
Nurse practitioners have a pivotal role in caring for adolescent females, especially in regard to the unique needs of this patient group, and can help educate them about what is needed to live a healthy life. This article discusses guidelines from the Women’s Preventive Services Initiative on preventive adolescent well-woman care, including recommendations for routine health maintenance, lifestyle risk reduction, and specific guidelines for reproductive and sexual health.
Key words: Women’s Preventive Services Initiative, preventive adolescent well-woman care
Healthcare for the female adolescent marks the transition from pediatric patient to adult care and is a time of robust change.1 Nurse practitioners (NPs) caring for this population have an opportunity to provide education and preventive care to promote the development of lifelong healthy habits. A 2016 Lancet commission on adolescent health and well-being stresses that adolescents are biologically, emotionally, and developmentally prepared to engage beyond their families, and clinicians can encourage adolescents to meaningfully participate in their health.2
This article’s focus is on preventive adolescent well-woman care based on recommendations from the Women’s Preventive Services Initiative (WPSI). The WPSI is led by an expert advisory panel representing the American Academy of Family Physicians, American College of Obstetricians and Gynecologists, American College of Physicians, and the National Association of Nurse Practitioners in Women’s Health. The panel developed a well-woman chart and a clinical summary table with preventive services recommended by the WPSI, US Preventive Services Task Force (USPSTF), and Bright Futures based on age, health status, and risk factors. Recommendations for immunizations are provided by the Advisory Committee on Immunization Practices.2,3 The WPSI recommendations serve as the basis for insurance coverage at no cost-sharing to patients.3 These recommendations are not intended as a statement of standard of care. NPs should use clinical judgment in applying the recommendations to individual patient care.
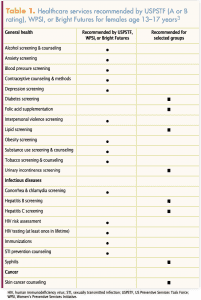 The WPSI chart has two relevant age groups for adolescent preventive services recommendations, ages 13 to 17 years and ages 18 to 21 years (Table 1, Table 2). In this discussion, we have chosen to be flexible in adolescent age range regarding various recommendations. Preventive services recommendations for pregnant and postpartum adolescents are not included in this article.
The WPSI chart has two relevant age groups for adolescent preventive services recommendations, ages 13 to 17 years and ages 18 to 21 years (Table 1, Table 2). In this discussion, we have chosen to be flexible in adolescent age range regarding various recommendations. Preventive services recommendations for pregnant and postpartum adolescents are not included in this article.
Preventive services recommendations
Immunizations
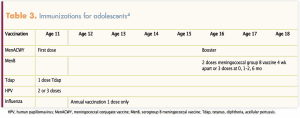
Immunizations needed for adolescents include meningococcal vaccine; tetanus, diphtheria, acellular pertussis (Tdap); human papillomavirus (HPV); and annual influenza vaccine (Table 3).4 Immunization records should be evaluated because adolescents may need other catch-up vaccines. Education on the importance of immunizations, infection risk and consequences, and counseling to overcome barriers such as fear of needles should be key focuses for adolescent patients.1
Blood pressure screening
Hypertension (HTN) is a common adult condition that when not adequately managed creates long-term consequences and future risk of heart disease and stroke. In the adolescent population, the prevalence of HTN is estimated at 5% to 20% and considered underdiagnosed because it is usually asymptomatic.5,6 Identification of elevated blood pressure (BP) or HTN and attention to contributing factors are important. Data indicate that elevated BP in childhood correlates with the onset of HTN in young adulthood.7 The USPSTF, however, notes it is unclear if the treatment of HTN in adolescents prevents future cardiovascular disease.7
Bright Futures recommends that children should have BP routinely measured beginning at age 3 years, and the WPSI recommends that adolescents ages 13 to 21 years have annual BP screening.3,7,8 Adolescents age 13 years and older with a blood pressure persistently greater than 120/80 mm Hg require further evaluation. Diagnosis of elevated blood pressure and HTN are based on normative percentiles that factor in age, sex, and height.6,9
Depression screening
Almost a quarter of adolescents experience at least one major depressive episode by age 19. Depression includes feelings of sadness and loss of interest in activities and can cause impairment in daily life.10,11 Adolescents may not recognize that these are signs of depression and are unlikely to seek professional help on their own. A negative stigma is often attached to mental health diagnosis and treatment, further contributing to underdiagnosis of adolescent depression.12 Of those diagnosed, only 20% seek treatment, and fewer than 40% of those receiving treatment comply with the regimen.13 When untreated, depression in adolescence can disrupt developmental processes, which can have negative consequences on adult psychosocial outcomes.14
