
We live in a world where visible skin conditions can profoundly affect self-esteem and self-confidence, and some individuals are under the impression that anything less than perfection is simply unacceptable. Although there are individuals fortunate enough to have clear complexions, many suffer from blemishes, bumps, lumps, and discoloration on their faces often mistaken for acne vulgaris. Acne is extremely common and diagnosis is usually easy, but there are a variety of skin diseases that can be associated with erythematous papules, pustules, or comedones on the face often mimicking acne vulgaris. Not all lesions that are present on the face are due to acne. While acne vulgaris is one of the most common dermatologic conditions worldwide, there are several separate differentials with similar manifestations but entirely different epidemiology, treatments, and prognosis. Due to the wide variety of presentations, misdiagnosis can occur. It is important to know and understand the sometimes subtle differences in these diseases as it will alter therapeutic regimens and impact overall outcomes of treatment. This article is aimed at helping differentiate some of the conditions commonly mistaken for acne vulgaris to improve diagnostic accuracy and treatment outcomes for patients presenting with comedonal, papular, or pustular lesions on the face or body.
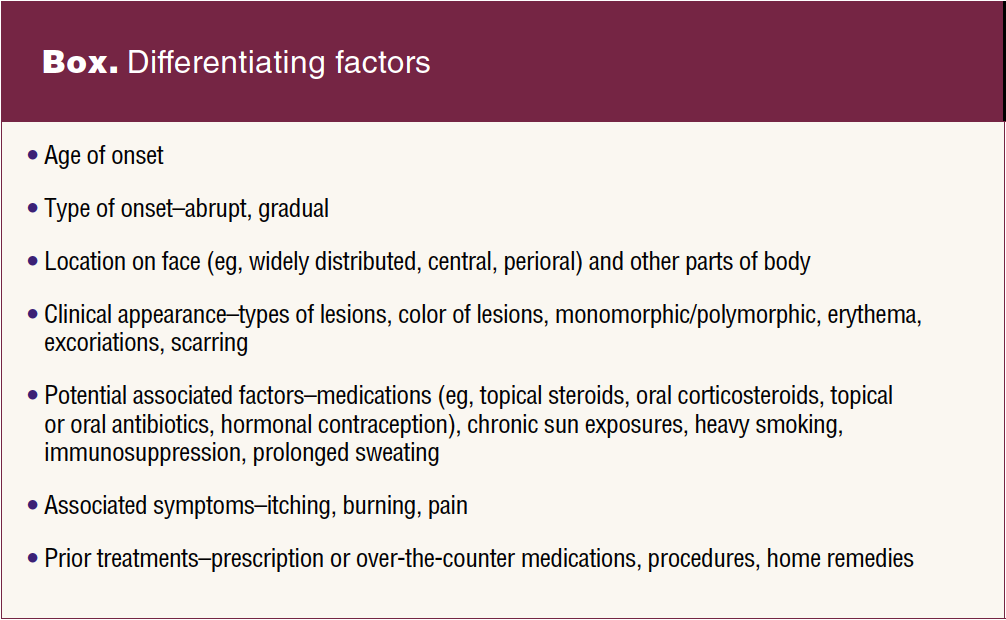
Acne vulgaris is a multifactorial, immune-mediated, androgen-triggered inflammatory disease of the pilosebaceous unit (the hair follicle and associated sebaceous gland).1 The pathogenesis of this disease is a complex relationship between four key pathogenic factors that include follicular hyperkeratinization, the proliferation of Cutibacterium acnes (formally Propionibacterium acnes), excess sebum production, and inflammation. This interplay results in the presence of open or closed comedones (blackheads and whiteheads), inflammatory papules, pustules, nodules, cysts, and scarring. Diagnosis is made based on clinical examination, and treatment is individualized based on severity. Retinoids, antimicrobial washes, antimicrobial topical preparations, oral antibiotics, and hormonal therapies are all used in a variety of combinations to target the underlying pathogenic causes. However, the key to clearing skin can be more challenging for some. Knowing and understanding the potential variants and differential diagnoses associated with acne vulgaris can help guide practitioners in clinical decision making that facilitates patients receiving treatments that are the most effective. The Box provides a summary of differentiating factors to consider.
