
An estimated 84% of adults experience symptoms related to low back pain (LBP) at some point in their lives.1 Acute LBP is most commonly encountered in women and is usually self-limiting.2 Research suggests that LBP in women increases with age and is the leading cause of disability in women globally.2,3 Moreover, it is often a condition that is underdiagnosed and therefore undertreated.3 This article provides a practical approach for nurse practitioners (NPs) to assess LBP, diagnose the underlying etiology or etiologies, use evidence-based management for commonly observed causes of LBP, and make referrals as needed.
Overview
Low back pain may be mechanical, neuropathic, degenerative, myofascial, or neoplastic and is typically categorized by the length of time symptoms are endured.4 Acute pain persists for less than 4 weeks; subacute pain between 4 and 12 weeks; and chronic pain for 12 weeks or more.1 Common risk factors associated with LBP include obesity, age, smoking, sedentary work, a strenuous job, anxiety and depression symptoms, job dissatisfaction, lower education attainment, workers’ compensation insurance, and female gender.1 Most LBP is not of a serious etiology but still can be debilitating, with loss of productivity and decreased quality of life. Etiologies frequently observed among women in the primary care setting are related to either musculoskeletal injury, urogynecologic pathology, pregnancy-related changes, or nonspecific causes. Those which are musculoskeletal in nature could be secondary to acute events such as when straining to lift heavy objects or could occur over time with repetitive use from activities such as gardening or playing sports. The term nonspecific LBP is often used when a specific cause has not been identified and does not indicate that a cause does not exist.4 Accurately diagnosing the cause of LBP requires a thorough history, a skilled physical examination, and if indicated, diagnostic testing. While patients with a serious etiology may initially present to the emergency department or to a specialist, many prefer to first seek medical attention from those whom they know and trust. LBP can be challenging to manage and often the best response is achieved with a multimodal approach.5,6
Assessment and diagnosis
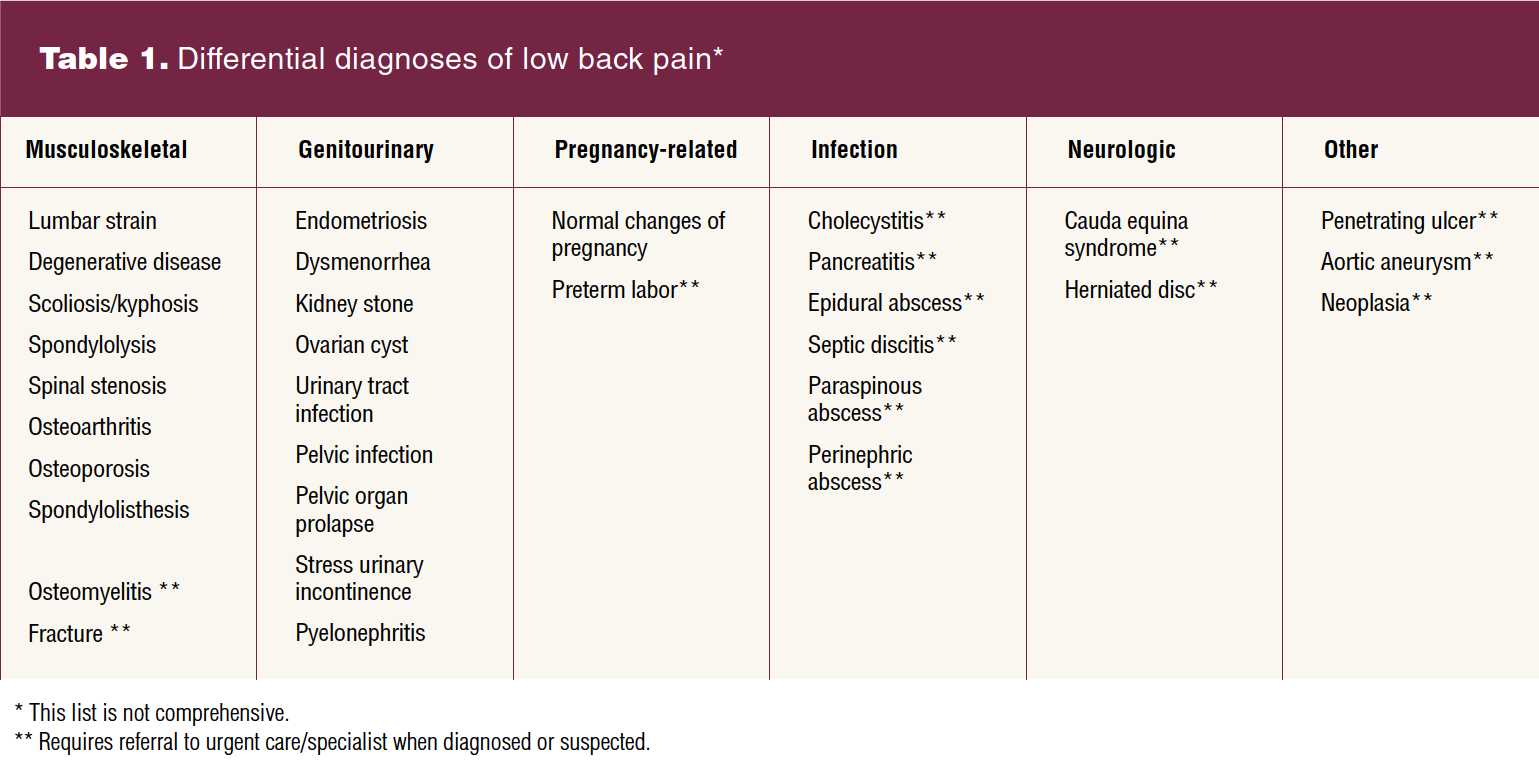
A lengthy list of etiologies are related to LBP, thus leading to numerous potential differential diagnoses (DDs). In addition to musculoskeletal, neoplastic, inflammatory, and infectious causes of LBP, women may experience referred pain with pelvic, renal, and gastrointestinal disorders that can manifest as this condition. Nurse practitioners in women’s health should be familiar with DDs associated with LBP. Table 1 provides a summary of the differential diagnoses.
