
Faculty: Nicole L. Bort, MSN, AGNP-C, DCNP, is a dermatology nurse practitioner and Director of the Nurse Practitioner Post-Graduate Training Program and Margaret A. Bobonich, DNP, FNP-C, DCNP, FAANP, is a dermatology nurse practitioner at University Hospitals Cleveland Medical Centers, Case Western Reserve University, in Cleveland, Ohio.
Intended audience: This continuing education (CE) activity has been designed to meet the educational needs of nurse practitioners and other healthcare providers who provide primary care for women.
CE approval period: Now through February 28, 2023
Estimated time to complete this activity: 1 hour
CE approval hours: 1.0 contact hour of CE credit including 0.50 contact hours of pharmacology content
Goal statement: Nurse practitioners and other healthcare providers who provide primary care for women will increase their knowledge about the pathogenesis, assessment, and medical management of acne in adult females.
Needs assessment: Acne is one of the most common inflammatory dermatologic conditions seen by primary healthcare providers and is postulated to be more common in women than men. Nurse practitioners and other healthcare providers who provide primary care for women need the knowledge to differentiate acne from other dermatologic conditions, assess severity, and make appropriate management decisions that may include treatment of mild-to-moderate cases and referral to a dermatology specialist when indicated.
Educational objectives: At the conclusion of this educational activity, participants should be able to:
- Discuss the four key pathogenic factors and potential triggers that contribute to adult acne.
- Describe the clinical presentation of mild, moderate, and severe classifications of acne.
- Describe indications, mechanism of action, efficacy, adverse effects, and contraindications for pharmacologic options in treating acne.
Accreditation statement: This activity has been evaluated and approved by the Continuing Education Approval Program of the National Association of Nurse Practitioners in Women’s Health (NPWH) and has been approved for 1 contact hour of CE credit, including 0.50 hours of pharmacology credit.
Faculty disclosures: NPWH policy requires all faculty to disclose any affiliation or relationship with a commercial interest that may cause potential, real, or apparent conflict of interest with the content of a CE program. NPWH does not imply that affiliation or relationship will affect the content of the CE program. Disclosures provides participants with information that may be important to their evaluation of an activity.
Nicole L. Bort, MSN, AGNP-C, DCNP, has no actual or potential conflicts of interest in relation to this article. Margaret A. Bobonich, DNP, FNP-C, DCNP, FAANP, has no actual or potential conflicts of interest in relation to the contents of this article.
Disclosure of unlabeled/unapproved use: NPWH policy requires authors to disclose to participants when they are presenting information about unlabeled use of a commercial product or device, or an investigational use of a drug or device not yet approved for any use.
Disclaimer: Participating faculty members determine the editorial content of the CE activity; this content does not necessarily represent the views of NPWH. This content has undergone a blinded peer review process for validation of clinical content. Although every effort has been made to ensure that the information is accurate, clinicians are responsible for evaluating this information in relation to generally accepted standards in their own communities and integrating the information in this activity with that of established recommendations of other authorities, national guidelines, FDA-approved package inserts, and individual patient characteristics.
Successful completion of the activity: Successful completion of this activity, J-21-01, requires participants to do the following:
- “Sign In” in at the top right-hand corner of this page if you have an NPWH account. You must be signed in to receive credit for this course. If you do not remember your username or password, please follow the “Forgot Password” link and instructions on the sign-in page. If you do not have an account, please click on “Create an Account.”*
- Read the learning objectives, disclosures, and disclaimers on the next page and then click on the “Continue” button.
- Study the material in the learning activity during the approval period (now through February 28, 2023).
- Complete the post-test and evaluation. You must earn a score of 70% or higher on the post-test to receive CE credit.
- Print out the CE certificate after you have successfully passed the post-test and completed the evaluation.
*If you are an NPWH member, were once a member, or have taken CE activities with NPWH in the past, you have a username and password in our system. Please do not create a new account. Creation of multiple accounts could result in loss of CE credits as well as other NPWH services. If you do not remember your username or password, either click on the “Forgot Username” or “Forgot Password” link or call the NPWH office at (202) 543-9693, ext. 1.
Commercial support: This activity did not receive any commercial support.