Acne variants
Acne excoriee
Acne excoriee is an excoriation disorder that is described as an uncontrollable desire to pick or scratch at the skin. It is typically limited to the face. It is a distinct entity within the group of obsessive-compulsive and related disorders. The underlying acne is typically mild, but affected individuals compulsively pick and squeeze at superficial lesions often resulting in significant scarring. The primary clinical findings of this disorder are excoriations rather than acneiform eruptions. It is rare to see primary acne lesions, but post- inflammatory hyperpigmentation and scarring are often present. Treatment for this condition includes traditional acne treatments to aid in reducing the number of comedones or inflammatory lesions and referral to a mental health specialist is often helpful.
Acne conglobata
Acne conglobata is a rare but severely disfiguring form of acne. The clinical presentation includes painful, interconnected comedones, cysts, inflammatory nodules, draining abscesses, and keloid-like scarring.2 It can occur gradually or abruptly as a sudden worsening of pustular acne most often on the face, trunk, arms, and lower extremities.2 If left untreated, acne conglobata can lead to permanent disfigurement. The severity of this disease differentiates it from traditional acne vulgaris with evidence of deep cysts, sinus tracts, nodules, or double comedones (multiple blackheads within one single follicle). The presence of large nodulocystic lesions, abscesses, or significant and disfiguring scarring should prompt immediate referral to dermatology. Topical treatments are largely unhelpful, and patients need aggressive treatment with systemic medications like prednisone, isotretinoin, and oral antibiotics to reduce the deformity.2 Surgical interventions may be necessary to treat scarring.
Acne fulminans
Acne fulminans is a rare but devastating skin disease that presents as a sudden onset of painful, ulcerating, or hemorrhagic acne-like eruption primarily affecting young men. It has been known to be associated with systemic symptoms of fever, malaise, polyarthritis, and anorexia. Like acne conglobata, if left untreated, it can result in severe scarring and disfigurement, so dermatology referral should be prompt. Treatment is difficult and can include corticosteroids, isotretinoin, and biologic therapy.
Acne differential diagnosis
Periorificial dermatitis
Periorificial dermatitis is a benign eruption that occurs most commonly in young female adults, consisting of small inflammatory papules and pustules or pink, scaly patches most commonly around the mouth.3 It can also affect periocular or paranasal skin. Etiology is largely unknown, but it has been associated with the use of topical steroids, fluorinated toothpaste, cosmetic products and sunscreens, inhaled steroids, and application of dental fillings. Given the female predominance, there may be a link to hormonal factors.3 Lesions can be itchy, tender, or sometimes described as having a burning sensation. The vermillion border of the lip and the immediate circumoral area are typically spared. When differentiating this disease from acne vulgaris, it is important to look for the absence of comedones, breakouts only occurring around the mouth, and inquire about the presence of itching or burning. Acne typically occurs in a much more generalized distribution. If topical steroids are being applied to the face, they should be discontinued. Treatments for perioral dermatitis include topical metronidazole, topical clindamycin, topical calcineurin inhibitors, and oral tetracycline antibiotics.3 Disease typically improves in 6 to 12 weeks with proper treatment, but this can be a chronic relapsing condition that requires long-term management.
