
The American Urogynecologic Society’s best practice statement for the definition of recurrent urinary tract infection (rUTI) is at least two culture-proven episodes in 6 months, or at least three in 1 year.1 Nearly 60% of women will experience at least one urinary tract infection (UTI) in their lifetime, while 30% to 40% will experience rUTI. Women with rUTI are fearful of adverse effects related to antibiotics and frustrated when clinicians do not adhere to antibiotic stewardship protocols.2 Recurrent urinary tract infections are estimated to cost the United States over two billion dollars per year.3 To improve outcomes, it is prudent to understand how to implement strategies to decrease the incidence of rUTI. Multiple guidelines including the American Urologic Association (AUA), Canadian Urologic Association (CUA), Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU), American Urogynecologic Society, and several European guidelines summarized in the British Journal of Urology form the basis for this article. Recommendations for assessment, diagnosis, treatment, and prevention of rUTI are described.
Symptoms
Urinary tract infections can have a wide variety of symptoms. However, the distinguishing symptom in young women is the presence of painful urination. A UTI can be diagnosed with 90% accuracy if a young woman presents with dysuria in the absence of a vaginal infection. Urgency, frequency, suprapubic pain, and hematuria are variably present with UTI.1
Symptoms of UTI for older women may be more difficult to identify. Dysuria in the presence of new or worsening urinary incontinence is a common finding. The difficulty arises when individuals present with symptoms that are commonly chronic in older women such as vaginal burning, pelvic discomfort and/or pressure, urinary urgency and frequency, and urinary incontinence.1 Because of the chronic nature of these symptoms, it is recommended to refrain from evaluating for UTI unless the symptoms are acute (onset < 1 week) or associated with a fever.1
Risk factors
Multiple factors can increase a woman’s risk for rUTI. Common risk factors include sexual intercourse, use of spermicides, new sex partners, genetics, vaginal atrophy, urinary incontinence, pelvic organ prolapse, incomplete bladder emptying, and structural abnormalities. Structural abnormalities may include intraluminal disturbance including bladder stones, neoplasms, indwelling catheters, or stents. Other structural causes may include ureteral stenosis, strictures, or masses.4-6 Recurrent urinary tract infections related to structural abnormalities should be managed by a specialist.4
