
Faculty: Nicole L. Bort, DNP, AGPCNP, DCNP, is a dermatology nurse practitioner and Director of Nurse Practitioner Post-Graduate Training Program at the University Hospitals of Cleveland Medical Centers in Cleveland, Ohio.
Intended audience: This continuing education (CE) activity has been designed to meet the educational needs of nurse practitioners and other healthcare providers who provide primary care for women.
CE approval period: Now through February 28, 2024
Estimated time to complete this activity: 1 hour
CE approval hours: 1.0 contact hour of CE credit including 0.25 contact hours of pharmacology content
Goal statement: Nurse practitioners and other healthcare providers who provide primary care for women will increase their knowledge about the diagnosis of hidradenitis suppurativa (HS), pharmacologic management, and potentially helpful lifestyle modifications.
Needs assessment: Nurse practitioners who provide primary care for adolescent and adult women often encounter dermatologic conditions. Hidradenitis suppurativa is one such condition that affects women three times more than men. This chronic, often debilitating skin disorder frequently goes undiagnosed and can have a significant effect on quality of life as the individual suffers with pain, embarrassment, and frustration. Knowledge about signs/symptoms for HS is needed for earlier diagnosis so that evidence-based management can be implemented.
Educational objectives: At the conclusion of this educational activity, participants should be able to:
- Identify signs/symptoms and appropriate evaluation for the diagnosis of HS.
- Describe indications, mechanism of action, efficacy, adverse effects, and contraindications for pharmacologic options in treating HS.
- Discuss lifestyle modifications that may ease exacerbation of HS.
Accreditation statement: This activity has been evaluated and approved by the Continuing Education Approval Program of the National Association of Nurse Practitioners in Women’s Health (NPWH) and has been approved for 1 contact hour CE credit, including 0.25 hours of pharmacology credit.
Faculty disclosures: NPWH policy requires all faculty to disclose any affiliation or relationship with a commercial interest that may cause potential, real, or apparent conflict of interest with the content of a CE program. NPWH does not imply that affiliation or relationship will affect the content of the CE program. Disclosure provides participants with information that may be important to their evaluation of an activity.
Nicole L. Bort, DNP, AGPCNP, DCNP, has no actual or potential conflicts of interest in relation to the contents of this article.
Disclosure of unlabeled/unapproved use: NPWH policy requires authors to disclose to participants when they are presenting information about unlabeled use of a commercial product or device or an investigational use of a drug or device not yet approved for any use.
Disclaimer: Participating faculty members determine the editorial content of the CE activity; this content does not necessarily represent the views of NPWH. This content has undergone a blinded peer review process for validation of clinical content. Although every effort has been made to ensure that the information is accurate, clinicians are responsible for evaluating this information in relation to generally accepted standards in their own communities and integrating the information in this activity with that of established recommendations of other authorities, national guidelines, and FDA-approved package inserts, and individual patient characteristics.
Successful completion of the activity: Successful completion of this activity, J 22-01, requires participants to do the following:
- “Sign in” at the top right-hand corner of this page if you have an NPWH account. You must be signed in to receive credit for this course. If you do not remember your username or password, please follow the “Forgot Password” link and instructions on the sign in page. If you do not have an account, please click on “Create an Account.”
- Read the learning objectives, disclosures, and disclaimers on the next page and then click on the “Continue” button.
- Study the material in the learning activity during the approval period (now through February 28, 2024).
- Complete the post-test and evaluation. You must earn a score of 70% or higher on the post-test to receive CE credit.
- Print out the CE certificate after you have successfully passed the post-test and completed the evaluation.
*If you are an NPWH member, were once a member, or have completed CE activities with NPWH in the past, you have a username and password in our system. Please do not create a new account. Creation of multiple accounts could result in loss of CE credits as well as other NPWH services. If you do not remember your username or password, either click on the “Forgot Username” or “Forgot Password” link or call the NPWH office at (202) 543-9693, ext. 1.
Commercial support: This activity did not receive any commercial support.