Before reading the article, click hereA to take the pretest.
Acne vulgaris is one of the most commonly treated dermatologic diseases in adult females, but treatment selection and patient education should be tailored specifically to this population. Acne in women has a known association with both physical and psychological factors. There are often genetic, hormonal, and skin care routines that play a role in the etiopathogenesis, and maintenance is often required for many years. Taking into consideration appropriate assessment and diagnosis of severity for acne and having knowledge about available treatment modalities will facilitate successful management.
Key words: acne vulgaris, adult female acne, dermatology, acne cosmetica, hormonal acne, skin care
“True beauty comes from within” is an axiom that many of us heard during our youth. This statement of wisdom underscores the belief that people should not be judged by their physical attributes or imperfections but rather by the inner beauty from their soul. This can be a challenging concept to embrace for females suffering from acne, a skin condition that is visible for all the world to see.
Nurse practitioners (NPs) who provide care for women across the lifespan often diagnose and treat acne. Some NPs have gained an even greater understanding about the physical and psychosocial impact of acne through their own personal experience, family, and friends. This article addresses assessment and diagnostic considerations and appropriate management options to aid NPs in providing high-quality evidence-based care for adult females with acne.
Epidemiology
Acne is one of the most common inflammatory dermatoses worldwide and is treated by both primary care clinicians and dermatology specialists.1 Acne vulgaris is a multifactorial, immune-mediated, androgen-triggered inflammatory disease of the pilosebaceous unit (the hair follicle and associated sebaceous gland). Onset is frequently associated with puberty, but recent data suggest that upward of 41% of adult females struggle with some form of acne and 78% of them have admitted to worsening lesions during their premenstrual period.1 It is postulated that females are more affected by acne than men in all age groups and it can even persist after age 50.2
Pathogenesis
The pathogenesis of acne involves a complex interplay of four key pathogenic factors including:
- Follicular hyperkeratinization
- Proliferation of Cutibacterium acnes (formerly Propionibacterium acnes)
- Excess sebum production
- Inflammation and irritation
There are likely genetic and hormonal factors that contribute to the increasing number of females who manifest acne in adulthood, but the true cause has not been elucidated. Several triggers or aggravating factors have been hypothesized and include exposure to ultraviolet radiation, stress, obesity, diet, smoking, sleep disorders, medications, excessive skin washing, possible resistance to C. acnes, and diseases that cause androgen excess.3 Women may also have acne cosmetica resulting from comedogenic products that contain ingredients like petrolatum, oils, lanolin, and chemicals (alcohol, oleic acid, or butyl stearate). Regardless of the etiology, acne in adult females can impact quality of life and have significant negative psychological impact.
Hormonal acne
Hormone-related acne in adult females most commonly manifests as a predominance of inflammatory lesions involving the lower third of the face (mandibular line, perioral region, and side of the neck). There should be a high degree of suspicion in cases with a sudden onset of acne, associated symptoms of hirsutism, menstrual irregularities, or any other signs of hyperandrogenism. Although not common, acne can be a cutaneous manifestation of underlying systemic conditions like polycystic ovary syndrome (PCOS), adrenal tumors, ovarian tumors, or congenital adrenal hyperplasia. Recommended laboratory studies include dehydroepiandrosterone sulfate, luteinizing hormone, follicle-stimulating hormone, free and total testosterone, and androstenedione.4 These tests should be performed during the follicular phase of the menstrual cycle and between the morning hours of 8 and 10 am. Hormonal therapies should be stopped 1 month prior to the tests for the most accurate results.
Clinical presentation and diagnosis
The presentation of acne is variable and ranges from mild comedones to inflammatory papules, pustules, nodules, cysts, and scarring. It occurs most often on the face, chest, and back because these areas have the largest concentration of pilosebaceous units. Acne is classified as mild, moderate, or severe depending on the type and number of lesions, location, and presence or absence of scarring (Figure). The degree of disease severity provides the basis for an evidence-based approach by the clinician. In general, the diagnosis of acne requires the presence of open or closed comedones (blackheads and whiteheads) with or without inflammation.