Women who engage in sexual intercourse four or more times per week are more likely to develop UTIs.4 Women also may have a predisposition to rUTI based on genetics. Blood group antigens secreted in body fluids characterize an individual’s “secretor status.” Those who secrete blood group antigens into body fluids are designated secretors and have an added level of protection against the environment in regard to microorganisms.7 Women with a nonsecretor vaginal epithelium have a higher risk for rUTI because two extended-chain glycosphingolipids are expressed, which in turn bind to pathogens more avidly, and increase the risk of infection.4 Secretor status is determined through DNA testing. Testing kits to the general population, however, are not commonly used in the clinical setting.7
Diagnosis
The gold standard for diagnosing a UTI remains a urine culture, a mainstay since the 19th century.8 Promising molecular research that could improve diagnosis is on the horizon. Whole genome and metagenomic sequencing technologies as well as a better understanding of the urinary tract microbiome may replace the current standard of practice in the future.6
The AUA, CUA, and SUFU developed a combined guideline for rUTI. The guideline defined rUTI as two or more culture-positive UTIs in 6 months or three culture-positive UTIs in 1 year.3 To follow the guideline, one must know how to interpret “culture-positive.” Based on multiple studies, the definition can be ambiguous.8 The most widely accepted definition of culture-positive is 105 colony forming units (CFU) per mL, which was published 60 years ago.8 Studies suggested the threshold of 105 CFU/mL reduced the over detection of contaminating organisms.8
The problem with the research is that data were taken from asymptomatic women. Several studies have demonstrated women with colony counts of less than 105 CFU/mL can present with pyuria and symptoms consistent with UTI. These studies suggest a 105 CFU/mL threshold for bacterial growth may help distinguish UTIs from contamination in asymptomatic, premenopausal women, but a lower threshold of 102 CFU/mL may be appropriate in symptomatic individuals.8
