
Cardiovascular disease (CVD) is the leading cause of death in women in the United States. About 1 in 3 women will die from CVD, and about 45% of women older than age 20 years will show evidence of cardiovascular disease. Professional organizations such as the American Heart Association, American College of Cardiology, and the American College of Obstetricians and Gynecologists have begun efforts to explore links between the development of CVD in women and the occurrence of adverse pregnancy outcomes (APO). This article explores the current understanding of this linkage and discusses strategies to increase provider and patient knowledge, and risk mitigation for women with APO.
Cardiovascular disease (CVD), including coronary artery disease and stroke, is the leading cause of death in women in the United States.1,2 Approximately 1 in 3 women will die from CVD, and a staggering 45% of women older than age 20 years demonstrate some form of cardiovascular disease.3 Evidence suggests a link between adverse pregnancy outcomes (APO) and CVD development primarily related to hypertensive disorders of pregnancy (HDP).3 The incidence of HDP rose by 25% over the last decade, identifying this problem as a significant health concern to be addressed by women’s healthcare providers.4 There is a 20% to 40% increased risk of CVD after the experience of preeclampsia that cannot be attributed to traditional risk factors such as obesity and smoking.5 Researchers suggest that HDP may uncover future cardiovascular risk.6
In addition to HDP, other APO are being considered as having potential links to CVD. This article discusses hypotheses about the underlying mechanisms for the association between APO and CVD, identifies several APO with potential links to CVD, and suggests strategies to optimize women’s cardiovascular health following APO.
Increased Risk of Adverse Pregnancy Outcomes in Women with Psoriasis: Study
Pregnancy With Infertility Treatments May Increase Risk of Vascular Complications
Antihypertensive Drugs Safe During Pregnancy, AHA Says
Physiologic changes of normal pregnancy
Many cardiometabolic changes occur in normal pregnancy. Early in pregnancy, cardiac output (CO) increases by about 10% over prepregnancy values, along with an increase in maternal heart rate. Plasma volume expands by 40% to 50%.6 Changes in clotting factors occur to guard against excessive blood loss during the birth process.6 Increased proclotting factors, endothelial alterations, and reduced fibrinolysis are further protective changes.6–9
By the end of the second trimester, increased insulin resistance from the secretion of human placental lactogen and human chorionic somatomammotropin alters metabolism, providing more glucose to the developing fetus.2,6,7 Pregnancy also promotes lipid changes to provide a ready source of nutrients for the growing fetus. Changes in triglycerides, total cholesterol, and both high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol promote fat storage for use during pregnancy, facilitate steroid hormone production, and later promote lactation through about 12 weeks’ postpartum.10
Maternal renal system alterations result in higher glomerular filtration rates and reduced serum creatinine levels. There is diminished sensitivity to some vasoconstrictors and an increased renal permeability resulting in more protein excretion in normal pregnancy.11
There is some supposition that underlying conditions that promote the risk for development of future CVD may be revealed with strain from usual physiologic changes of pregnancy.6 It is unclear whether the increased risk of CVD results from maladaptation to the typical changes of pregnancy, identifies some predisposition to future CVD that precedes pregnancy, or some combination of both.4
Underlying mechanisms by which APO may be linked to future CVD
Researchers debate how APO contribute to CVD development but note they may share pathologic pathways.2 The underlying mechanism of several APO (eg, preeclampsia, gestational diabetes mellitus, preterm birth, small for gestational age birthweight, stillbirth) is generally considered to be placental and/or vascular dysfunction.12 There is some evidence, most specifically related to preeclampsia, to suggest the associated CVD risk later in life may be preceded by acute placental atherosis similar to that seen in atherosclerosis. Acute placental atherosis may contribute to inflammatory changes and long-term endothelial dysfunction that plays an important role in future CVD development.2,13
Hypertensive disorders of pregnancy
All hypertensive disorders of pregnancy (HDP) categories have significantly increased over the last 10 years, occurring in up to 10% of US pregnancies.1,4,6 It is estimated that 4% to 8% of US mothers have at least one pregnancy complicated by preeclampsia.14 Approximately 3% to 5% of pregnancies are complicated by chronic hypertension (CHTN), defined as hypertension occurring or recognized before 20 weeks of gestation or persisting beyond 12 weeks’ postpartum. Women with any category of HDP are at risk of developing CHTN within a year of giving birth, hospitalization for a cardiovascular event within 3 years after giving birth, and are more likely to develop diabetes and dyslipidemia.3 Research strongly links early development of CVD to HDP occurrence.4 Women with HDP have a 2- to 4-fold higher risk of future CVD compared with women who have not experienced HDP.3,6,10 Proinflammatory risk factors such as obesity, sedentary lifestyle, poor diet, and smoking further contribute to future CVD, but the experience of HDP is independent of those risk factors.5