Hidradenitis suppurativa (HS) is a chronic, often debilitating, inflammatory skin disease that presents with painful abscesses, nodules, sinus tracts, and scarring to intertriginous areas that frequently goes undiagnosed. Treatment options are influenced by disease severity and include both medical and surgical interventions. The chronicity of HS can lead to destructive impact on patients’ quality of life as they often suffer from pain, embarrassment, frustration, and multiple comorbidities. This article highlights the main features and treatment options available for HS to help expand disease awareness.
Nurse practitioners (NPs) who provide primary care for adolescent and adult women often encounter dermatologic conditions. One such condition is hidradenitis suppurativa (HS). It is a chronic inflammatory condition of the hair follicles that can have profound and often debilitating effects on an individual’s quality of life. The disease consists of painful, persistent, inflammatory nodules and abscesses located in intertriginous sites that can lead to tunneling sinus tracts and scarring. It is often unrecognized by healthcare providers, leading to delays in diagnosis. Evidence shows that the mean delay in diagnosis for HS was more than 10 years and more than 60% of patients had visited a healthcare provider more than five times before receiving a formal diagnosis.1 The reasons for delays in diagnosis are not completely clear but are likely as complex as the disease itself.
Individuals with HS silently endure the enormous physical and emotional suffering that follows an unpredictable course of flares and quiescence. It can result in permanent scarring, is associated with several comorbidities, and frequently has a psychosocial sequela. This article addresses the assessment and management of HS to equip NPs with knowledge for timely diagnosis and initiation of appropriate treatment.
Epidemiology and pathogenesis
The prevalence of HS ranges from 0.05% to 4.1% with varying degrees of severity, but true prevalence may be higher due to underreporting or delays in accurate diagnosis.2 Women are affected three times more than men.3 Onset is typically somewhere between puberty and the fourth decade of life. There is a greater likelihood of HS in patients who are of African descent, obese, smokers, have Down syndrome, or those with a low socioeconomic status.1,4,5
The etiology of HS is not entirely understood. It was originally believed to be associated with apocrine gland dysfunction, but current data have linked a complex interplay of events originating from follicular occlusion in addition to being reported in individuals who are likely genetically predisposed. The occluded follicle eventually ruptures, which leads to a cascade of inflammatory responses and the development of painful nodules and abscesses. It is important to know that while bacteria can sometimes play a role, this is not an infectious disease, but rather an inflammatory dermatosis. Genetics, hormonal changes, obesity, and smoking may also play a role. Environmental factors like heat, sweat, friction, and physical exertion have all been attributed to a worsening of the condition.
Clinical presentation and diagnosis
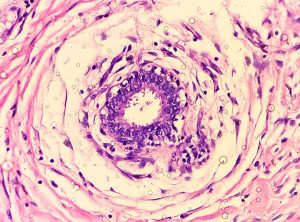
The presentation of HS is variable, ranging from mild inflammatory lesions to painful, indurated papules, nodules, abscesses, scarring, or tract formation. Distribution is oftentimes symmetric and can occur in the axilla, inframammary area, medial thighs, inguinal folds, perineum, or anogenital area. Patients often describe these lesions as “boils.” As the abscesses repeatedly heal and reemerge, the skin can develop permanent tunnels (known as sinus tracts) between the skin surface and the abscess. Lesions can form with or without sinus tract formation, scarring, or malodorous drainage. The hallmark sign is a double-headed comedone that appears as multiple blackheads within one single follicle. The degree of disease severity is what guides evidence-based treatment options and is classified based on the Hurley staging system.2
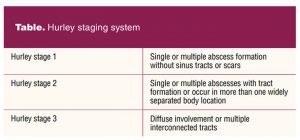
Clinical diagnosis is typically made with visual inspection in the presence of recurrent, characteristic lesion(s) in one or more of the characteristic locations. Differential diagnoses include furuncles, carbuncles, folliculitis, epidermal cysts, infected Bartholin’s gland, or cutaneous presentation of Crohn’s disease. It is important to remember that HS is not an infectious process, so bacterial cultures are not helpful for diagnosis unless being utilized to exclude a differential diagnosis. Single lesions without evidence of tracts or scars are considered the mildest form of the disease known as Hurley stage 1. The presence of scarring, sinus tract formation, or if lesions exist in more than one body location is classified as Hurley stage 2. The presence of diffuse involvement either in one or multiple body locations with evidence of interconnected tracts and scarring results in a disease severity escalating it to Hurley stage 3 (Table).