Clinicians should have a clear understanding of clinical laboratory protocols because certain laboratories may report 104 CFU/mL or less as “no growth.”1 It is recommended to obtain a repeat urine culture if the initial specimen is noted to be contaminated, and consideration should be given to a catheterized specimen.8 Utilization of molecular diagnostics is emerging in hopes of a more accurate diagnosis for UTI. However, due to the potential for overdiagnosis and misuse of antibiotics, the technology is not currently recommended for clinical use.6
Urinalysis can confirm the presence or absence of pyuria and is recommended with each symptomatic acute cystitis episode prior to initiating treatment.1 A urine dipstick can rule out a UTI, but it has little value to rule in a UTI. Urine dipstick testing is not advised because women with rUTI do not have a low pretest probability for UTI.1
Physical assessment
A physical examination is essential when diagnosing rUTI. The examination begins with the general appearance of the individual and proceeds with palpation for costovertebral angle and suprapubic tenderness. A pelvic examination follows and includes assessing the vulvar epithelia for tissue changes, urethral diverticulum, pelvic organ prolapse, abnormal vaginal discharge, pelvic masses, pelvic floor muscle tenderness, and bladder pain.1 In addition, foreign bodies such as a retained pessary or mesh erosion can be revealed by a thorough pelvic examination.1 A post-void residual can easily be performed at the time of physical examination to rule out urinary retention. Imaging studies are not generally recommended for diagnosing rUTI unless a urinary stone is suspected, there is rapid recurrence of the infection after appropriate treatment, or symptoms persist beyond 3 days despite proper treatment.1
Treatment
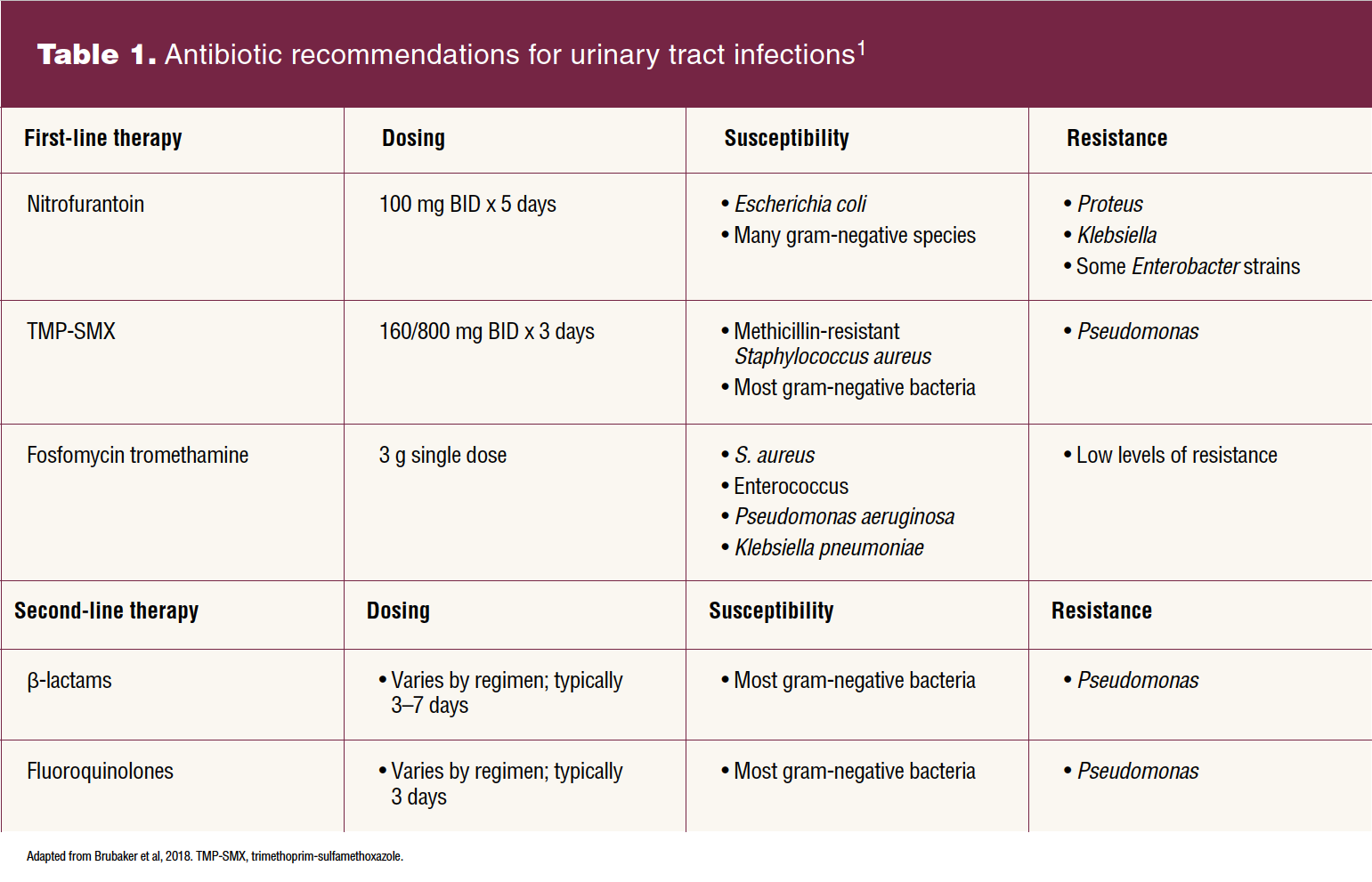
Symptomatic, culture-positive rUTI should be treated with the shortest course of first-line therapy (nitrofurantoin, trimethoprim-sulfamethoxazole [TMP-SMX], and fosfomycin) according to the local antibiogram. An antibiogram provides comprehensive information about local antimicrobial resistance and can be obtained from the local laboratory from where urine cultures are obtained.1,8
When first-line therapy is not an option, second-line therapy can be used. Second-line therapy includes β-lactams and fluoroquinolones. Caution must be taken when prescribing fluoroquinolones due to the increasing resistance patterns and serious adverse side effects.1,8
Parenteral antibiotics may be indicated when urine culture results demonstrate resistance. As with oral antibiotics, the shortest course of parenteral antibiotics is recommended at usually 7 days or less.8