Gestational diabetes
Gestational diabetes (GDM) occurs in about 7% of pregnancies in the US, but it is rising due to worsening obesity, sedentary lifestyles, and increases in maternal age and comorbidities. Physiologic increased insulin resistance during pregnancy may be a tipping point for women on the brink of overt diabetes as the pancreas cannot keep pace with this high insulin resistance. Research suggests women with GDM have up to a 4-fold risk of developing preeclampsia and a 2-fold risk of future CVD, with cardiac events demonstrated about 7 years earlier than in women with nonaffected pregnancies.2,4,6,13 After a pregnancy complicated by GDM, there is a 7-fold higher risk of developing type 2 diabetes.2
Placental abruption
The etiology for placental abruption is unclear but believed to be associated with abnormal placentation, endothelial dysfunction, and capillary fragility from proinflammatory changes that predispose to necrosis and infarction.15 Abruption occurs in about 1% of pregnancies.16 Maternal hypertension is the most common risk factor, accounting for about 44% of all abruptions.17 Other risk factors include advanced maternal age, cocaine use, cigarette smoking, and trauma.17,18 A history of placental abruption was significantly associated with future CVD-related morbidity and mortality in a meta-analysis of four studies. Of note, none of the studies examined whether the effect of placental abruption was independent of hypertension.18
Preterm birth
Birth before 37 completed weeks’ gestation is considered preterm birth (PTB) and occurs in about 10% of pregnancies. This may be caused by intrauterine infection or iatrogenic when obstetric complications make delivery necessary.2 PTB is an independent risk factor for future CVD, increasing risk by about 42% and doubling CVD risk if occurring concomitantly with HDP.2,16
Other
Various studies have called attention to other potential APO that could increase the risk for CVD in the future. These include birth of a small for gestational age infant, stillbirth, and loss of pregnancy.16,18 Ongoing research is needed to discern the connection between the pathophysiology of APO and CVD risk. However, with current knowledge there are specific strategies for healthcare providers to help women improve their CV health and reduce their CVD risk.
Mitigating future CVD risk
Disparities
Women in the US display many traditional cardiovascular risk factors including hypertension, obesity, diabetes, and sedentary lifestyle, but significant racial and ethnic disparities exist. Black women have a higher rate of hypertension than their White and Hispanic counterparts, while the incidence of diabetes is higher among Hispanic women. More overweight and obese women are found among Black and Hispanic women than among White women.16 Further, Black, Hispanic, and Asian women experience a higher proportion of APO associated with increased CVD risk than non-Hispanic White women.16,17 Clinical presentations and outcomes are commonly more severe. The reason for these disparities is not fully understood. Inequalities in access to prenatal care and disparities in other prepregnancy risk factors have been proposed as causative but not proven. More studies on APO and CVD in non-White women evaluating the effects of social determinants of health such as violence against women, access to care, and available technologies are needed to better understand and address these health disparities.16,18,19 Structural racism and bias with ensuing psychological stress should be considered.
Create opportunities for patient-centered communication
After pregnancies complicated by an APO, women commonly describe a lack of consistent messaging and poor communication about future CVD risk and believe their concerns were dismissed by providers.3,5,16 Frank patient–clinician discussion of previous pregnancy complications, current lifestyle behaviors, and relevant family history risk factor identification is recommended. An interdisciplinary approach with seamless communication among all providers, including obstetricians, maternal–fetal medicine specialists, primary care providers such as women’s health nurse practitioners, and cardiologists is necessary for risk mitigation. Comprehensive obstetric histories, including the occurrence of APO, must be collected, and maintained, which may improve care for women at an increased risk of CVD.7
Screen for a history of APO
Key to identifying women who may be at increased risk for CVD is screening for APO, utilizing every point of contact as an opportunity. Although there is no consensus on when and how to screen, developing strategies for targeted risk screenings may avoid delayed or missed recognition and promote chances to mitigate CVD risk.2,20,21 Screening opportunities include prepregnancy counseling, early pregnancy visits, and postpartum and well-woman exams.