The WPSI guidelines recommend annual screening for major depressive disorder (MDD) for adolescents ages 13 to 21 years.3 The USPSTF recommends that clinicians screen all adolescents for MDD but does not specify frequency.15 Several MDD screening tools developed for primary care settings have been used with adolescents. Two of the most widely studied are the Patient Health Questionnaire for Adolescents and the Beck Depression Inventory.15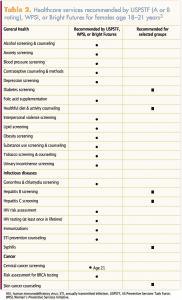
Anxiety screening
Anxiety disorders include several related conditions all characterized by excessive, uncontrollable worry. The prevalence rate of anxiety among adolescents age 13 to 18 years is 32%, with an estimated 8.3% having severe impairment. Anxiety rates are higher for girls than boys (38% vs 26%).16 Anxiety disorders can cause significant impairment in daily activities including school performance and can adversely impact well-being and social relationships. In children and adolescents, anxiety disorders are frequently associated with depression, eating disorders, and attention-deficit/hyperactivity disorder.17 Screening has the potential to identify previously unrecognized anxiety so that further assessment can take place and individualized treatment initiated to prevent progression and impairment.
The WPSI guidelines recommend screening females age 13 years and older for anxiety.3 The USPSTF has a screening recommendation update in progress for depression, anxiety, and suicide risk in children and adolescents.A
Lipid screening
There is no recommendation to routinely screen for dyslipidemia in adolescents. The USPSTF concludes that current evidence is insufficient to assess the balance of benefits and harms of screening for lipid disorders in children and adolescents age 20 years or younger.18 Bright Futures recommends a one-time screening for dyslipidemia between the ages of 17 and 21 years, especially if there is a family history of dyslipidemia or if the patient smokes cigarettes or e-cigarettes.8,19
Diabetes screening
The annual incidence rate of type 2 diabetes in adolescents has increased by 4.8% from 2003 to 2012.20 Current guidelines from the American Diabetes Association recommend diabetes screening for adolescents who are overweight or obese and have at least two additional risk factors. Risk factors include family history of diabetes, maternal history of gestational diabetes, high-risk race/ethnicity (Black, Hispanic, Asian, Native American, Pacific Islander), or current signs of insulin resistance.21 Although the WPSI does not recommend routine screening for diabetes in adolescents, it does recommend screening for individuals age 13 years or older who have had gestational diabetes in pregnancy but have not been previously diagnosed with diabetes when not pregnant.3
Hepatitis B, hepatitis C, and tuberculosis screening
The recommendations for screening for hepatitis B, hepatitis C, and latent tuberculosis in adolescents are based on individual risk factors for these infections. Routine screening for this age group is not recommended.3
Cancer screening, risk assessment, and counseling
Cervical cancer screening is recommended starting at age 21 for average-risk women regardless of sexual history or human papillomavirus (HPV) vaccination status. Cervical cytology alone should be used every 3 years in the 21- to 29-year-old age group. Co-testing with cytology and HPV testing is not recommended in women younger than age 30 years.3,22
In the general US population, BRCA1/2 mutations occur in 1 in 300 to 500 women and account for 5% to 10% of breast cancer cases.23 The USPSTF recommends that clinicians assess women with a brief familial risk assessment tool. Women with a positive result on the risk assessment tool should receive genetic counseling and, if indicated and desired after counseling, genetic testing.23 The WPSI recommends that this risk assessment start between ages 18 and 21.3
Fair-skinned children, adolescents, and young adults should utilize protective behaviors to minimize exposure to ultraviolet radiation. These protective behaviors include limiting sun exposure and use of sunscreen. Radiation exposure during childhood and adolescence increases the risk of skin cancer later in life.3,8,24
Urinary incontinence screening
Approximately 50% of women experience urinary incontinence that can adversely affect their quality of life.3 Although rates of urinary incontinence are higher among older women, adolescents and younger adults who have risk factors such as obesity or previous vaginal delivery are also at risk. The WPSI recommends screening women ages 18 to 21 years for urinary incontinence, as well as adolescents ages 13 years and older who have had a vaginal delivery. Clinicians can refer for further diagnostic evaluation and treatment if indicated.3
Healthy diet, activity, and obesity