Self-start therapy is an option for women who can reliably detect UTI symptoms, who are not candidates for long-term antibiotic prophylactic therapy, or who do not wish to take antibiotics long term.1 The clinician prescribes an antibiotic that will likely cover the uropathogen based on previous culture results. If symptoms are not resolved after 48 hours, it is recommended the woman contact the clinician for further guidance. Nitrofurantoin, TMP-SMX, and fosfomycin are the recommended antibiotics for self-start therapy and are dosed as defined in Table 1. Fluoroquinolones are not recommended for self-start therapy due to the increase in resistance and potential side effects.1 See Table 1 for antibiotic recommendations, dosing, susceptibility patterns, and resistance for UTI.
Prevention
Nonpharmacologic
Multiple guidelines exist for the management of rUTI. Although there is a general consensus with treatment and prophylaxis of rUTI using antibiotics, the guidelines vary significantly for nonpharmacologic prophylaxis options. Limited evidence exists for nonpharmacologic preventive measures, but due to growing concerns regarding antibiotic resistance, attention should be given to these options.3,9
Behavioral modifications include increased water intake (at least 1.5 L/day), wiping from front to back following defecation, postcoital voiding, not delaying urination, avoiding douching, avoiding spermicide use, and not wearing restrictive undergarments.3,8,9 Nearly all guidelines previously mentioned made a weak recommendation for implementing behavioral modifications.10 Regardless of the strength of evidence, it is acceptable to implement these modifications as no harm can be done to the individual.9
The use of cranberry for UTI prevention has been recommended for decades despite the lack of supporting data. The proanthocyanidins in cranberry are believed to prevent adherence of bacteria to the bladder wall. Available studies lack a standard cranberry formulation and dose. Nevertheless, the majority of guidelines make a weak recommendation for the use of cranberry tablets and/or cranberry juice for rUTI prevention.3,8 Given the high sugar content in juice, cranberry tablets may be a more desirable formulation.8 In similar fashion, D-mannose capsules or powder had weak recommendations at best for rUTI prevention.3,8,9