Figure. Algorithmic approach for acne treatment
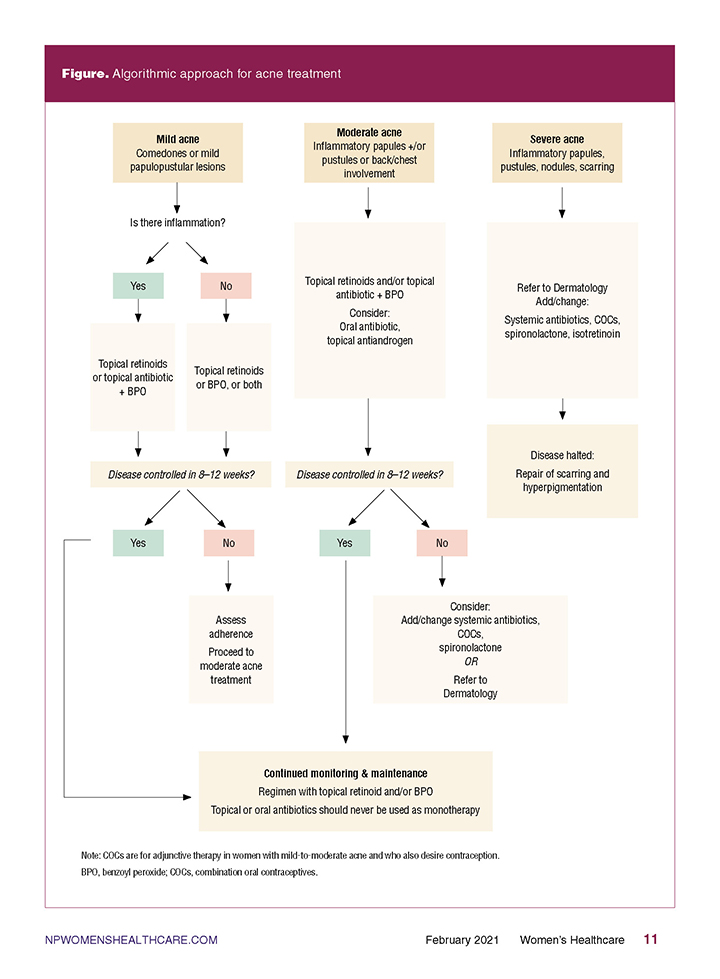
Clinicians should assess patients for the presence of inflammatory lesions that can be characterized as papules, pustules, nodules, or cysts. Evidence of inflammatory lesions on the face or any type of acne lesions involving the trunk classifies acne as moderate severity. The presence of cysts, nodules, or scarring escalates the condition to a severe disease state and should prompt immediate referral to a dermatology specialist to prevent permanent sequelae.
The diagnosis of acne is a clinical one. The presence of comedones is required for the diagnosis of acne vulgaris, whereas the absence of comedones is helpful in differentiating it from other dermatoses. It is important to ensure that acne-like variants such as rosacea and perioral dermatitis have been excluded prior to initiating treatment. Additional laboratory testing should be performed if the diagnosis is unclear or there is suspicion for an underlying systemic or endocrine abnormality.
Skin of color
The characteristics of acne are not homogenous and are influenced by racial and ethnic backgrounds. Adult females with darker skin types are at higher risk for post-inflammatory hyperpigmentation, which can result from inflammation or trauma (picking or squeezing lesions). One study described the emotional and social impact of post-inflammatory hyperpigmentation including a negative effect on quality of life in addition to symptoms of anxiety or depression.5 Findings showed that 57.9% of White/Caucasian women reported lesion clearance as the most important measure of successful acne treatment compared to only 31.7% of non-White/Caucasian women [Black/African American, Hispanic/Latina, Asian, and other]. In contrast, clearing the post-inflammatory hyperpigmentation was of the greatest importance for non-White/Caucasian women (41.6%) compared to 8.4% of White/Caucasian women. This emphasizes not only the differences in the burden of acne on skin of color but also should guide treatment choices. If possible, acne treatments that also address secondary pigmentary changes are ideal for these patients.