Assessment begins with a detailed history including questions to ascertain the onset, location, character, and severity of the pain. Moreover, it is important to understand what exacerbates their symptoms and what makes it better. Examples of questions routinely asked during the assessment include the following: Does it radiate? Is it affected by position? Are there any associated manifestations such as numbness, tingling, fever, night sweats, or loss of bowel or bladder control? Because pain is subjective, the numeric rating scale (0–10) is most often used to rate pain, although pictorial depictions such as the Wong-Baker FACES pain rating scales may be more beneficial for some patients. Noting the effects of pain on activities of daily living and quality of life is particularly important when determining clinical outcomes and efficacy of treatment.1 Screening for depression and anxiety is relevant as these conditions can contribute to or be a result of LBP and can increase the risk for acute pain to become chronic.4
The physical examination should include both musculoskeletal and neurologic assessments and should be performed using a systematic approach. Begin with gait assessment and visualization of the back, observing their posture and looking for any asymmetry, obvious swelling, or muscle atrophy. Next, palpate key structures for tenderness or masses including along the spinous processes, paraspinal muscles and other soft tissues, and over the sacroiliac joints. Percuss over the costovertebral area to assess for a potential renal etiology and consider performing a pelvic examination if a patient complains of pain radiating between the back and the pelvis. Assessing active range of motion is achieved by asking the patient to bend forward, then backward, and finally to the left and right sides. The examiner should not only assess degree of mobility but also should ask about any associated pain or reproduction of symptoms with these movements. Neurologic examination includes assessment of bilateral lower extremity strength using the Medical Research Council Manual Muscle Testing scale, rating strength of each muscle group 0–5, assessment of sensation, and deep tendon reflexes.8 Dural tension tests such as the straight leg raise (SLR), which is performed with the patient lying supine, or the slump test, which is a modified SLR in a sitting position are important to perform, as pain with these maneuvers suggests nerve root impingement. Other special tests such as FABER [flexion, abduction, external rotation of the hip] are helpful for determining if there is sacroiliac joint pathology.7 All of these findings, along with the history obtained, provide insight into diagnosis because the clinical presentation may vary based on the underlying pathogenesis.4,8
The NP in a primary care setting can exclude emergent conditions as causes for LBP and those requiring advanced diagnostic testing and make expedited referrals when indicated. Determining the cause of LBP can require the use of laboratory and diagnostic tools, some of which can be initiated in the primary care setting. For example, the patient presenting with LBP accompanied by urinary symptoms may necessitate a urinalysis and/or urine culture and sensitivity. Sexually transmitted infection screening or pelvic examination may be appropriate in some cases. A kidney, ureter, and bladder x-ray may be ordered for the patient with hematuria and a history of kidney stones. Plain radiographs of the lumbar spine may be indicated following acute trauma or for patients with bony tenderness on exam.