Lactobacillus is a bacteria naturally found in the digestive system, urinary tract, and other parts of the body. Because of growing concerns of antibiotic resistance, more attention has been given to lactobacilli probiotics. Studies utilizing both vaginal and oral lactobacilli have found no difference in the risk of developing a UTI. Therefore, all referenced guidelines agree there are insufficient data to recommend lactobacilli for prevention of rUTI.3,8,9
Nonantibiotic
Multiple studies have clearly demonstrated that the use of vaginal estrogen decreases the incidence of rUTI because the pH is restored to an acidic level favoring Lactobacillus colonization and discouraging pathogens.3,8,9 According to the AUA’s best practice statement, the benefits of vaginal estrogen for reducing rUTI are so evident that it should be recommended to all hypoestrogenic women who are good candidates.1
Methenamine hippurate, a salt of methenamine and hippuric acid, demonstrated evidence to decrease incidence of rUTI in a 2012 Cochrane review.9,10 Methenamine salts are taken as oral tablets and converted in the urine to ammonia and formaldehyde. The mechanism of action is believed to be bacteriostatic.11 Updated guidelines do not recommend methenamine hippurate for rUTI prophylaxis due to inadequate data, although larger studies may be promising for the future.8
Intravesical nonantibiotic instillations such as hyaluronic acid and chondroitin sulfate are believed to coat the urothelial surface and therefore create a barrier against Escherichia coli.8,9 The research is encouraging, although the guidelines do not currently recommend this therapy because of lack of adequate evidence.8
The use of vaccines may play an important role in the future for rUTI prevention.9,11 The goal of vaccines is to prime the immune response to pathogens, thus providing protection against infections such as rUTIs. Four different vaccine formulations exist for rUTI: oral and sublingual tablets, a vaginal suppository, and an intramuscular injection. Data are limited, but it is believed that vaccines may decrease the incidence of rUTI in the short term (< 6 months). Vaccines are not currently recommended for rUTI. Additional study of these vaccines with randomized controlled trials is needed to determine long-term efficacy and safety for infection prevention in patients with rUTIs.
Antibiotics
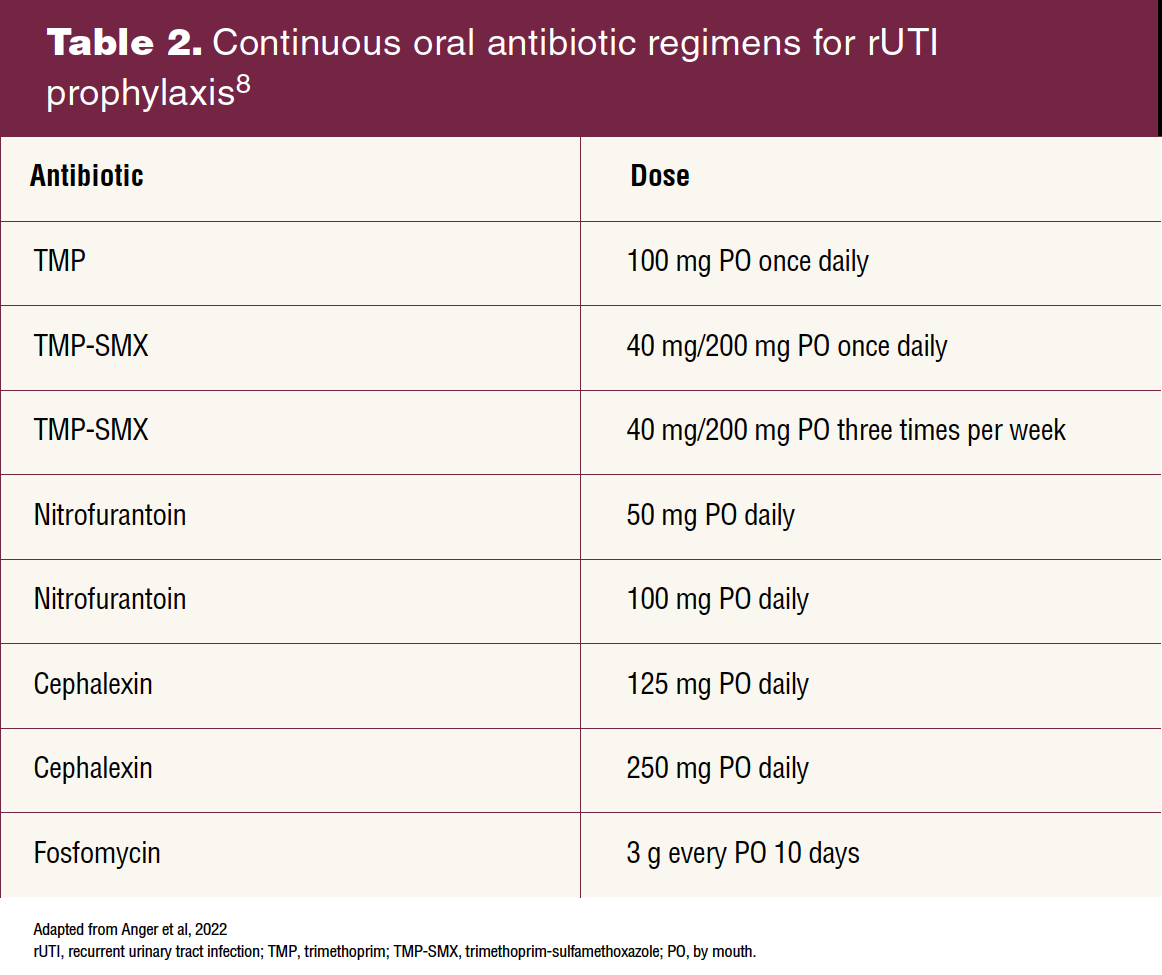
