
Perinatal depression is the most common complication of pregnancy, with a higher incidence than gestational diabetes, preeclampsia, or preterm birth. Perinatal depression affects 1 of every 7 women.1 Antenatal depression is a significant risk factor for postpartum depression and, if left untreated, increases risk for preterm birth, low birth weight, preeclampsia, excess gestational weight gain, and operative delivery while decreasing rates of breastfeeding.2,3
The American College of Nurse Midwives recommends midwives integrate prevention, universal screening, treatment, and/or referral for depression into the care they provide for women.4 The American College of Obstetricians and Gynecologists, the US Preventive Services Task Force, and the American Academy of Family Physicians recommend screening all pregnant and postpartum women for depression and stress that screening should be implemented only when adequate systems are in place to ensure accurate diagnosis, effective treatment, and appropriate follow-up.5–7
A survey of 53 certified nurse midwives in Oregon showed that although 94% screened for prenatal depression, only 53% had a formalized screening process in place.8 A national survey of obstetricians and gynecologists reported that 53% universally screened pregnant patients for depression, but only 33.67% implemented guideline-congruent care.9
The Council on Patient Safety in Women’s Health Care, a multidisciplinary collaboration of organizations across the spectrum of women’s health, developed the Maternal Mental Health Patient Safety Bundle in 2016. The bundle has four key components: readiness, recognition and prevention, response, and reporting and systems learning. Patient safety bundles are developed to provide a small set of evidence-based interventions to achieve improved outcomes. They are based on the concept that when care processes are grouped into simple bundles, healthcare providers are more likely to implement them by making fundamental changes in how they work.10
Project purpose
The purpose of this DNP quality improvement (QI) project was to utilize the Maternal Mental Health Patient Safety Bundle to design and implement a universal perinatal depression screening and response protocol within a Federally Qualified Health Center (FQHC) in central Ohio. The goal was to increase the rate of screening and referral for depressive symptoms among pregnant and postpartum individuals. Prior to implementation, the FQHC site did not have a standardized process in place to ensure timely diagnosis, effective treatment, and follow-up for perinatal depression.
Description of the setting and population
The site for this project was a nurse-practitioner–led FQHC in an urban area in central Ohio. The implementation site provided prenatal care to women who lived predominantly in one county, with 65% of pregnant patients being low-income Black women. The age range for the perinatal population was from 15 to 44 years, with 74% of women falling between the ages of 20 and 29 years.
A low volume of perinatal patients was seen at the site, typically 30 to 35 patients each week with 110 births per year. Three certified nurse midwives provided perinatal care and a unique multidisciplinary team consisting of a counselor, social worker, psychiatric mental health nurse practitioner, family nurse practitioners, and a community health worker worked at the site.
Description of the quality improvement project
An evidence-based perinatal depression screening and response protocol was developed based on recommendations from the Maternal Mental Health Safety Bundle. Education on use of the protocol was given to all providers and staff via a 30-minute PowerPoint presentation. The screening aspect of the protocol called for administration of the Edinburgh Postnatal Depression Scale (EPDS) to all patients at initial, 24- to 28-week gestation, and postpartum visits. The response aspect of the protocol required a referral to a mental health provider for any EPDS score of 14 or greater, indicating the patient is at risk for or has symptoms of moderate-to-severe depression. All patients with an EPDS score of more than 6 were scheduled to have a repeat screen at the following visit. The project was implemented over an 8-week period of time. This QI project was determined to be exempt by the Ohio State University human subjects assessment process and did not require Institutional Review Board review.
Methods to evaluate outcomes
Patient charts were reviewed before and after implementation to monitor rates of perinatal depression screening and referral. Data collection was done by chart review and a case management log. Six months of patient charts were reviewed for baseline data. This included descriptive statistics such as age, race, screenings completed, number of positive screens, the response to positive screens, and referrals made and completed. After project implementation, this same data was collected for 8 weeks to assess provider adherence to the protocol. All patient charts that demonstrated a positive screen (EPDS > 6) were reviewed for appropriate diagnosis added to the electronic medical record (EMR) problem list, documentation of education, and, if required, a completed referral to a mental health provider.
Outcomes
A total of 50 perinatal patients were screened during the 8-week implementation of the protocol.
As shown in Table 1, implementation of the protocol increased rates of screening from 92.5% to 94% at the new patient visit and from 0% to 92% at the 24- to 28-week prenatal visit. Screening rates remained stable at 100% pre- and post-implementation for all postpartum visits. During implementation, two patients were not screened: one at the initial visit and one at the 24- to 28-week visit. Both patients were non-English speaking with no EPDS readily available for their language. As shown in Table 2, the percentage of positive depression screens decreased pre- to post-QI project.
Table 1. Rates of depression screening by visit type pre- and post-quality improvement
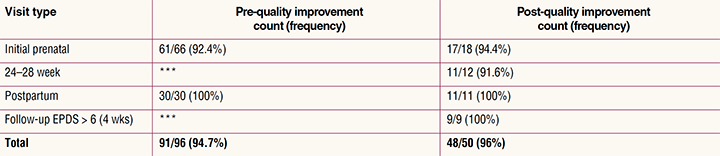
EPDS, Edinburgh Postpartum Depression Scale.
***No screenings done at this time period.
Note: The pre-quality improvement data spanned 6 months while the post-quality improvement data spanned 8 weeks.
