
As the science has grown around the female athlete triad, researchers have gained a greater understanding of the consequences that low-energy availability has on both men and women’s bodies. In 2014, experts defined relative energy deficiency in sport (RED-S), a gender-inclusive model comprehensive of all body systems impacted by energy deficiency. RED-S is prevalent, affecting up to 22% to 58% of women in various sports and physical activities, but it is not well understood among healthcare providers. Women’s healthcare providers play an important role in providing female athletes with education on fueling their bodies with the energy necessary to promote health and wellness while supporting performance goals. This article provides nurse practitioners and other healthcare professionals with a clinical overview of RED-S and how its health implications may impact issues relevant to women’s healthcare.
In 1992, the American College of Sports Medicine held a special conference to address a growing concern about the health of female athletes. The conference focused on a triad of medical disorders, collectively termed the female athlete triad: disordered eating, amenorrhea, and osteoporosis.1 As scientific understanding of this phenomenon advanced, the triad was redefined as a clinical entity involving the “relationship between three interrelated components: energy availability, menstrual function, and bone health.”2 The pathophysiology of the disordered state was further described and understood along a continuum through which healthy athletes with optimal energy availability, regular menses, and healthy bones digress along the spectrum to an unhealthy athlete with low energy availability (LEA), amenorrhea, and decreased bone mineral density leading to osteoporosis.3 Low energy availability present in the triad could be explained with or without disordered eating.2 Throughout the 2000s, research in this field continued to elucidate energy deficiency as the primary factor underpinning the consequences of the triad. Energy deficiency occurs when dietary energy intake is inadequate compared to the energy expenditure needed to support normal body functions from growth and development and activities of daily living to exercise and sport.3
In 2014, the International Olympic Committee introduced and defined relative energy deficiency in sport (RED-S), a broader and more comprehensive term for what was previously known as the female athlete triad.3 In addition to menstrual function and bone health issues related to energy deficiency, RED-S syndrome includes impaired physiologic function impacting protein synthesis, metabolic rate, immunity, and cardiovascular health.3 RED-S is a clinical phenomenon that extends to encompass the physiologic and psychological complexities related to energy deficiency experienced by both males and females. Not only gender-inclusive, RED-S applies to a more general population of individuals to include those involved in recreational sport and physical activities such as dancing, as the effects of low-energy availability are not exclusive to athletes.3 This article provides nurse practitioners and other healthcare professionals with a clinical overview of RED-S and how the health implications of RED-S may impact issues relevant to women’s healthcare.
Health implications of RED-S in women
The amount of energy that most healthy, active women need for optimal physiologic function is 45 calories or more per day per kg of fat-free mass (kcal/kg FFM day).3 Less than 30 kcal/kg FFM day is considered a threshold for LEA when unfavorable physiologic changes occur in women.4 Whereas LEA can result from energy restriction associated with disordered eating and intentional weight loss without disordered eating, it can also occur with low energy-density diets and excessive exercise or training.4 Whole grains, fruits, and vegetables are examples of low-energy density foods. Due to their high water and fiber content, these foods cause individuals to feel full after eating, which can result in having LEA if other energy-dense foods are not consumed. These low energy-density diets are effective for overweight individuals to lose weight, but they may not provide the energy necessary for an active person to perform optimally. When energy demands outweigh the body’s available energy, physiologic changes take place to accommodate the discrepancy. Essential physiologic functions such as thermoregulation and cellular maintenance are prioritized while other less important functions necessary to survive such as bone turnover and menstruation are suppressed.5,6
Energy deficiency or LEA manifests clinically across several body systems. Endocrine system adaptions to LEA in women include disruptions in the hypothalamic-pituitary-ovarian axis, altered thyroid function, decreases in insulin and insulin-like growth factor, changes in appetite-regulating hormones, and increased cortisol.7 Female athletes with oligo or amenorrhea when compared to eumenorrheic peers have demonstrated altered bone turnover markers and less bone strength and increased risk for fractures.2,8,9 Low body mass index (BMI) and LEA are related to decreased bone density and fracture risk.8,9 In women, LEA has been associated with a suppressed metabolic rate.4 Metabolic dysfunction can contribute to hematologic changes in female athletes resulting in low ferritin and iron deficiency anemia.4