After discussing the benefits, risks, and alternative options with an individual, prophylactic antibiotics are an appropriate treatment option for women with rUTI.3,8,10 The duration of continuous oral antibiotics for prophylaxis in research ranges from 6 to 12 months. Daily prophylaxis beyond 6 months is uncommon, but treatment is often restarted due to recurrence of UTI. It is recommended to re-evaluate the use of daily antibiotics for prophylaxis after 3 months to determine efficacy.1 The following antibiotics are recommended for prophylaxis due to tolerability and low resistance: trimethoprim (TMP), TMP-SMX, nitrofurantoin, cephalexin, and fosfomycin.8 See Table 2 for continuous oral antibiotic dosing recommendations for rUTI prophylaxis.
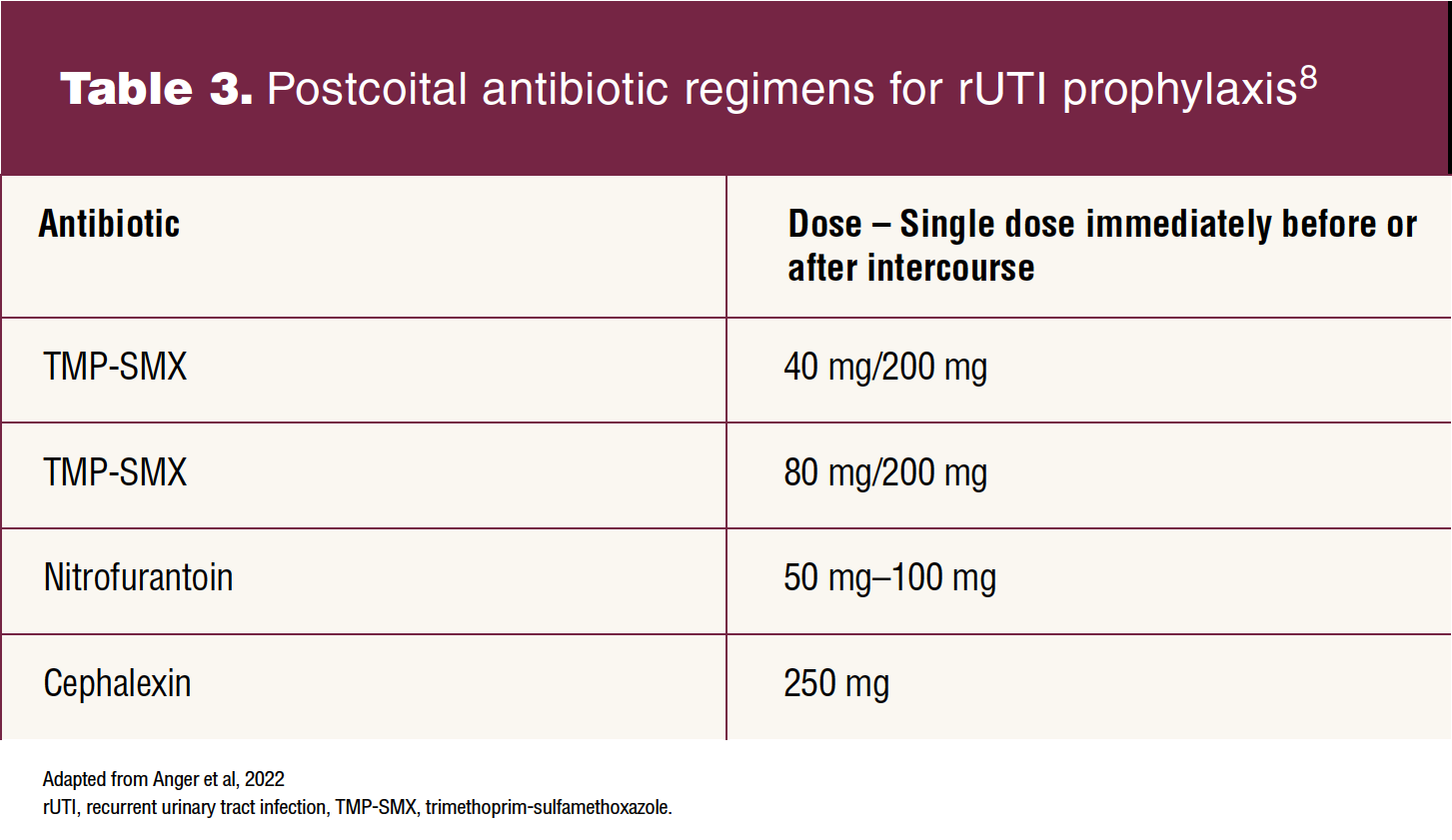
Some women suffer from rUTI related to sexual intercourse. Individuals often think this phenomenon is related to hygiene, although hygiene is usually not the culprit. One of the main reasons UTIs occur after intercourse is anatomic. The female urethra is short, so when bacteria residing around the anus are shifted toward the urethra with intercourse, the bacteria can easily ascend into the bladder.12 The guidelines recommend prophylactic antibiotics to be taken either before or after intercourse.8 One study confirmed that intermittent dosing was as effective as continuous daily antibiotic dosing for rUTI prophylaxis after intercourse.1 See Table 3 for postcoital antibiotic recommendations for rUTI prophylaxis.
Antibiotic bladder irrigations are not currently recommended but may provide some advantages over oral and/or parenteral routes. Intravesical instillations deliver the antibiotic directly to the site of infection. Bypassing the gastrointestinal tract decreases incidence of resistance and side effects. Gentamycin is the most studied antibiotic for this regimen and concentrations range from 40 mg to 80 mg of gentamycin in 50 mL of sterile water.1 Randomized controlled studies are not available, although reports on case series exist.1
One study included 68 individuals with rUTI. The dose of gentamicin used was 80 mg mixed with 20 mL of normal saline. The treatment regimen consisted of intravesical instillations daily for 2 weeks followed by every other day for 10 weeks and then twice weekly for 12 weeks (total, 24 weeks). The results of the case study demonstrated an 80% reduction in UTI during intravesical treatment and a 55% decrease in resistance rate of uropathogens. Elevations of serum gentamicin levels were not detected.13 Clinicians may consider this therapy for select individuals based on the limited evidence available.