Management
Treatment plans should be individualized considering severity, morphology, distribution, and patient history. A discussion regarding lactation and the possibility of being or becoming pregnant during treatment is also important for women of childbearing potential as some medications may be contraindicated. To date, there are no topical medications that treat all the pathogenic causes of acne. Systemic treatment with isotretinoin is the only pharmacotherapy that targets all four pathways of acne pathogenesis (Table 1). Thus, the goal should be a targeted approach that may require a combination of treatment modalities. Shared decision making, re-evaluation, and modifications to therapy are paramount for achieving optimal patient outcomes. Although there are many remedies and treatments based on anecdotes that have been utilized, it is essential for the clinician to use evidence-based treatment guidelines for management of adult females with acne.6
Table 1. Targeted therapeutics for acne
| Medication | Normalize keratinization |
Decrease C. acnes |
Decrease inflammation |
Decrease sebum |
| Topical benzoyl peroxide | X | X | X | |
| Topical retinoids | X | X | ||
| Topical antimicrobials | X | X | ||
| Topical antiandrogen | X | X | ||
| Oral antibiotics | X | X | ||
| Spironolactone | X | |||
| Combination oral contraceptives | X | |||
| Isotretinoin | X | X | X | X |
Mild acne
For mild acne (comedones only), treatment should include mild cleansers, topical retinoids, and antimicrobial agents with several combination products available (Table 2). Potential side effects include mild irritation or erythema, but they are overall well tolerated. There should be close monitoring for improved response or progression to more severe forms of the disease.
Table 2. Topical and oral acne treatments
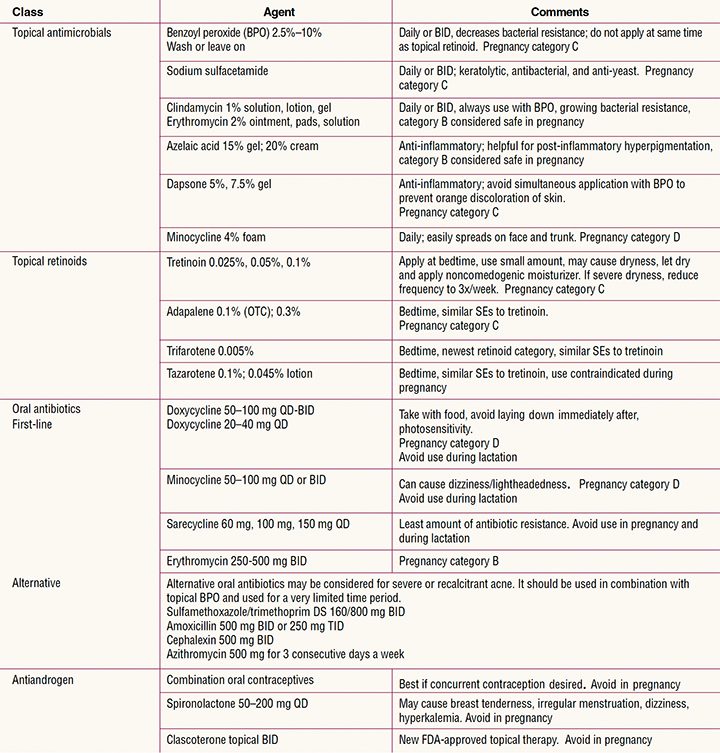
Note: Several combined therapy options are available.
BID, twice daily; DS, double strength; OTC, over the counter; QD, four times daily; SEs; side effects; TID, three times daily.
Topical therapies
Topical retinoids, antimicrobial agents, and antibiotics are first-line therapy for mild acne and the basis for acne of any severity.
- Benzoyl peroxide (BPO) is an antimicrobial agent that both kills C. acne and is mildly comedolytic. It has been shown to not only enhance antibiotic therapy but it may also reduce bacterial resistance.
- Retinoids are ideal to treat comedonal acne because they are both comedolytic and anti-inflammatory. The most common side effects include erythema, irritation, and dryness. Side effects can be minimized with gentle skin care and moisturizers. There is a risk of photosensitivity with retinoids, so daily sunscreen should be encouraged. Topical retinoids should not be applied at the same time as BPO, which can degrade the retinoid molecule and render it ineffective. Some stable combinations are available to avoid this problem.