Obesity is a known risk factor for diabetes and cardiovascular disease (CVD), and evidence shows that obesity may also be a risk factor for chronic inflammation and development of asthma.25,26 Data from the 2016 NHANES indicate the prevalence of obesity (body mass index [BMI] 30 or higher) among adolescent females (ages 12–19 years) is 21%, a significant increase from the 1999 rate of 15%.27 In addition to risks for chronic physical health conditions, adolescents who are obese may experience low self-esteem or psychological issues related to teasing and bullying from peers based on their weight.28
All adolescents should be screened for obesity using age/gender-specific BMI percentiles charts.3,8,28 The USPSTF and the WPSI recommend that individuals 18 years of age or older who are overweight or obese and who have additional CVD risk factors be offered referral to comprehensive programs that include dietary, activity, and behavioral counseling components to support healthy weight loss and improve long-term health.3,28
Tobacco, alcohol, and substance use screening and counseling
The WPSI recommends that individuals age 13 and older should be screened annually for the use of tobacco/nicotine products (including vaping), alcohol, and illicit drugs and appropriately counseled.3,29 Identification of risk and protective factors for the development of drug and alcohol use should be assessed.8
The American Academy of Pediatrics has provided a policy statement on substance use screening, brief intervention, and referral to treatment for pediatricians.30 This policy includes a flow chart for questioning adolescents, providing treatment or referral, and describes adolescent substance use in these categories: abstinence, experimentation, limited use, problematic use, abuse, and addiction. For adolescents who report experimentation or limited substance use, NPs should promote patient strengths, encourage cessation, and provide clear educational counseling. Adolescents who report problematic use should have close follow-up and possible referral. NPs who identify an adolescent with substance abuse or addiction should encourage parental involvement and refer the adolescent for comprehensive assessment and treatment. Breaking patient–provider confidentiality may be necessary when serious health risks are identified. The NP should be aware of state laws and HIPAA [Health Insurance Portability and Accountability Act] requirements regarding disclosure of information.
Interpersonal violence
All adolescent females should be screened annually for interpersonal violence that includes physical and sexual violence, stalking and psychological aggression, reproductive coercion, and neglect.3 Any sexual activity for which consent is not freely given constitutes sexual violence.31 The Youth Risk Behavior Survey from 2017 reported 11% of adolescent females have experienced sexual dating violence.32 This same survey reported 9% of adolescent females have experienced physical violence within a teen dating relationship.32 Recognizing risk factors and incorporating screening questions about interpersonal violence of all types will help lead to earlier detection and promote safety.33
Reproductive and sexual health
Educating adolescents about reproductive and sexual health is an important part of comprehensive well-woman care. The NP should make no assumptions about sexual orientation, gender identity, or sexual activity, ask open questions about sexual health, and use inclusive and sensitive history-taking language.34 Three components guide practice: recognizing sexual rights, sexuality education and counseling, and confidential high-quality services.35 Incorporating these components supports young women in feeling empowered regarding bodily autonomy and sexual rights.
Although it may be ideal to involve parents or guardians in the care of adolescents, the adolescent female may not seek reproductive and sexual health services if she knows her parents will be informed. NPs should be aware of state laws that govern the age at which reproductive and sexual healthcare can be provided without parental involvement, with variations in age restrictions existing about contraceptive services, sexually transmitted infection (STI) screening and treatment, and referral to abortion services.B
Information on prevention of STIs is an essential part of adolescent reproductive and sexual health. Risks for STIs are higher in the female adolescent population due to factors including cervical ectopy, increased likelihood of multiple sex partners, and lower use of condoms.36,37 In 2017, there were over 1 million cases of chlamydia infection among adolescents and young adults (ages 15–24 years) in the United States, and rates for gonorrhea and syphilis are consistently higher among adolescents than older women.37 Annual gonorrhea and chlamydia screening is recommended for all sexually active women age 24 and younger.3,38 Risk factors for human immunodeficiency virus (HIV) should be assessed annually starting at age 13, along with testing for HIV at least once in the lifetime of each woman.3 Screening for syphilis should be considered for adolescents with risk factors.3 Safer sex practices that include condom and dental dam use and limiting number of sexual partners should be strongly encouraged to reduce risk of STIs.