Encourage lactation
Encouraging lactation promotes better cardiometabolic status by reducing blood glucose levels and insulin resistance. Lipid improvements, including increases in HDL, occur during lactation and result in less early atherosclerosis.10,15 While there is limited evidence that lactation influences CVD risks factors specifically among women who experience APO, it seems plausible given the positive effects on the general population. The American Heart Association and the American College of Obstetricians and Gynecologists (ACOG) make the recommendation to encourage women with APO to continue lactation beyond 6 months.16,21
Improve lifestyle choices after APO
Timely and practical strategies to facilitate behavioral change are critical for reducing the risk of future CVD. Providers can encourage women to optimize health with a focus on reducing major modifiable risk factors. Making more heart-healthy dietary choices, such as implementing the DASH diet [Dietary Approaches to Stop HTN] or the Mediterranean diet and adopting a more active lifestyle to include 20 to 30 minutes of moderately intense activity most days reduce CVD risk.2,10,15
On the one hand, postpartum women may be motivated to adopt healthy lifestyles especially after experiencing an APO. Promoting patient use of resources from the Preeclampsia Foundation and HeartHealth4Mom may empower women to make healthy choices.5,7,21 Telehealth visits and cell phone-based risk reduction and support programs may be useful for patient education and motivation and alleviate postpartum scheduling difficulties.
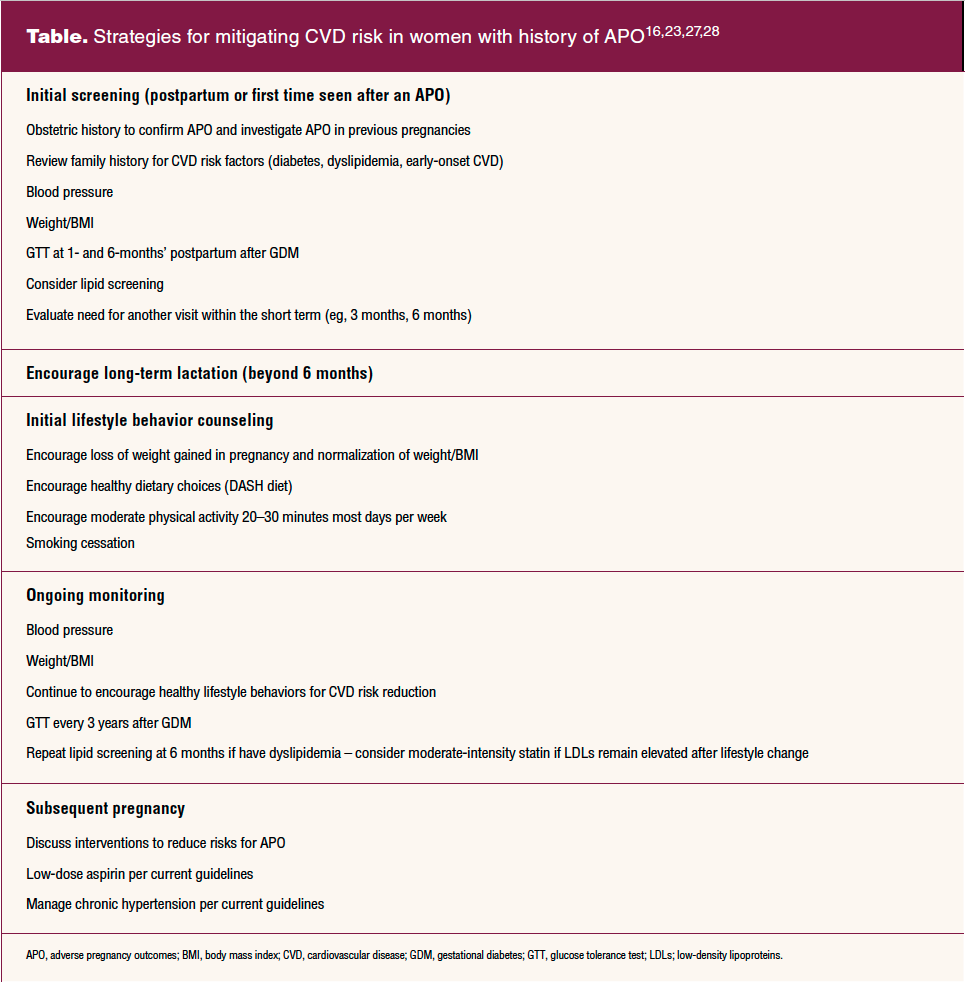
On the other hand, up to 40% of women do not attend a postpartum visit.21 These are often women with limited resources. Providers will want to remain cognizant that the initial opportunity to address risks associated with an APO may not be postpartum but at another visit along the way. The Table provides recommendations for initial screening, monitoring over time, and lifestyle counseling interventions for women identified as having had an APO.