Associated disorders
A variety of underlying or concomitant conditions are associated with HS including polycystic ovary syndrome, inflammatory bowel disease, nodulocystic acne, metabolic syndrome, and squamous cell carcinoma.4 In a recent analysis, HS patients were shown to have twice the overall comorbidity burden when they were compared to those who did not have HS.1 Screening for blood pressure, body mass index (BMI), complete blood count, complete metabolic profile, fasting glucose, and glycosylated hemoglobin type A1c should be done at least annually.4 If any signs of hyperandrogenism are present, DHEAS [dehydroepiandrosterone] and free testosterone should be checked for abnormalities. If any perianal lesions exist in the presence of gastrointestinal symptoms, biopsy should be considered. Screening for depression, anxiety, suicidal ideation, and substance use disorders is important as individuals with HS may be at increased risk.1
Management of Hidradenitis suppurativa
Hidradenitis suppurativa has a significant impact on quality of life and can be very difficult to treat. Treatment options include both medical and surgical intervention in addition to addressing the pain and psychological impact that accompanies the disease. Although there is no cure, many effective evidence-based treatments are available to control disease progression and improve symptoms. The goal is not only to manage flares but also to help reduce their recurrence. Treatment regimens should be tailored to each patient and are based on disease severity and lifestyle factors. Attention to the effect of HS on the patient’s quality of life is important, with referrals as needed to counseling and other supports.
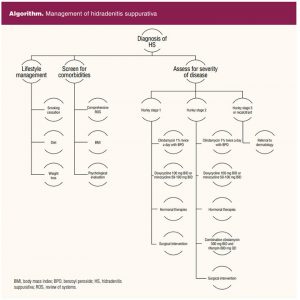
 Treatment options are based on Hurley staging and include antibiotics, topical cleansers, hormonal therapies, biologics, adjunct treatments, or surgical interventions. Antibiotics are a common mainstay in the treatment of HS and are likely effective due to their anti-inflammatory properties and not their antibacterial action.6 Clindamycin 1% (solution or gel) is the only topical antibiotic shown to be effective. It can be used for Hurley stage 1 and 2 and as an adjunct to systemic therapies.5 For moderate/severe disease or acute flaring, oral antibiotics should be utilized. Tetracycline derivatives have been shown to be helpful, but ideally these are used in short courses (< 3 months) for individuals with several lesions or frequent exacerbations.5,7,8 Combination clindamycin 300 mg twice a day and rifampin 600 mg daily is an effective second-line therapy.5 To help reduce the potential for bacterial resistance, both oral and topical antibiotics should be used in combination with benzoyl peroxide. Biologic therapy can be considered for patients with Hurley stage 2/3 who are unresponsive to systemic antibiotics. Adalimumab is a fully human monoclonal antibody targeting TNF-alpha and is the first and only systemic therapy approved by the US Food and Drug Administration (FDA) for moderate-to-severe HS. Results of randomized controlled trials have demonstrated higher efficacies, reduction in abscess and inflammatory nodule count, and improvement of pain and quality of life when compared to placebo after 12 weeks of treatment.9 As a rescue therapy for acute flares, intralesional corticosteroids or a short course of oral prednisone can help accelerate the resolution of painful inflammatory lesions.10 Long-term systemic steroid use is not advised. Limited evidence suggests that combination oral contraceptive pills or spironolactone 100 to 150 mg daily may be helpful for women, especially if menstrual flaring exists. There is anecdotal data suggesting that progestogen-only contraceptives may worsen HS symptoms.5 Individuals who are pregnant or lactating can be treated with topical therapies or surgical procedures if needed.5 Patients who have not improved after 3 months of treatment, have experienced an increase in frequency of flares, or who have severe disease should be referred to a dermatology specialist.