Rosacea
Although it is sometimes referred to as acne rosacea, rosacea and acne vulgaris are two separate diagnoses. Rosacea is a chronic and inflammatory skin disease characterized by flushing, nontransient erythema, papules, pustules, telangiectasia, and sometimes phymatous (thickened, irregular nodularity found commonly on the nose, chin, forehead, or ears) changes.4 The etiology is not well understood, but immune dysfunction, Demodex (a common, benign mite living within human hair follicles) infestation, and exposure to ultraviolet radiation are believed to be contributing factors.4 Differentiating acne vulgaris from rosacea can be a challenge, but the first clue is paying attention to the presence or absence of comedones (blackheads and whiteheads). The absence of comedones favors a diagnosis of rosacea. Both diseases can include inflammatory lesions on the face, but the second clue in deciphering between the two is the location of lesions. In rosacea, lesions are primarily localized to the medial cheeks, nose, forehead, and chin where acne is more widespread across the entire face. In addition, there is a vascular component in patients with rosacea causing transient flushing exacerbated with triggers like heat, hot beverages, spicy foods, or stress that is not present in acne vulgaris. Treatments for rosacea include topical metronidazole, azelaic acid, ivermectin, minocycline, oral antibiotics, oral beta blockers for persistent erythema, laser therapy, and strict trigger avoidance.5
Medication-induced acne
Acne-like eruptions can occur as an adverse effect due to several systemic medications. It is most commonly seen with the use of oral corticosteroids, but it also can be induced by androgenic anabolic steroids, lithium, high doses of vitamin B12, halogen compounds (ie, iodine, bromine, fluorine, and chlorine), antiepileptic drugs, epidermal growth factor receptor inhibitors (EGFR), and oral contraceptives containing progestins with androgenic properties.5,6 It should be noted that long-acting reversible hormonal contraception methods like levonorgestrel intrauterine devices and subdermal progestin implants lack sufficient data, but have been shown to contribute to acne-like eruptions in some people.7 Drug- induced acne is clinically hallmarked by an abrupt eruption of monomorphic (similar in appearance) 1 to 3 mm follicular papules and pustules beyond the traditional seborrheic zone (ie, hairline, eyebrows, nasolabial folds, and chin). Cystic lesions and nodules are rare. The main differentiating factors between medication- induced acne and acne vulgaris are the lack of polymorphic presentation seen in acne vulgaris, a rapid onset, and is usually pruritic.6 It is important to have a detailed history of recent or current medications, the record of medication onset, dosage regimen, and medication therapy duration to help identify a clinical relationship between the drug and the onset of the acne-like eruption.6 The time between medication exposure and the acne-like eruption will differ depending on the offending agent but can be seen as rapidly as 2 to 5 weeks. Discontinuation of the medication will lead to remission of symptoms in all cases.5,6 If discontinuation of the medication is not possible, then traditional acne medications like retinoids or topical antibiotics can be initiated.
Sebaceous hyperplasia
The number of sebaceous glands (oil glands) remains unchanged throughout life, but the gland itself can atrophy over time.7 The most common reason for this atrophy is in response to aging or excessive sun exposure, so sebaceous hyperplasia develops mainly in individuals age 50 years or older. It is mostly seen in the forehead and cheeks and is clinically manifested as single or multiple pale yellow or flesh-colored papules ranging from 1 to 5 mm in size often with central umbilication.7 It does not have inflammatory lesions or comedones associated with acne vulgaris. It also is associated with those who are immunosuppressed or have a history of Muir-Torre syndrome (a rare genetic disorder causing tumors in sebaceous glands and internal organs). Sebaceous hyperplasia is a benign disorder not requiring treatment, although cosmetic therapies include cryosurgery, photodynamic therapy, laser treatment, electrodesiccation, excision, or isotretinoin.8 If there is a solitary lesion located on the sun-exposed skin that is pink, painful, bleeding, or is occurring in a high-risk population, then a dermatology referral is recommended to rule out basal cell carcinoma as they can be clinically similar.
Favre-Racouchot syndrome
Clinically, this syndrome is characterized by a diffuse yellowish hue with the presence of large, open, black comedones symmetrically distributed on the temporal and periorbital areas, and deep wrinkles and furrows over a background of actinically damaged and atrophic skin.9,10 It most often occurs in middle-age to elderly individuals.9,10 Long-term sun exposure, radiation, and heavy smoking are known predisposing factors to this condition.10 Unlike acne vulgaris, inflammation is conspicuously absent, and location is localized to the temporal or periorbital areas. Treatment includes meticulous sun protective measures, cessation of smoking, topical retinoids, surgical extraction, or laser resurfacing.
Malassezia (Pityrosporum) folliculitis
Malassezia (Pityrosporum) folliculitis is a common disorder characterized by an intensely pruritic, monomorphic eruption of perifollicular pustules and inflammatory papules 1 to 2 mm in size on the face, chest, arms, or upper back.11 Malassezia folliculitis results from an overgrowth of yeast present in the normal cutaneous flora.11 Eruptions of this condition are associated with any alteration in normal flora like immunosuppression or antibiotic use. It is seen more often in warmer months, during long periods of sweating, or in those who wear occlusive clothing.11 The condition clinically resembles, is commonly misdiagnosed as, and can coexist with acne vulgaris.12 While it can occur anywhere on the face, it mostly affects the chin and lateral face as opposed to the central facial lesions of acne vulgaris. In addition, acne vulgaris does not typically itch. It is important to differentiate folliculitis from acne vulgaris because antibiotic treatments can further exacerbate the disease.11 If the two disease states overlap, it is ideal to use other anti-acne therapies over antibiotics to avoid this. Treatment includes both oral and topical antifungal medications.