NPs should ask the adolescent about reproductive goals and if she is considering having children at some point. Sexually active females of any age who could become pregnant should be taking a multivitamin with folic acid to decrease risk for neural tube defects.3 Sexually active females who are at risk for unplanned pregnancy should be counseled on contraceptive choices. Contraceptive counseling that gives attention to personal preference, risk–benefits and future family planning goals promotes patient-centered decision making.3 Hormonal contraception, especially long-acting reversible contraceptives (LARCs), is highly effective and well suited for adolescents.39,40 Whichever method is chosen, the NP should encourage the adolescent to use condoms for STI prevention. Evidence suggests adolescents who use LARCs are less likely to use condoms.40
Conclusion
NPs should strive for providing high-quality care that incorporates understanding of unique female adolescent needs. The WPSI guidelines encourage evidence-based care and provide recommendations for routine health maintenance, lifestyle risk reduction, and specific guidelines for reproductive and sexual health. The transition from pediatric care to well-woman care should be seamless and include comprehensive services unique to this population. Additional information on WPSI recommendations and interactive well-woman charts for use on computers and phones is available at womenspreventivehealth.org/wellwomanchart/. C
Sandi Tenfelde is Associate Professor at Loyola University Marcella Niehoff School of Nursing in Maywood, Illinois. She is a member of the board of directors of NPWH. Lindsey Garfield is Assistant Professor at Loyola University Marcella Niehoff School of Nursing. The authors state that they do not have any financial interest in or other relationship with any commercial product named in this article.
References
Bernstein HH, Bocchini JA, Committee on Infectious Diseases. The need to optimize adolescent immunization. Pediatrics. 2017;139(3):e20164186.
Patton GC, Sawyer SM, Santelli JS, et al. Our future: a Lancet commission on adolescent health and wellbeing. Lancet. 2016;387(10036):2423-2478.
Phipps MG, Son S, Zahn C, et al; Women’s Preventive Services Initiative. Women’s Preventive Services Initiative’s well-woman chart: a summary of preventive health recommendations for women. Obstet Gynecol. 2019;134(3):465-469.
CDC Advisory Committee on Immunization Practices. Recommended child and adolescent immunization schedule for ages 18 years and younger, United States 2020. https://www.cdc.gov/vaccines/schedules/downloads/child/0-18yrs-combined-schedule-bw.pdf.
Anyaegbu EI, Dharnidharka VR. Hypertension in the teenager. Pediatr Clin North Am. 2014;61(1):131-151.
Weaver DJ Jr. Hypertension in children and adolescents. Pediatr Rev. 2017;38(8):369-382.
Moyer VA. Screening for primary hypertension in children and adolescents: USPSTF recommendation statement. Pediatrics. 2013;132(5):907-914.
Hagan JF, Shaw JS, Duncan PM. Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents, 4th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2017.
Flynn JT, Kaelber DC, Baker-Smith CM, et al; Subcommittee on Screening and Management of High Blood Pressure in Children. Clinical Practice Guideline for Screening and Management of High Blood Pressure in Children and Adolescents. Pediatrics. 2017;140(3):e20171904.
Alsaad AJ, Al Nasser Y. Depression in Children. Treasure Island, FL: StatPearls Publishing; 2019.
Bernaras E, Jaureguizar J, Garaigordobil M. Child and adolescent depression: a review of theories, evaluation instruments, prevention programs, and treatments. Front Psychol. 2019;10:543.
Bravender T. Mental disorders and learning disabilities in children and adolescents: depression in adolescents. FP Essent. 2018;475:30-41.
Singh S, Zaki RA, Farid NDN. A systematic review of depression literacy: knowledge, help-seeking and stigmatising attitudes among adolescents. J Adolesc. 2019;74:154-172.
Clayborne ZM, Varin M, Colman I. Systematic review and meta-analysis: adolescent depression and long-term psychosocial outcomes. J Am Acad Child Adolesc Psychiatry. 2019;58(1):72-79.
Siu AL; US Preventive Services Task Force. Screening for depression in children and adolescents: US Preventive Services Task Force Recommendation Statement. Pediatrics. 2016;137(3):e20154467.
National Institute of Mental Health. Any anxiety disorder. 2017. https://www.nimh.nih.gov/health/statistics/and-anxiety-disorder.shtml.