Treatment options are based on Hurley staging and include antibiotics, topical cleansers, hormonal therapies, biologics, adjunct treatments, or surgical interventions. Antibiotics are a common mainstay in the treatment of HS and are likely effective due to their anti-inflammatory properties and not their antibacterial action.6 Clindamycin 1% (solution or gel) is the only topical antibiotic shown to be effective. It can be used for Hurley stage 1 and 2 and as an adjunct to systemic therapies.5 For moderate/severe disease or acute flaring, oral antibiotics should be utilized. Tetracycline derivatives have been shown to be helpful, but ideally these are used in short courses (< 3 months) for individuals with several lesions or frequent exacerbations.5,7,8 Combination clindamycin 300 mg twice a day and rifampin 600 mg daily is an effective second-line therapy.5 To help reduce the potential for bacterial resistance, both oral and topical antibiotics should be used in combination with benzoyl peroxide. Biologic therapy can be considered for patients with Hurley stage 2/3 who are unresponsive to systemic antibiotics. Adalimumab is a fully human monoclonal antibody targeting TNF-alpha and is the first and only systemic therapy approved by the US Food and Drug Administration (FDA) for moderate-to-severe HS. Results of randomized controlled trials have demonstrated higher efficacies, reduction in abscess and inflammatory nodule count, and improvement of pain and quality of life when compared to placebo after 12 weeks of treatment.9 As a rescue therapy for acute flares, intralesional corticosteroids or a short course of oral prednisone can help accelerate the resolution of painful inflammatory lesions.10 Long-term systemic steroid use is not advised. Limited evidence suggests that combination oral contraceptive pills or spironolactone 100 to 150 mg daily may be helpful for women, especially if menstrual flaring exists. There is anecdotal data suggesting that progestogen-only contraceptives may worsen HS symptoms.5 Individuals who are pregnant or lactating can be treated with topical therapies or surgical procedures if needed.5 Patients who have not improved after 3 months of treatment, have experienced an increase in frequency of flares, or who have severe disease should be referred to a dermatology specialist.
Pain is often a significant burden to sufferers of HS. It is important to acknowledge that treatment of the underlying inflammatory state is essential to controlling the pain and reduce the number and severity of flares. Pharmacologic pain management options include topical analgesics like lidocaine 5% ointment or diclofenac 1% gel and oral nonsteroidal anti-inflammatory drugs (NSAIDs).2,4 Contraindications to the use of NSAIDs include liver or renal impairment, gastrointestinal bleeding, inflammatory bowel disease, peptic ulcers, or heart failure.4 Tramadol can be used as a nonopioid alternative for refractory pain.2 There is no clinical evidence to support use of opioids in HS patients, so for severe or recalcitrant pain control a pain management specialist should be utilized.
Surgical intervention can be a consideration for unresponsive lesions or extensive scarring in addition to medical management; however, the technique remains a challenge as there is no clarity in the literature regarding which surgical intervention is the most optimal. Contemplation for surgical intervention should be individualized, with consideration to the affected site, extent of disease, and the patient’s comorbidities.11 Options include simple excision, wide local excision, carbon dioxide (CO2) ablative laser treatments, or deroofing (electrosurgically removing only the top layers of an abscess, cyst, or sinus tract). Incision and drainage can be beneficial for relieving acute pain, but it is discouraged as a long-term practice because it can induce further inflammation and reoccurrence rates remain high.11 See the Algorithm for an overview of the management of HS.
Lifestyle modifications
It is important to reinforce that HS is not a result of infection, poor hygiene, is not sexually transmitted, or contagious. Even though the contributory mechanisms remain poorly understood, patients may benefit from select lifestyle modifications to help ease the development or exacerbation of HS. Diet, smoking, and mechanical stress have all been reported as possible contributors to the development or exacerbation of HS. Shaving, waxing, depilatory creams, and deodorants can be possible triggers, but are not known to be causative factors. Shaving or waxing in between flares is generally considered safe but should be avoided during acute flares to prevent additional trauma and inflammation. There are no clear data on use of washcloths, loofahs, or bath brushes in individuals with HS, but in general patients should also be advised to avoid harsh or aggressive scrubbing. Antiseptic cleansers and anti-inflammatory washes like benzoyl peroxide are the most beneficial cleansers.