Emergent referral for specific signs and symptoms associated with LBP is critical. Loss of bowel or bladder control could indicate cauda equina syndrome, recent infection with fever could indicate epidural abscess or discitis, and the inability to ambulate accompanied by decreased sensation or paresthesia in the lower extremities could indicate central canal stenosis and/or cord compression.7,8 Patients presenting with these red flag symptoms should be immediately referred to the emergency department for evaluation, which may include advanced diagnostic imaging (eg, magnetic resonance imaging or computed tomography).
Special considerations apply when assessing the patient during pregnancy. The growing uterus along with weight gain misplace the center of gravity and thus place more stress on muscles and joints. Moreover, increases in hormones such as progesterone and relaxin may cause the sacroiliac joints and the posterior ligament to become lax, thereby affecting stability and contributing to LBP.9 Specific radiographic imaging is not indicated in pregnant patients with LBP unless an obstructing kidney stone is suspected based on a thorough history and physical examination. Finally, the NP should assess for preterm labor and ask about pelvic pain, as both pelvic pain and LBP may be related to widening of the pelvis.
Select LBP causes and assessment findings
Lumbosacral strain
Lumbosacral strain represents the most common musculoskeletal cause of acute LBP and can be differentiated from other causes using the described history and physical examination components. Lumbosacral strain results from stretching or tearing of muscles, tendons, ligaments, and fascia due to trauma or repetitive mechanical stress. Pain is often described as being located in the lower back or buttocks and characterized as a spasm or aching. The pain does not radiate into the lower extremities. The patient with lumbosacral strain may have increased pain with back flexion and possible tenderness over the paraspinal muscles. An SLR will be negative, and the neurologic examination will be normal.4
Herniated intervertebral disc
In contrast to lumbosacral strain, LBP due to a herniated intervertebral disc may be felt in the buttocks or radiating to a lower extremity below the knee (radicular pain) and characterized as sharp, burning, or shooting. Pain may be exacerbated by maneuvers that increase intra-abdominal pressure such as straining with a bowel movement. The patient may have numbness or tingling over the associated nerve root. An SLR is likely to be positive. There may be weakness, loss of sensation, and diminished reflexes in aspects of the foot depending on the affected nerve root.4,7