Similar to individuals with anorexia nervosa, dysfunction in insulin-like growth factor 1 and a disorderly response to growth hormone can contribute to suppressed linear growth in female athletes.4 Endocrine dysfunction leading to a hypoestrogenic state affects the cardiovascular system negatively. Research involving amenorrheic female athletes has shown lipid dysfunction and endothelial damage that may lead to early atherosclerosis.10 In studies of young female athletes, LEA has been associated with negative gastrointestinal symptoms such as stool leakage resulting from altered sphincter function and constipation related to delayed gastric emptying.11,12 The immune system also may be impacted by LEA with amenorrheic female athletes reporting greater frequency of upper respiratory symptoms and having decreased levels of immunoglobulin A when compared to eumenorrheic peers.13
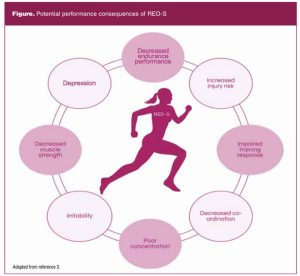
Finally, psychological function is impacted by LEA. The relationship between psychological problems and LEA is bidirectional. Psychological issues can precede LEA such as an unhealthy drive for thinness or a desired level of performance, and can also result from LEA. For example, when compared to healthy controls, adolescent females with functional hypothalamic amenorrhea have higher incidences of depression, psychosomatic disorders, and difficulties managing stress.14 As a result, all of these disruptions and adaptations to LEA collectively cause a decline in athletic performance.4,15 Potential performance consequences of RED-S are depicted in the Figure.
Recognizing risks and preventing RED-S
Preventing RED-S begins with educating healthcare professionals, parents, coaches, and athletes about RED-S. Despite the fact that the female athlete triad was defined nearly three decades ago, several surveys have indicated a knowledge deficit among physicians, physical therapists, and athletic trainers, with less than half of these healthcare professionals correctly identifying components of the female athlete triad.16–19 RED-S, being relatively new to the scene as having been defined in 2014, is less understood among healthcare professionals. In a 2020 survey of healthcare professionals in attendance at a sports medicine conference, 76% including nurse practitioners, physicians, physician assistants, and physical therapists were aware of the triad, but only 29% were aware of RED-S.20 Only 13% of survey participants indicated feeling confident in treating individuals with RED-S.20 These results are discouraging when considering the critical role of healthcare professionals in promoting health and preventing disease.
Nurse practitioners providing primary care to women should be knowledgeable about the risk factors for and signs of RED-S so they may educate patients, evaluate, treat, and/or make appropriate referrals. A recent study of 1,000 female athletes presenting to medical care found 47% of the sample as having LEA and thus at risk for RED-S.21 Other studies have estimated LEA prevalence ranges from 22% to 58% in various sports.22 Any female athlete is at risk for RED-S. As previously mentioned, LEA also can be observed in nonathletes such as dancers and those involved in physical activity for recreation. RED-S risk is certainly higher among females involved in weight-sensitive sports such as gymnastics, cycling, figure skating, and elite ballet dancing where an athlete’s body weight or physical appearance is important for optimal performance and success.4,7 Screening for RED-S should be a standard part of the physical exam for annual visits with female athletes, especially those involved in endurance sports (eg, running, cycling, rowing, swimming) or females engaged in recreational activities where aesthetics and lean physique are desirable.23 When a female presents with concerns of decreased performance, fatigue, weight loss, recurrent injuries or illnesses, or endocrine dysfunction, the nurse practitioner should further investigate for RED-S and begin screening for health implications related to energy deficiency.
Consider the following case
Brittany is a 32-year-old who presents to your office for her annual well-woman exam. Today her blood pressure is 102/70 mm Hg, pulse 65, weight 103 lbs, height 5’4”, and BMI 17.68. Her last normal menstrual period was 2 months ago. She tells you she occasionally skips a period or two and is not concerned for pregnancy since her husband had a vasectomy after the birth of their second child 2 years ago. You notice that her weight has dropped by 15 lbs since her visit with you a year ago. Over the past year, she has become involved with a local running club. She ran cross country in high school and ran off and on in college and as a young adult to “stay in shape.” She tells you it has been good to get back into running regularly and to do something for herself. She enjoys the competition and accomplishment with training and racing. She is running 35 to 40 miles per week. She tells you that she feels run down and fatigued most days, but she attributes that to being busy with work and taking care of two small children.