Lupus miliaris disseminatus faciei
Lupus miliaris disseminatus faciei (LMDF) is a rare idiopathic granulomatous disease that primarily affects the central face of young adults. Although it typically has a spontaneously resolving course lasting months to years, it is cosmetically debilitating given the location and potential for scarring.13 Clinically, it appears as an abrupt eruption of bilaterally symmetric red, yellow, brown, or flesh-colored papules on the central areas of the face including the forehead, eyelids, nose, cheeks, and perioral areas.13 Acne can have a similar presentation, but this disease lacks comedones and its onset is usually beyond the teenage years. Acne most often does not have a symmetric distribution or affect the eyelids. Other granulomatous disorders like rosacea can have a similar presentation, but patients with LMDF do not have the accompanying vascular abnormalities like flushing and telangiectasias or the exacerbation associated with triggers like sun, alcohol, stress, or spicy foods. Etiology is largely unknown and treatment options have a paucity of data but include combinations of oral tetracyclines, isotretinoin, prednisone, or oral dapsone. This condition can lead to permanent scarring, so accurate diagnosis and quick onset of treatment is aimed at reducing the cosmetic impact as much as possible.
Emotional considerations
Acneiform eruptions are sometimes believed to be trivial, especially when compared to other diseases, but lesions on the face and body affect more than just the skin. Society often emphasizes the importance of appearance and the psychological, social, and emotional ramifications that can coincide with acne-like dermatoses should not be taken lightly. Patients have reported an association with negative self-image, embarrassment, difficulty in sports and school/work, and reduction in social activities.14 There is a known association between acne and an increase in depression and anxiety.15
When the primary care provider should consider a referral
Primary care providers can give extremely high-quality care to patients with a variety of dermatologic needs, but there are times when referral is required to a dermatology specialist. If patients experience an abrupt onset of lesions, if they have exceptionally severe disease, evidence of scarring, or have acne that is recalcitrant to traditional acne therapies, prompt referral to a dermatology specialist is needed.
Conclusion
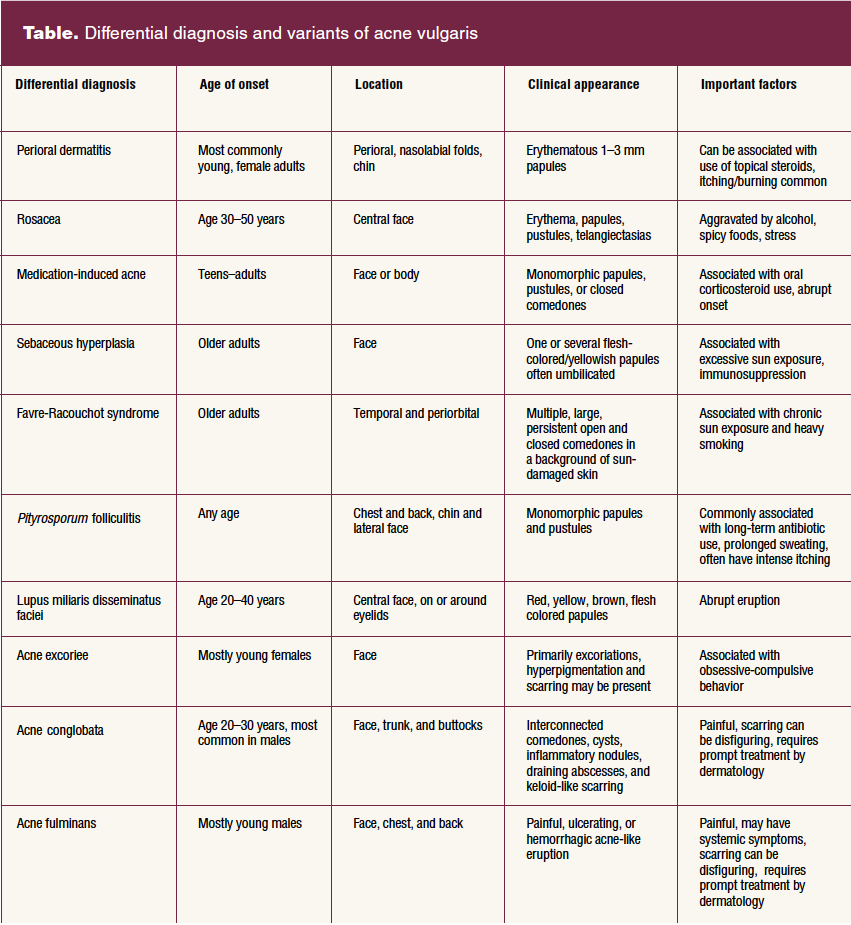