Promote use of low-dose aspirin when indicated
The 2021 recommendations from ACOG, the Society of Maternal–Fetal Medicine, and the United States Preventive Services Task Force (USPSTF) suggest women with one or more high-risk factors for preeclampsia or more than one moderate risk factors should begin 81 mg aspirin at 12 weeks’ gestation and continue until birth occurs.3,16,18 Moderate risk factors include nulliparity, body mass index greater than 30, age older than 35 years, non-Hispanic Black race, or lower income. Factors indicating high risk include the history of preeclampsia, CHTN, pregestational diabetes, and renal or autoimmune disease. USPSTF separated sociodemographic risk factors to the Black race and having lower income, acknowledging that non-Hispanic Black women experience earlier onset, more severe, and higher incidence of APO.19 Low-dose aspirin improves placentation and helps with spiral artery remodeling, generally completed by 18 weeks of gestation.7,22
Manage chronic hypertension in pregnancy
A 2022 ACOG practice advisory suggests aggressive treatment of CHTN in pregnancy, starting or modifying medication management at 140/90 mm Hg rather than 160/110 mm Hg as previously recommended, and allowing patients to remain on current blood pressure medications as long as they are considered safe.23 The California Maternal Quality Care Collaborative (CMQCC) provides a tool kit to support timely recognition and response to hypertension and preeclampsia. Guidance on low-dose aspirin for prevention of preeclampsia and long-term follow-up after hypertensive disorders of pregnancy is included.24 The Alliance for Innovation on Maternal Health (AIM) produces safety bundles for in- hospital management of severe hypertension. AIM bundles include information on provider recognition and prevention of severe hypertension during pregnancy, which is helpful for antepartum providers.25
Use statins when appropriate
In nonpregnant women with dyslipidemia, statin therapy decreases inflammation and oxidative stress and provides endothelial protection. Statins additionally protect through inhibiting abnormal clotting mechanisms and promotion of angiogenesis.3,7 Current guidelines recommend stopping statin therapy 1 to 3 months before attempting pregnancy or as soon as pregnancy is confirmed.2,3 Healthy lifestyle habits should be encouraged for management of dyslipidemia during pregnancy. Bile sequestrants are approved for use during pregnancy. Human trials are under way to determine the safety of hydrophilic statin use during pregnancy, particularly pravastatin because of a better safety profile in pregnancy.7,26
Future research
There are several directions for future study. More research is needed to identify timely targeted screening strategies after APO. We must continue to study the potential use of hydrophilic statins during pregnancy combined with careful fetal growth monitoring. The impact of traumatic pregnancy and delivery experiences on mental health due to APO must be explored to reduce emotional trauma, which is known to increase oxidative stress and inflammation leading to endothelial and immune dysfunction, heightening CVD risk.3
Carolyn L. Bottone-Post is an Associate Professor at the School of Nursing University of Northern Colorado in Greeley. The author has no actual or potential conflicts of interest in relation to the contents of this article.
Key words: hypertension, preeclampsia, gestational diabetes, preterm birth, cardiovascular disease, adverse pregnancy outcomes
Womens Healthcare. 2022;10(6):19-24. doi: 10.51256/WHC122219
References
1 Centers for Disease Control. Hypertensive disorders in pregnancy and mortality at delivery hospitalization: United States, 2017-2019. 2022. https://www.cdc.gov/mmwr/volumes/71/wr/mm7117a1.htm.
2 Hauspurg A, Ying W, Hubel CA, Michos ED. Adverse pregnancy outcomes and future cardiovascular disease. Clin Cardiol. 2018 41(2):239-246.
3 Cho L, Davis M, Elgendy I, et al. Summary of updated recommendations for primary prevention of cardiovascular disease in women: JACC state-of-the-art review. J Am Coll Cardiol. 2020;75(20):2602-2618.
4 Benschop L, Duvekot JJ, Roeters van Lennep JE. Future risk of cardiovascular disease risk factors and events in women after a hypertensive crisis. Heart. 2019;105(16):1273-1278.
5 Seely EW, Celi AC, Chausmern J, et al. Cardiovascular health after preeclampsia: patient and provider perspective. Womens Health Rep (New Rochelle). 2020;30(3):305-313.
6 American College of Obstetricians and Gynecologists. Practice bulletin no. 212: pregnancy and heart disease. Obstet Gynecol. 2019;133(5):e320-e356.
7 Park K, Minissian MB, Wei J, et al. Contemporary clinical updates on the prevention of future cardiovascular disease in women who experience adverse pregnancy outcomes. Clin Cardiol. 2020;43(6):553-559
8 Babker AM, Elnaim EOD. Hematological changes during all trimesters in normal pregnancy. J Drug Delivery Ther. 2020;10(2):1-4.