The nurse practitioner caring for this patient should recognize the risks and signs of possible energy deficiency in this patient. First, she has lost a significant amount of weight and her BMI is in the underweight range. Second, she is involved in an endurance sport. Third, she is reporting fatigue and irregular periods. The Table shows the important aspects of the history and physical exam for RED-S screening.23,24 All of the tests may or may not be applicable depending on the age, gender, and clinical presentation of the patient. A thorough health history and physical examination, along with appropriate tests, guide the nurse practitioner in discerning other potential causes for the patient’s presenting symptoms and evaluating serious medical consequences resulting from energy deficiency.23,25

Management and treatment
Ideally, the care of an athlete with RED-S is managed with a multidisciplinary team approach. For young athletes, parents or guardians should be involved in care management. Any coaches, athletic trainers, sports medicine physicians, and/or sports dieticians involved with the athlete should be involved in the plan of care. Nonpharmacologic treatment of RED-S includes correction of energy deficiency with dietary changes, modifying exercise regimen, supplementation of vitamins and minerals, namely calcium and vitamin D to support healthy bone development, and cognitive behavioral therapy.7 For competitive athletes, the RED-S Clinical Assessment Tool is available to assess at-risk athletes and assist in informing decisions about athletes returning to play.26 When disordered eating is suspected or other comorbid disorders such as anxiety, depression, or substance abuse are present, the athlete’s treatment plan should be modified to include medical, nutritional, and mental health support.7
In female athletes with amenorrhea for longer than 6 months, it is recommended that a baseline BMD be evaluated with dual-energy X-ray absorptiometry using Z scores rather than T scores.25 Nutritional, exercise, and psychological interventions should be implemented, and the athlete should monitor for the return of normal menstrual function. If menses do not return within 6 to 12 months of implementing nonpharmacologic treatments, the clinician should consider adding pharmacologic therapy.25 Transdermal estrogen and cyclic oral progesterone are recommended to correct functional hypothalamic amenorrhea in the female athlete affected by RED-S.25 Using combined estrogen and progesterone contraception such as oral contraceptive pills (OCPs), the contraceptive patch, or contraceptive vaginal ring to reestablish a normal period in the amenorrheic female athlete is not recommended.25 These methods of contraception do not improve BMD or decrease fracture risk and can mask normal menstrual function.27,28 Transdermal estradiol does not affect the secretion of insulin-like growth factor 1, a bone-trophic hormone that OCPs have been shown to downregulate; thus, transdermal estradiol has a more positive effect on BMD when compared to OCPs.27,28
The issue of oligomenorrhea and amenorrhea being used as a sign to monitor for RED-S is a challenge for girls and women who are using hormonal contraception because the normal function of the menstrual cycle is masked. Female athletes using hormonal contraception should be informed that their menstrual cycle is not a reliable marker for energy availability and that bone loss may continue if the energy deficit is not corrected. Due to this concern, female athletes may consider nonhormonal methods of contraception. In January 2022, US professional middle-distance runner, Colleen Quigley, shared about her decision to use the copper intrauterine device on Instagram.29 Having a normal menstrual period as an indicator of proper fueling and energy availability along with not having hormones potentially to impact her performance and moods were two important factors impacting her contraceptive choice.29 When partnering with female athletes in making sexual and reproductive health decisions, healthcare providers must consider the risk for RED-S as well as contraceptive choice. If a woman prefers to use a hormonal method of birth control for contraception, she should be able to use that method knowing she will need to carefully monitor her health and performance, ensuring she is adequately fueling her body and preventing RED-S. Healthcare providers should monitor the health of female athletes using hormonal contraception using data from the history and physical examination other than the menstrual cycle to screen for RED-S (Table).
Conclusion
Nurse practitioners and other clinicians providing care to women are key in recognizing risks for RED-S and implementing appropriate screening. Healthcare providers can gain rapport with athletes, as well as their families and coaches, by showing interest in the athletes’ training and performance and providing education to promote health. Knowing the risk factors and signs to watch for are imperative for early intervention. Providers should talk to athletes about energy deficiency including the long-term health and athletic performance implications. Incorporating graphics may be helpful when having discussions with athletes about the impact of energy deficiency and symptoms they should watch for and report to their provider.
