her website.
Editor’s Note –The views expressed in the nurse influencer posts are those of the contributing authors. NPWH does not sanction the content of these posts.