- Topical antibiotics have been postulated to be effective through anti-inflammatory mechanisms in addition to their antibacterial effects. Topical erythromycin and clindamycin have been the most widely used as they can reduce the concentration of C. acnes, but because there is a growing bacterial resistance, monotherapy is not recommended. Recently, the addition of topical minocycline products may be a worthy alternative as they potentially provide a lower rate of bacterial resistance promotion, but more studies are needed. Concurrent use of BPO increases efficacy to topical antibiotics in addition to reducing the risk of bacterial resistance and should be used whenever possible.
- Alternative topicals should also be taken into consideration as topical dapsone and azelaic acid can be helpful in patients who have sensitive skin or in those with dyspigmentation from inflammatory lesions.
- Topical antiandrogens are the newest novel drug class introduced for the treatment of acne. Clascoterone is the first drug in this class to be approved. It directly competes with dihydrotestosterone (DHT) for binding to the androgen receptor on the sebaceous gland and reduces downstream sebum production and inflammation. Clascoterone has promising data as a complement in the acne armamentarium for its antiandrogen effects and limited systemic activity.7
Moderate acne
For moderate acne (comedones plus inflammatory lesions) combining systemic antibiotics with topical products offers a synergistic effect and maximizes therapy (Table 2).
Table 3. Acne basic skin concepts
- Keep facial washing simple with a twice-daily regimen using a gentle cleanser
- Always wash off makeup before going to bed by using an oil-free makeup remover
- Choose makeup, moisturizers, and sunscreens that are labeled as noncomedogenic or “oil-free”
- Never squeeze or pick acne lesions
- Avoid sharing makeup, brushes, and beauty blenders
- Avoid using “testers” at beauty counters
- Look for cosmetic products that have expiration displayed on the products
- Regularly clean brushes, beauty blenders, and tools to avoid self-contamination
- Avoid harsh exfoliants, scrubbing, and mechanical devices
- Avoid overuse of OTC acne treatments containing salicylic acid, astringents, masks
- Use sun protection
OTC, over the counter.
- Oral antibiotics are generally indicated when there is widespread involvement of face, chest, and back. Tetracycline and its derivatives are typically first choice. Long-term use is not recommended due to increasing resistant strains of C. acnes, and monotherapy is not recommended. Treatment duration should not exceed 3 to 4 months. The most reported side effects include photosensitivity, gastrointestinal upset, vaginal candidiasis, and hypersensitivity. More severe side effects like severe allergic reactions, Steven’s Johnson syndrome, lupus-like reactions, and pseudotumor cerebri have been reported, so patients should be closely monitored.
- Combination oral contraceptives (COCs) suppress testosterone production and increase production of sex hormone binding globulin (SHBG), reducing serum concentrations of free testosterone. This makes them an especially good adjunct therapeutic option for treatment of mild-to-moderate acne for women who also desire contraception and who do not have contraindications to their use. For women with PCOS, the use of COCs can reduce the occurrence of both acne and excess facial hair. COCs used solely for acne treatment should be evaluated for their risk compared to other systemic therapies. Typically, it takes at least 3 months of use before a significant effect can be demonstrated. Several COC brands have received formal US Food and Drug Administration (FDA) approval for treatment of mild-to-moderate acne, but all formulations are effective.
- Spironolactone is oftentimes used due to its local antiandrogenic properties, directly competing with DHT for cutaneous receptors. The result is an inhibition for DHT and testosterone binding. In addition, it offers some inhibition of 5α-reductase activity and increased quantity of SHBG causing a reduction in circulating free testosterone.8 Spironolactone should be avoided in patients taking potassium-sparing diuretics, angiotensin-converting enzyme inhibitors, potassium supplements, lithium, or who are pregnant or attempting pregnancy. Total and free testosterone levels do not need to be regularly monitored for those with no underlying endocrinology abnormalities. Typical dosage ranges from 50 to 200 mg daily.