Healthcare providers can have the greatest impact on the health of female athletes by educating them on the importance of proper fueling with food intake to support energy demands from training. Maintaining a healthy body weight by eating energy-rich proteins and carbohydrates should be encouraged. Providers may employ psychological strategies such as promoting the concept of “eating to perform” to encourage healthy relationships with food so that athletes consume the calories and nutrients needed to support optimal athletic performance. There are many factors to consider when caring for the female athlete including her training regimen, performance goals, underlying physical and mental health, diet, reproductive goals, and contraceptive status. Healthcare providers in women’s health have the unique ability to partner with female athletes in addressing each of these important areas potentially impacted by RED-S. Equipped with education on how to fuel for performance and prevent RED-S, athletes are better able to maintain lifelong physical activity and health.
Further research is needed to better understand the implications of energy deficiency on body systems outside of the triad (ie, gastrointestinal, immunologic, psychological, etc.).30 Research linking direct cause-and-effect relationships between LEA and pathologic effects along with consistent and quantifiable measures of clinical outcomes will strengthen the clinical usefulness of the model.30 Although more needs to be understood about RED-S and science will continue to develop, scientists have already made great discoveries in this field over the past two decades. Sadly, there is a knowledge deficit among clinicians. Research is needed to understand and address knowledge deficits to ensure patients are receiving evidence-based care.
Casey S. Hopkins is Assistant Professor of Nursing at Clemson University in Clemson, South Carolina; a women’s health nurse practitioner in the Division of Pediatric and Adolescent Gynecology, Department of Obstetrics and Gynecology, at Prisma Health-Upstate in Greenville, South Carolina; and Clinical Assistant Professor at the University of South Carolina School of Medicine-Greenville. Chris Hopkins is Assistant Professor in the Department of Health Sciences at Furman University in Greenville. Julie Mackin is a registered nurse at Bon Secours St. Francis Eastside Hospital in Greenville and a graduate student in the Master of Science in Nursing program, Family Nurse Practitioner track, at Clemson University. The authors have no actual or potential conflict of interest in relation to the contents of this article.
References
- Yeager KK, Agostini R, Nattiv A, Drinkwater B. The female athlete triad: disordered eating, amenorrhea, osteoporosis. Med Sci Sports Exerc. 1993;25(7):775-777.
- Nattiv A, Loucks AB, Manore MM, et al. American College of Sports Medicine position stand. The female athlete triad. Med Sci Sports Exerc. 2007;39(10):1867-1882.
- Mountjoy M, Sundgot-Borgen J, Burke L, et al. The IOC consensus statement: beyond the female athlete triad—relative energy deficiency in sport (RED-S). Br J Sports Med. 2014;48(7):491-497.
- Dipla K, Kraemer RR, Constantini NW, Hackney AC. Relative energy deficiency in sports (RED-S): elucidation of endocrine changes affecting the health of males and females. Hormones. 2021;20(1):35-47.
- Jasienska G. Energy metabolism and the evolution of reproductive suppression in the human female. Acta Biotheor. 2003;51(1):1-18.
- Wade GN, Jones JE. Neuroendocrinology of nutritional infertility. Am J Physiol Regul Integr Comp Physiol. 2004;287(6):R1277-R1296.
- Mountjoy M, Sundgot-Borgen J, Burke L, et al. International Olympic Committee (IOC) consensus statement on relative energy deficiency in sport (RED-S): 2018 update. Int J Sport Nutr Exerc Metab. 2018;28(4):316-331.
- Ackerman KE, Nazem T, Chapko D, et al. Bone microarchitecture is impaired in adolescent amenorrheic athletes compared with eumenorrheic athletes and nonathletic controls. J Clin Endocrinol Metab. 2011;96(10):3123-3133.
- Ackerman KE, Putman M, Guereca G, et al. Cortical microstructure and estimated bone strength in young amenorrheic athletes, eumenorrheic athletes and non-athletes. Bone. 2012;51(4):680-687.