Antimicrobial stewardship
Concerns related to antimicrobial resistance and potential side effects from oral antibiotics have brought awareness to antibiotic stewardship protocols. Antibiotic stewardship protocols can help reduce inappropriate antibiotic treatment, decrease broad-spectrum antibiotic use, and modify treatment to the shortest effective duration, thereby decreasing the incidence of fluoroquinolone and cephalosporin resistance.8 Unfortunately, nonadherence to these protocols is more common in individuals with rUTI than those with an isolated UTI. Clinicians treating symptomatic rUTI must routinely obtain urine cultures to avoid overtreatment and assist with appropriate antibiotic treatment choice.3,8
Asymptomatic bacteriuria (ASB) represents another challenge in antimicrobial stewardship. ASB is the presence of bacteria in a urine specimen from an individual without symptoms of a UTI.8 The guidelines strongly recommend not treating ASB in nonpregnant women. Additionally, routine urine cultures in asymptomatic patients with rUTI are not recommended.3,8 It is prudent that clinicians recognize ASB and adhere to antimicrobial stewardship protocols. Asymptomatic bacteriuria can be confusing for individuals, or they may insist treatment is necessary. Therefore, patient education about inappropriate use of antibiotics is essential.3,8
Referral
Instances occur when the situation is beyond the routine practice for the women’s health nurse practitioner in a primary care setting. Such instances include abnormal genitourinary anatomy, concern for obstruction, chronic catheterization, suspicion for malignancy, pyelonephritis, and immunosuppression. In these situations, the patient should be referred to a urologist for advanced imaging and/or studies such as cystoscopy, renal ultrasound, and computed tomographic urography.1
Practice implications
Women’s health nurse practitioners play a key role in the identification and management of rUTI. Timely diagnosis and treatment can decrease the incidence of inappropriate antibiotics and lower the risk of antibiotic resistance. Early detection of rUTI also can expedite referrals to specialists when indicated.8 Educating individuals about preventive strategies can alleviate fears and frustration among women who suffer from rUTI. Fortunately, best practice recommendations are constantly being updated to reflect current research. It is imperative to keep abreast of the current guidelines so that the most appropriate and safe management approach is implemented.
Kendra L. Roloff is a certified women’s health and urology nurse practitioner at Pelican Health in Bismarck, North Dakota. The author has no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(1):17-22. doi: 10.51256/WHC022317
Key words: recurrent urinary tract infection, urinary tract infection, asymptomatic bacteriuria, antibiotic stewardship, antibiotics, dysuria
References
1 Brubaker L, Carberry C, Nardos R, et al. American Urogynecologic Society best-practice statement: recurrent urinary tract infection in adult women. Female Pelvic Med Reconstr Surg. 2018;24(5):321-335.
2 Scott VCS, Thum LW, Sadun T, et al. Fear and frustration among women with recurrent urinary tract infections: findings from patient focus groups. J Urol. 2021;206(3):688-695.
3 Anger J, Lee U, Ackerman AL, et al. Recurrent uncomplicated urinary tract infections in women: AUA/CUA/SUFU guideline. J Urol. 2019;202(2):282-289.
4 Storme O, Tirán Saucedo J, Garcia-Mora A, et al. Risk factors and predisposing conditions for urinary tract infection. Ther Adv Urol. 2019;11:19-28.
5 Aggarwal N, Lotfollahzadeh S. Recurrent urinary tract infections. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2022 Jan-. Updated August 24, 2022. https://www.ncbi.nlm.nih.gov/books/NBK557479/.
6 Jung C, Brubaker L. The etiology and management of recurrent urinary tract infections in postmenopausal women. Climacteric. 2019;22(3):242-249.
7 D’Adamo P. The importance of your secretor status (secretor or non-secretor). Body and Mind Studio International. March 8, 2017. https://bodyandmindstudio.co.uk/helpful-articles/the-importance-of-your-secretor-status-secretor-or-nonsecretor/.
8 Anger J, Lee U, Ackerman L, et al. Recurrent uncomplicated urinary tract infections in women: AUA/CUA/SUFU guideline. American Urological Association. 2022. https://www.auanet.org/guidelines-and-quality/guidelines/recurrent-uti.
9 Sihra N, Goodman A, Zakri R, et al. Nonantibiotic prevention and management of recurrent urinary tract infection. Nat Rev Urol. 2018;15(12):750-776.
10 Kwok M, McGeorge S, Mayer-Coverdale J, et al. Guideline of guidelines: management of recurrent urinary tract infections in women. BJU Int. 2022 May 17. Online ahead of print.
11 Prattley S, Geraghty R, Moore M, Somani BK. Role of vaccines for recurrent urinary tract infections: a systematic review. Eur Urol Focus. 2020;6(3):593-604.
12 WebMD Editorial Contributors. Urinating after sexual intercourse to prevent urinary tract infections. April 19, 2021. Accessed December 4, 2022. https://www.webmd.com/sex/urinating-after-sexual-intercourse-to-prevent-urinary-tract-infection
13 Stalenhoef JE, van Nieuwkoop C, Menken PH, et al. Intravesical gentamicin treatment for recurrent urinary tract infections caused by multidrug resistant bacteria. J Urol. 2019;201(3):549-555.