9 Devis P, Knuttinenn MG. Deep venous thrombosis in pregnancy: incidence, pathogenesis and endovascular management. Cardiovasc Diagn Ther. 2017;7(suppl 3):S309.
10 Waage CW, Mdala I, Stigum H, et al. Lipid and lipoprotein concentrations during pregnancy and associations with ethnicity. BMC Pregnancy Childbirth. 2022;22(1):1-12.
11 Gonzalez Suarez ML, Kattah A, Grande JP, Garovic V. Renal disorders in pregnancy: core curriculum 2019. Am J Kidney Dis. 2019;73(1):119-130.
12 Lane-Cordova A, Khan S, Grobman W, et al. Long-term cardiovascular risks associated with adverse pregnancy outcomes. J Am Coll Cardiol. 2019;(16):2106-2116.
13 Pitz Jacobsen D, Fjeldstad HE, Johnsen GM, et al. Acute atherosis lesions at the fetal-maternal border: current knowledge and implications for maternal cardiovascular health. Front Immunol. 2021;12:791606.
14 Rich-Edwards JW, Stuart JJ, Skurnik, G, et al. Randomized trial to reduce cardiovascular risk in women with recent preeclampsia. J Womens Health. 2019.1493-1504.
15 Garovic VD, Dechend R, Easterling T, et al. Hypertension in pregnancy: diagnosis, blood pressure goals, and pharmacotherapy: a scientific statement from the American Heart Association. Hypertension. 2022;79(2):e21-e41.
16 Parikh NI, Gonzalez JM, Anderson CA, Judd SE; American Heart Association Council on Epidemiology and Prevention; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Cardiovascular and Stroke Nursing; and the Stroke Council. Adverse pregnancy outcomes and cardiovascular disease risk: unique opportunities for cardiovascular disease prevention in women: a scientific statement from the American Heart Association. Circulation. 2021;143(18):e902-e916.
17 Deering SH. Abruptio Placentae. Medscape. Updated November 30, 2018. Accessed June 7, 2022.
18 Grandi SM, Filion KB, Yoon S, et al. Cardiovascular disease-related morbidity and mortality in women with a history of pregnancy complications: systematic review and meta-analysis. Circulation. 2019;139(8):1069-1079.
19 Wenger NK, Lloyd-Jones DM, et al. Call to action for cardiovascular disease in women: Epidemiology, awareness, access, and delivery of equitable health care. Circulation. 2022;145e:1059-1071.
20 Ford ND, Robbins CL, Nandi N, et al. Clinician knowledge and practices related to a patient history of hypertensive disorders of pregnancy. Obstet Gynecol. 2022;139(5):898-906.
21 American College of Obstetricians and Gynecologists. Committee opinion no. 736. Optimizing postpartum care. Obstet Gynecol. 2018;131(5):e140-e150.
22 American College of Obstetricians and Gynecologists. Clinical practice advisory. 2021. https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2021/12/low-dose-aspirin-use-for-the-prevention-of-preeclampsia-and-related-morbidity-and-mortality.
23 American College of Obstetricians and Gynecologists. Clinical practice advisory. 2022. https://www.acog.org/clinical/clinical-guidance/practice-advisory/articles/2022/04/clinical-guidance-for-the-integration-of-the-findings-of-the-chronic-hypertension-and-pregnancy-chap-study.
24 California Maternal Quality Care Collaboration (CMQCC). Hypertensive disorders of pregnancy toolkit. 2021. https://www.cmqcc.org/resources-tool-kits/toolkits/HDP.
25 Alliance for Innovation on Maternal Health. Severe hypertension in pregnancy. 2020. https://safehealthcareforeverywoman.org/council/patient-safety-bundles/maternal-safety-bundles/severe-hypertension-in-pregnancy-aim/.
26 Chang JC, Chen YJ, Chen IC, et al. Perinatal outcomes after statin exposure during pregnancy. JAMA Netw Open. 2021;4(12):e2141321-e2141321.
27 Poon LC, Shennan A, Hyett JA, et al. The International Federation of Gynecology and Obstetrics (FIGO) initiative on pre-eclampsia: a pragmatic guide for first-trimester screening and prevention [published correction appears in Int J Gynaecol Obstet. 2019;146(3):390-391]. Int J Gynaecol Obstet. 2019;145(suppl 1):1-33.
28 Brown MA, Magee LA, Kenny LC, et al. Hypertensive disorders of pregnancy: ISSHP classification, diagnosis, and management recommendations for international practice. Hypertension. 2018;72(1):24-43.