Nelson HD, Cantor A, Pappas M, Weeks C. Screening for anxiety in adolescent and adult women: systematic review for the Women’s Preventive Services Initiative. 2020:1-63. https://www.womenspreventivehealth.org/wp-content/uploads/Screening-for-Anxiety-Report.pdf.
US Preventive Services Task Force; Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Screening for lipid disorders in children and adolescents: US Preventive Services Task Force recommendation statement. JAMA. 2016;316(6):625-633.
Wiegman A. Lipid screening, action, and follow-up in children and adolescents. Curr Cardiol Rep. 2018;20(9):80.
Mayer-Davis EJ, Lawrence JM, Dabelea D, et al. Incidence trends of type 1 and type 2 diabetes among youths, 2002-2012. N Engl J Med. 2017;376(15):1419-1429.
Xu H, Verre MC. Type 2 diabetes mellitus in children. Am Fam Physician. 2018;98(9):590-594.
US Preventive Services Task Force; Curry SJ, Krist AH, Owens DK, et al. Screening for cervical cancer: US Preventive Services Task Force recommendation statement. JAMA. 2018;320(7):674-686.
Moyer VA. Risk assessment, genetic counseling, and genetic testing for BRCA-related cancer in women: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2014:160(4):271-281.
US Preventive Services Task Force; Bibbins-Domingo K, Grossman DC, Curry SJ, et al. Screening for skin cancer: US Preventive Services Task Force recommendation statement. JAMA. 2016;316(4):429-435.
Ho HCH, Maddaloni E, Buzzetti R. Risk factors and predictive biomarkers of early cardiovascular disease in obese youth. Diabetes Metab Res Rev. 2019;35(4):e3134.
Sanyaolu A, Okorie C, Qi X, et al. Childhood and adolescent obesity in the United States: a public health concern. Glob Pediatr Health. 2019;6:2333794X19891305
Fryar CD, Carroll MD, Ogden CL. Prevalence of overweight, obesity, and severe obesity among children and adolescents aged 2–19 years: United States, 1963–1965 through 2015–2016. Division of Health and Nutrition Foundation. National Center for Health Statistics. Health E-Stats. September 2018.
US Preventive Services Task Force; Grossman DC, Bibbins-Domingo K, Curry SJ, et al. Screening for obesity in children and adolescents: US Preventive Services Task Force recommendation statement. JAMA. 2017;317(23):2417-2426.
Alinsky RH, Percy K, Adger H Jr, et al. Substance use screening, brief intervention, and referral to treatment in pediatric practice: a quality improvement project in the Maryland Adolescent and Young Adult Health Collaborative Improvement and Innovation Network. Clin Pediatr. 2020 Jan 29. Epub ahead of print.
Committee on Substance Abuse; Levy SJL, Kokotailo PK. Substance use screening, brief intervention, and referral to treatment for pediatricians. Pediatrics. 2011;128(5):e1330–e1340.
Northridge JL. Sexual violence in adolescents. Pediatr Ann. 2019;48(2):e58-e63.
Kann L, McManus T, Harris WA, et al. Youth risk behavior surveillance – United States, 2017. MMWR Surveill Summ. 2018;67(8):1-114.
Littlefield AD, Hunt DA, Keefe JM. Teen dating violence: not child’s play. Women’s Healthcare. 2019;7(4):22-30.
Leonardi M, Frecker H, Scheim AI, Kives S. Reproductive health considerations in sexual and/or gender minority adolescents. J Pediatr Adolesc Gynecol. 2019;32(1):15-20.
Apter D. Contraception options: aspects unique to adolescent and young adult. Best Pract Res Clin Obstet Gynaecol. 2018;48:115-127.
Cuffe KM, Newton-Levinson A, Gift TL, et al. Sexually transmitted infection testing among adolescents and young adults in the United States. J Adolesc Health. 2016;58(5):512-519.
Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2018. Atlanta, GA: US Department of Health and Human Services; 2019.
LeFevre ML; US Preventive Services Task Force. Screening for chlamydia and gonorrhea: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;161(12):902-910.
Sherin M, Waters J. Long-acting reversible contraceptives for adolescent females: a review of current best practices. Curr Opin Pediatr. 2019;31(5):675-682.
Steiner RJ, Liddon N, Swartzendruber AL, et al. Long-acting reversible contraception and condom use among female US high school students: implications for sexually transmitted infection prevention. JAMA Pediatr. 2016;170(5):428-434.
Web resources
B. guttmacher.org/state-policy/explore/overview-minors-consent-law