Severe acne
Severe acne should prompt immediate referral to a dermatology specialist for treatment considerations to reduce the potential for long-term scarring. Severe disease often requires treatment that includes isotretinoin. To date, isotretinoin remains the most clinically effective anti-acne therapy and can produce substantial improvement and long-term remission. Due to severe teratogenic properties and potential for adverse side effects, however, there are several necessary rules for prescribing, monitoring, and the mandatory participation in the FDA Risk Evaluation and Mitigation Strategy program iPLEDGE. Isotretinoin therapy must be prescribed by a registered iPLEDGE practitioner. Additional therapeutics may be used based on severity and individual case. Experienced dermatology clinicians may use intralesional steroids, short-course oral corticosteroids, chemical peels, extractions, photodynamic therapy, and lasers as complements to acne regimens.
Patient education
Cosmetics
Adult female acne can be caused or exacerbated by heavy use of cosmetics. Although C. acnes is the most common pathogen in acne, individual cosmetic practices by females may also impact the skin health. In a study investigating the extent of microbial contamination of cosmetic products, researchers identified the specific type and load of bacteria in lipstick, lip gloss, eyeliners, mascaras, and beauty blenders.9 The role and potential risk of all of the pathogens for acne have not been determined but are concerning. Approximately 79% to 90% of the products were contaminated with bacteria including Staphylococcus aureus, Escherichia coli, and Citrobacter freundii. In addition, beauty blenders had a high prevalence of Enterobacteriaceae and fungi (56%–96%). Patient education on the use and cleaning of cosmetics and applicators should be foremost in avoiding use of contaminated products. About 93% of the beauty blenders had not been cleaned, while 64% were reported dropped on the floor and continued use.
Skin care
All acne care should begin with washing twice daily using a gentle cleanser along with other measures to prevent/control flares (Table 3). Patients benefit from education that guides them through avoiding the gauntlet of skin care products with unfounded advertisements promising a cure for acne.
Lifestyle modifications
It is postulated that foods with high glycemic index, dairy products, high stress levels, and lack of sleep may all play a role in the severity of acne in some females.10 Further studies are required to fully understand the impact of these factors, but talking to patients about how some of these can contribute may prompt lifestyle changes that may make a positive difference in both their acne and overall health.
Conclusion
Adult females may present with the common characteristics of acne vulgaris, but there are several unique etiopathogenic factors that make management of adult female acne more challenging. Cost, resources, potential for side effects, and patient preferences are important variables and the key to patient adherence. This article serves as a guide on recommendations for best evidence-based clinical practices and therapeutic decisions to help manage both the physical and psychological symptoms that often accompany it.
References
- Rocha MA, Bagatin E. Adult-onset acne: prevalence, impact, and management challenges. Clin Cosmet Investig Dermatol. 2018;11:59-69.
- Bagatin E, Freitas THP, Rivitti-Machado MC, et al. Adult female acne: a guide to clinical practice. An Bras Dermatol, 2019;94(1):62-75.
- Dréno B, Thiboutot D, Layton AM, et al; Global Alliance to Improve Outcomes in Acne. Large-scale international study enhances understanding of an emerging acne population: adult females. J Eur Acad Dermatol Venereol. 2015;29(6):1096-1106.
- Barros B, Thiboutot D. Hormonal therapies for acne. Clin Dermatol. 2017;35(2):168-172.
- Callender VD, Alexis AF, Daniels SR, et al. Racial differences in clinical characteristics, perceptions and behaviors, and psychosocial impact of adult female acne. J Clin Aesthet Dermatol. 2014;7(7):19-31.
- Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016;74(5):945-973.e33.
- Rosette C, Agan FJ, Mazzetti A, et al. Cortexolone 17a-propionate (clascoterone) is a novel androgen receptor antagonist that inhibits production of lipids and inflammatory cytokines from sebocytes in vitro. J Drugs Dermatol. 2019;18(5):412-418.
- Kim GK, Del Rosso JQ. Oral spironolactone in post-teenage female patients with acne vulgaris: practical considerations for the clinician based on current data and clinical experience. J Clin Aesthet Dermatol. 2012:5(3):37-50.
- Bashir A, Lambert P. Microbiological study of used cosmetic products: highlighting possible impact on consumer health. J Appl Microbiol. 2020;128(2):598-605.
- Bansal P, Sardana K, Vats G, et al. A prospective study examining trigger factors and hormonal abnormalities in adult female acne. Indian Dermatol Online J. 2020;11(4):544-550.