Several differential diagnoses are associated with lesions on the face that can easily be mistaken for acne vulgaris. Considering the potential variants of acne and the differential diagnoses most commonly mistaken for it can support clinical decision making that facilitates patients receiving appropriate and effective treatment. This is especially relevant when patients present with facial lesions not typical of acne vulgaris or who are not responding to treatment. This article serves as a guide for some of the possible alternatives to acne vulgaris. The Table summarizes common characteristics for the differential diagnoses that have been described.
Nicole L. Bort is a dermatology nurse practitioner at University Hospitals of Cleveland Medical Centers, and Clinic Instructor at Case Western Reserve University School of Medicine in Cleveland, Ohio. The author has no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(2):26-31. doi: 10.51256/WHC042326
References
1 Bort NL, Bobonich MA. Updates on acne in adult females. Womens Healthcare. 2021;9(1):8-14,48.
2 Hafsi W, Arnold DL, Kassardjian M. Acne conglobata. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2022 Jan-. Updated November 22, 2022.
3 Tolaymat L, Hall MR. Perioral dermatitis. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2022 Jan-. Updated September 5, 2022.
4 Zhang H, Tang K, Wang Y, et al. Rosacea treatment: review and update. Dermatol Ther. 2021;11(1):13-24.
5 Pontello R Jr, Kondo RN. Drug- induced acne and rose pearl: similarities. An Bras Dermatol. 2013;88(6):1039-1040.
6 Kazandjieva J, Tsankov N. Drug- induced acne. Clin Dermatol. 2017;35(2):156-162.
7 Bosanac SS, Trivedi M, Clark AK, et al. Progestins and acne vulgaris: a review. Dermatol Online J. 2018;24(5):13030/qt6wm945xf.
8 Hou X, Wei Z, Zouboulis CC, Ju Q. Aging in the sebaceous gland. Front Cell Dev Biol. 2022;10:909694.
9 Al-Natour SH. Acne mimickers: another cause for unresponsive acne. J Saudi Soc Dermatology Dermatologic Surg. 2012;16(2):35-40. http://dx.doi.org/10.1016/j.jssdds.2012.04.002.
10 Sonthalia S, Arora R, Chhabra N, Khopkar U. Favre-Racouchot syndrome. Indian Dermatol Online J. 2014;5(suppl 2):S128-S129. doi:10.4103/2229-5178.146192
11 Rubenstein RM, Malerich SA. Malassezia (pityrosporum) folliculitis. J Clin Aesthet Dermatol. 2014;7(3):37-41.
12 Malgotra V, Singh H. Malassezia (Pityrosporum) folliculitis masquerading as recalcitrant acne. Cureus. 2021;13(2):e13534.
13 Toda-Brito H, Aranha JMP, Tavares ES. Lupus miliaris disseminatus faciei. An Bras Dermatol. 2017;92(6):851-853.
14 Hazarika N, Archana M. The psychosocial impact of acne vulgaris. Indian J Dermatol. 2016;61(5):515-520.
15 Nguyen CM, Beroukhim K, Danesh MJ, et al. The psychosocial impact of acne, vitiligo, and psoriasis: a review. Clin Cosmet Investig Dermatol. 2016;9:383-392.
Key words: acne vulgaris, differential diagnosis, rosacea, perioral dermatitis, medication-induced acne, Favre-Racouchot syndrome, folliculitis, acne excoriee, acne conglobata, acne fulminans