Spinal stenosis
Spinal stenosis is more common in individuals older than age 50 years, whereas a herniated intervertebral disc is seen more often in the 20- to 40-year-old age group.4,7 Spinal stenosis can cause chronic mechanical compression resulting in muscle pain and nerve root compression. Pain is usually bilateral (as it involves both the back and legs), aggravated by walking and standing, and alleviated by bending forward. The patient may have a wide-based gait and assume a kyphotic (flexed lumbar spine) to alleviate pain. Weakness and diminished reflexes may be present depending on nerve root involvement. An SLR may be positive but is less reliable than with a herniated disc.4,7
Treatment options
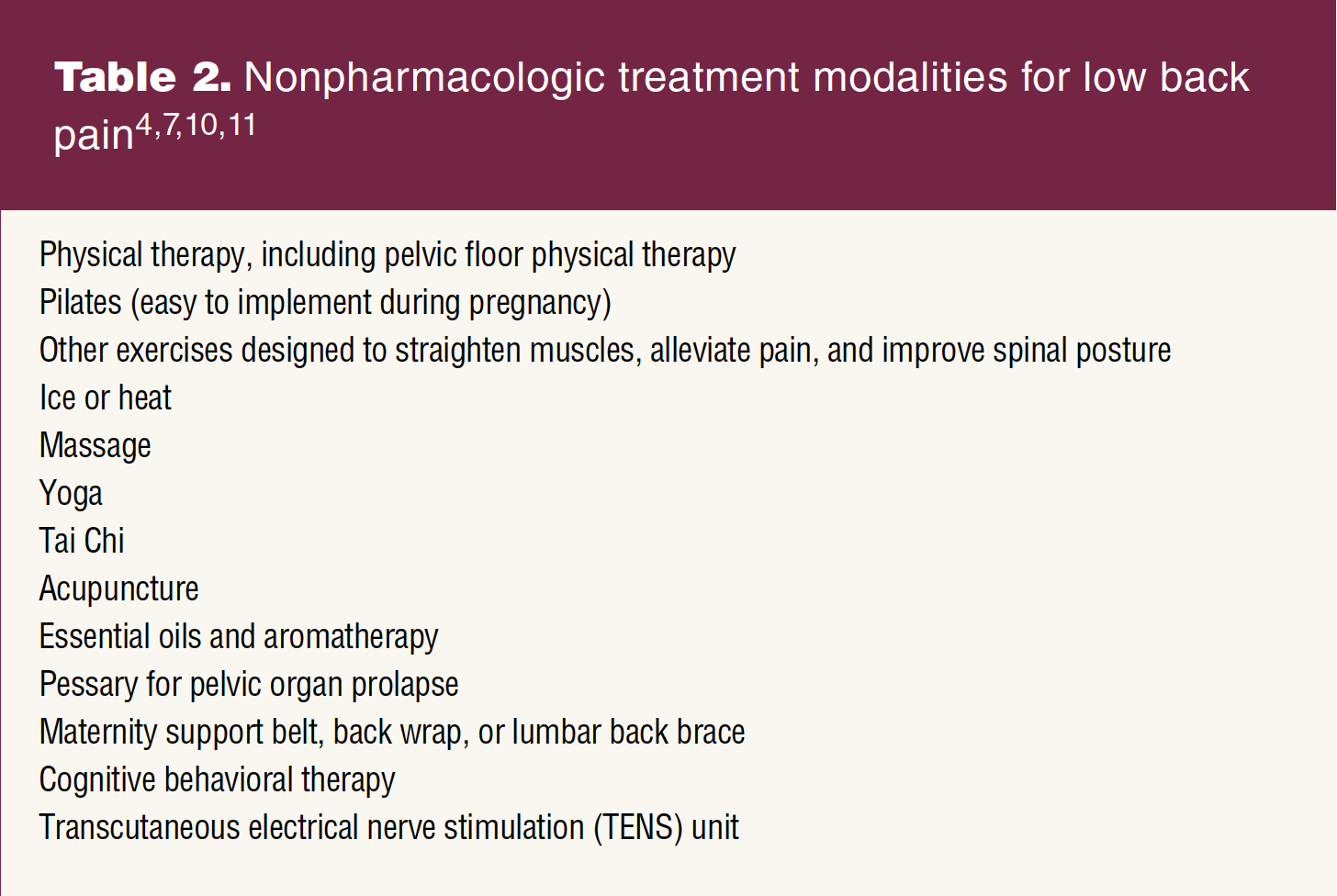
Multimodal treatment is typically necessary to relieve LBP and depends on etiology of the pain. Commonly used treatment options for lumbar strain or nonspecific LBP include physiotherapy, exercise, complementary alternative therapies, and pharmacologic interventions.10 Nonpharmacologic treatment is the initial recommendation for acute and subacute LBP in the absence of any red flags based on the applicable clinical practice guidelines. Pilates exercise focuses on active use of the core muscles for lumbar stabilization and has been found to decrease LBP.11 Acupuncture and aromatherapy have been useful for treatment of LBP during pregnancy.10 Table 2 provides a list of specific nonpharmacologic modalities. If pain is not relieved with nonpharmacologic modalities, pharmacologic interventions are considered. Options include nonsteroidal anti-inflammatory drugs (NSAIDs), acetaminophen, muscle relaxants, and topical lidocaine.4,7 NSAIDs should not be used in the first and third trimesters and muscle relaxants should be avoided. Muscle relaxants should be used with caution in older individuals and those at risk for falling as they have a central-acting sedative effect.7 The NP in the primary care setting does not typically prescribe narcotics for LBP. Patients with chronic LBP not relieved by the recommended treatment modalities and for whom low-dose, short-acting, short-term opioids are considered are best managed within a pain management specialty team.