Data support a strong relationship to smoking, but a causal relationship has not been clearly identified.2,7,10,12 All HS patients should be advised to stop smoking. In addition, patients who are obese should be encouraged to reduce their BMI as improvements in disease severity have been reported after weight loss.13 Patients are advised to avoid friction from tight clothing because that can worsen inflammation. There are no official dietary recommendations, but some individuals have reported seeing improvement with diets low in glycemic index, gluten, or dairy products.12 Further studies are needed, but an evaluation of nutritional status may be helpful and patients may be advised to keep a food diary to help identify individual food triggers. Any patient exhibiting signs of depression, anxiety, substance-related disorders, or suicidal ideation should be referred to a mental health provider.
Future research
Although there has been a recent surge in HS research, it continues to be one of the most enigmatic inflammatory skin conditions. There are current research efforts on the role of additional biologic target molecules like interleukins, Janus kinases, hormones, and complement that may aid in future treatment options. Research efforts are needed on the differences between HS presentations among different ethnic groups, races, and genders and the role diet plays in HS pathogenesis.
Conclusion
Hidradenitis suppurativa is a chronic and debilitating disease that can have great impact on an individual’s quality of life. It is important that patients receive prompt diagnosis and appropriate management to avoid the long-term physical and psychological effects that often accompany it. This article is meant to serve as a guide for disease awareness, diagnosis, and treatment options based on the most up-to-date evidence available.
References
- Garg A, Neuren E, Cha D, et al. Evaluating patients’ unmet needs in hidradenitis suppurativa: results from the Global Survey Of Impact and Healthcare Needs (VOICE) Project. J Am Acad Dermatol. 2020;82(2):366-376.
- Hendricks AJ, Hsiao JL, Lowes MA, Shi VY. A comparison of international management guidelines for hidradenitis suppurativa. Dermatology. 2021;237:81-96.
- Dufour DN, Emtestam L, Jemec GB. Hidradenitis suppurativa: a common and burdensome, yet under-recognized, inflammatory skin disease. Postgrad Med J. 2014;90:216-221.
- Patel K, Liu L, Ahn B, et al. Hidradenitis suppurativa for the nondermatology clinician. Proc (Bayl Univ Med Cent). 2020;33(4):586-591.
- Alikhan A, Sayed C, Alavi A, et al. North American clinical management guidelines for hidradenitis suppurativa: A publication from the United States and Canadian Hidradenitis Suppurativa Foundations: Part I: Diagnosis, evaluation, and the use of complementary and procedural management. J Am Acad Dermatol. 2019;81(1):76-90.
- Matusiak Ł, Bieniek A, Szepietowski JC. Bacteriology of hidradenitis suppurativa—which antibiotics are the treatment of choice? Acta Derm Venereol. 2014;94(6):699-702.
- Zouboulis CC, Bechara FG, Dickinson-Blok JL, et al. Hidradenitis suppurativa/acne inversa: a practical framework for treatment optimization -systematic review and recommendations from the HS ALLIANCE working group. J Eur Acad Dermatol Venereol. 2019;33(1):19-31.
- Wieczorek M, Walecka I. Hidradenitis suppurativa -known and unknown disease. Reumatologia. 2018;56(6):337-339.
- Gupta AK, Studholme C. Adalimumab (Humira) for the treatment of hidradenitis suppurativa. Skin Therapy Lett. 2016;21(4):1-4.
- Tchero H, Herlin C, Bekara F, et al. Hidradenitis suppurativa: a systematic review and meta-analysis of therapeutic interventions. Indian J Dermatol Venereol Leprol. 2019;85(3):248-257.
- Scuderi N, Monfrecola A, Dessy LA, et al. Medical and surgical treatment of hidradenitis suppurativa: a review. Skin Appendage Disord. 2017;3(2):95-110.
- Narla S, Lyons AB, Hamzavi IH. The most recent advances in understanding and managing hidradenitis suppurativa. F1000Res. 2020;9:F1000 Faculty Rev-1049.
- Kromann CB, Ibler KS, Kristiansen VB, Jemec GBE. The influence of body weight on the prevalence and severity of hidradenitis suppurativa. Acta Derm Venereol. 2014;94(5):553-557.
Key words: hidradenitis suppurativa, acne inversa, dermatology, diagnosis, treatment, management