- Rickenlund A, Eriksson MJ, Schenck-Gustafsson K, Hirschberg AL. Amenorrhea in female athletes is associated with endothelial dysfunction and unfavorable lipid profile. J Clin Endocrinol Metab. 2005;90(3):1354-1359.
- Melin A, Tornberg AB, Skouby S, et al. The LEAF questionnaire: a screening tool for the identification of female athletes at risk for the female athlete triad. Br J Sports Med. 2014;48(7):540-545.
- Ackerman KE, Holtzman B, Cooper KM, et al. Low energy availability surrogates correlate with health and performance consequences of relative energy deficiency in sport. Br J Sports Med. 2019;53(10):628-633.
- Shimizu K, Suzuki N, Nakamura M, et al. Mucosal immune function comparison between amenorrheic and eumenorrheic distance runners. J Strength Cond Res. 2012;26(5):1402-1406.
- Bomba M, Corbetta F, Bonini L, et al. Psychopathological traits of adolescents with functional hypothalamic amenorrhea: a comparison with anorexia nervosa. Eat Weight Disord. 2014;19(1):41-48.
- O’Donnell E, Goodman JM, Mak S, et al. Discordant orthostatic reflex renin-angiotensin and sympathoneural responses in premenopausal exercising-hypoestrogenic women. Hypertension. 2015;65(5):1089-1095.
- Curry EJ, Logan C, Ackerman K, et al. Female athlete triad awareness among multispecialty physicians. Sports Med Open. 2015;1(1):38.
- Lodge MT, Ackerman K, Garay J. Knowledge of the female athlete triad and relative energy deficiency in sport among female cross-country athletes and support staff. J Athl Train. 2022;57(4):385-392.
- Mukherjee S, Chand V, Wong XX, et al. Perceptions, awareness and knowledge of the female athlete triad amongst coaches – are we meeting the expectations for athlete safety? Int J Sport Sci Coach. 2016;11(4):545-551.
- Pantano KJ. Knowledge, attitude, and skill of high school coaches with regard to the female athlete triad. J Pediatr Adolesc Gynecol. 2017;30(5):540-545.
- Tenforde AS, Beauchesne AR, Borg-Stein J, et al. Awareness and comfort treating the female athlete triad and relative energy deficiency in sport among healthcare providers. Dtsch Z Sportmed. 2020;71:76-80.
- Ackerman KE, Holtzman B, Cooper KM, et al. Low energy availability surrogates correlate with health and performance consequences of relative energy deficiency in sport. Br J Sports Med. 2019;53(10):628-633.
- Logue DM, Madigan SM, Melin A, et al. Low energy availability in athletes 2020: an updated narrative review of prevalence, risk, within-day energy balance, knowledge, and impact on sports performance. Nutrients. 2020;12(3):835.
- Statuta SM, Asif IM, Drezner JA. Relative energy deficiency in sport (RED-S). Br J Sports Med. 2017;51:1570-1571.
- Holtzman B, Ackerman KE. Recommendations and nutritional considerations for female athletes: health and performance. Sports Med. 2021;51(suppl 1):43-57.
- Cobb KL, Bachrach LK, Sowers M, et al. The effect of oral contraceptives on bone mass and stress fractures in female runners. Med Sci Sports Exerc. 2007;39(9):1464-1473.
- Mountjoy M, Sundgot-Borgen J, Burke L, et al. The IOC relative energy deficiency in sport clinical assessment tool (RED-S CAT). Br J Sports Med. 2015;49(21):1354.
- Ackerman KE, Singhal V, Slattery M, et al. Effects of estrogen replacement on bone geometry and microarchitecture in adolescent and young adult oligoamenorrheic athletes: a randomized trial. J Bone Miner Res. 2020;35(2):248-260
- Gordon CM, Ackerman KE, Berga SL, et al. Functional hypothalamic amenorrhea: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2017;102(5):1413-1439.
- @Steeple squigs. Just FYI, this post is about periods and IUDs. January 6, 2022.
- De Souza MJ, Strock NCA, Ricker EA, et al. The path towards progress: a critical review to advance the science of the female and male athlete triad and relative energy deficiency in sport. Sports Med. 2022;52(1):13-23.
Key words: RED-S, energy deficiency, sports, female athletes, female athlete triad, nurse practitioners
Womens Healthcare. 2022;10(4):38-45. doi:10.51256/WHC082238