Patient education and follow-up
Low back pain is usually self-limiting and therefore reassurance should be provided to patients. It is important to encourage patients to avoid activity that could exacerbate their pain and to discourage prolonged bedrest.4,7 Maintaining a healthy weight, stretching, regularly exercising, and utilizing proper body mechanics when lifting objects are all preventive measures to avoid LBP. Follow-up is not necessarily required unless there is no improvement or if there is worsening of symptoms. If pain does worsen or persists, consider a referral to a specialist. Advise patients with LBP about red flags that require immediate attention (eg, loss of bowel or bladder control, urinary retention, weakness in lower extremities, persistent or high fever, worst pain at rest or night).4 Evidence-based patient education is available on these websites:
American College of Obstetricians and Gynecologists: Back Pain During Pregnancy;
American College of Obstetricians and Gynecologists: Back Pain;
and American Academy of Family Physicians: Low Back Pain.
Conclusion
Given that all women are at risk for experiencing LBP at some point across their lifespan, NPs should remain vigilant and knowledgeable about the current evidence supporting safe, effective, and efficient care of women experiencing LBP symptoms. They are strategically positioned to provide primary care to women experiencing LBP that can positively impact overall quality of life.
Christy D. Martin is Adjunct Instructor at the University of Alabama at Birmingham School of Nursing in Birmingham, Alabama. M. Heath Hale is Associate Professor at the University of Alabama at Birmingham School of Medicine and Department of Family and Community Medicine, UAB Student Health and Wellness. Aimee C. Holland is Professor at the University of Alabama at Birmingham School of Nursing and UAB Student Health and Wellness. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(1):36-40. doi: 10.51256/WHC022336
References
1 Song C-Y, Chen C-H, Chen T-W. Assessment of low back pain: reliability and minimal detectable change of the brief pain inventory. Am J Occup Ther. 2022;76(3):7603205040.
2 Centers for Disease Control and Prevention. QuickStats: Percentage of adults aged ≥18 years who had lower back pain in the past 3 months, by sex and age group — National Health Interview Survey, United States, 2018. MMWR Morb Mortal Wkly Rep 2020;68:1196.
3 Prego-Jimenez S, Pereda-Pereda E, Perez-Tejada J, et al. The impact of sexism and gender stereotypes on the legitimization of women’s low back pain. Pain Manag Nurs. 2022;23(5):591-595.
4 Knezevic NN, Candido KD, Vlaeyen JWS, et al. Low back pain. Lancet. 2021;398(10294):78-92.
5 Urits I, Burshtein A, Sharma M, et al. Low back pain, a comprehensive review: pathophysiology, diagnosis, and treatment. Curr Pain Headache Rep. 2019;23(3):23.
6 Dupuis M, Duff E. Chronic low back pain: evidence-informed management considerations for nurse practitioners. J Nurse Pract. 2022;15:583-587.
7 Hemmer CR. Evaluation and treatment of low back pain in adult patients. Orthop Nurs. 2021;40(6):336-342.
8 Patel EA, Perloff MD. Radicular pain syndromes: cervical, lumbar, and spinal stenosis. Semin Neurol. 2018;38(6):634-639.
9 Berber MA, Satılmış İG. Characteristics of low back pain in pregnancy, risk factors, and its effects on quality of life. Pain Manag Nurs. 2020;21(6):579-586.
10 Hughes C, Liddle SD, Sinclair M, McCullough JEM. The use of complementary and alternative medicine (CAM) for pregnancy related low back and/ or pelvic girdle pain: an online survey. Complement Ther Clin Prac. 2018;31:379-383.
11 Octaviani I. Pilates workouts can reduce pain in pregnant women. Complement Ther Clin Prac. 2018;31:349-351.
Key words: low back pain, women’s health, primary care, pregnancy