Table 2. Elevated depression screens by visit type pre- and post-quality improvement
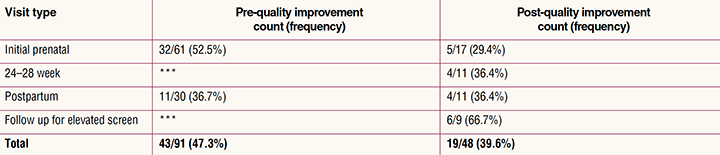
***No screenings done at this time period.
Note: A score of > 6 on the Edinburgh Postpartum Depression Scale was considered to be an elevated depression screen; the pre-quality improvement data spanned 6 months while the post-quality improvement data spanned 8 weeks.
As shown in Table 3, referral rates increased from 18.6% to 26.3% for women with elevated EPDS scores indicating symptoms of depression (> 6). This represents a 41.4% increase in clinic referrals. It is important to note that there were nine patients who had follow-up appointments during the 8-week project who were re-screened per the new perinatal depression screening and response protocol. Women were re-screened if their EPDS score on a prior visit was more than 6. Of the nine patients, six had scores that remained elevated and four of the six agreed to a referral for counseling. The highest percentage of referrals occurred in this follow-up screening group. This screening time frame was new for the practice and highlights the importance of follow-up for women who have elevated EPDS screens.
Table 3. Referral rates for elevated depression screens pre- and post-quality improvement

EPDS, Edinburgh Postpartum Depression Scale.
Note: The pre-quality improvement data spanned 6 months while the post-quality improvement data spanned 8 weeks.
Discussion and implications for practice
Early identification of depression during pregnancy and postpartum offers an opportunity for providers to discuss symptoms of depression and refer patients for counseling and treatment. It has long been recognized that standardization of healthcare processes and reduced variation improves outcomes and quality of care.10 This DNP project demonstrated that standardization in the form of an evidence-based protocol increased the rate of depression screening and increased referrals to a mental health specialist for treatment. This project also demonstrates the need for multiple screening points during and after pregnancy with follow up for those with elevated EPDS scores.
Facilitators of this project included the unique makeup of the FQHC, midwives with additional mental health training and supportive administration and staff. The project had no negative finanacial impact and minimal workflow changes. The ability to refer for mental health services to the clinic’s imbedded mental health counselor or psychiatric mental health nurse practitioner allowed successful implementation of the screening and response protocol.
Barriers encountered during implementation of this QI project included a provider resignation that resulted in missed opportunities for screening due to increased workload on the remaining providers and the need to orient a new provider. Another challenge was patient language barriers. The clinic did not have the EPDS readily available in all languages of the clinic population. An additional barrier was the EMR. Specifically, documentation of an EPDS score is cumbersome and an elevated score does not “trigger” additional documentation or action. This issue provides an excellent future opportunity to create a clinical decision support aid within the EMR for a perinatal depression screening and response protocol.
Conclusion
Limitations
The implementation and further evaluation of this protocol warrants consideration at additional sites over a longer time period and with a larger number of providers and patients. After completion of this project, there are some questions that need additional research for evidence-based solutions. What are other interventions for women who score in the “at risk for depression” EPDS range (7–13)? Is giving a handout on resources enough? Another question is how many times should this screen be repeated if the scores remain elevated before recommending a patient for further evaluation by a mental health provider? What are the barriers to patient’s acceptance of a referral? What interventions increase referral acceptance rates?
In conclusion, the utilization of bundles and the standardization of care improve patient outcomes. Implementing evidence-based perinatal depression screening protocols into practice is essential. The evidence-based screening and response protocol presented here can be utilized by obstetric providers to improve the care delivered to perinatal women in regard to screening for depression during and after pregnancy.
Lucia M. Jenkusky is Assistant Professor of Clinical Practice, Director of the Nurse-Midwifery and Women’s Health Specialty Tracks, and Director of The Ohio State University Total Health and Wellness, Women’s Health Services, in Columbus, Ohio. Barbara Jones Warren is Professor of Clinical Nursing and Director of the Psychiatric Mental Health Nurse Practitioner Specialty Track at the Pitzer Center for Women, Children, and Youth; Randee L. Masciola is Assistant Professor of Clinical Nursing and Doctorate of Nursing Practice Program Director, Clinical Expert; and Shannon L. Gillespie, PhD, RN, is Assistant Professor at the Pitzer Center for Women, Children, and Youth, all at the College of Nursing, The Ohio State University. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
References
- Ashley JM, Harper BD, Arms-Chavez CJ, LoBello SG. Estimated prevalence of antenatal depression in the US population. Arch Womens Ment Health. 2016;19(2):395-400.
- Biaggi A, Conroy S, Pawlby S, Pariante CM. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J Affect Disord. 2016;191:62-77.
- Atwood AL. Antenatal anxiety: origins, effects, and interventions. Internl J Childbirth Educ. 2013;28(3):54-60.
- American College of Nurse-Midwives. Position Statement, Depression in Women. Updated May 2013. http://www.midwife.org/ACNM/files/ACNMLibraryData/UPLOADFILENAME/000000000061/Depression%20in%20Women%20May%202013.pdf.
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion No. 757: Screening for perinatal depression. Obstet Gynecol. 2018;132(5):e208-e212.
- US Preventive Services Task Force. Final Recommendation Statement. Depression in Adults: Screening. January 26, 2016. https://www.uspreventiveservicestaskforce.org/uspstf/document/RecommendationStatementFinal/depression-in-adults-screening.
- American Academy of Family Physicians. Clinical Preventive Service Recommendation. Depression. 2018. https://www.aafp.org/patient-care/clinical-
recommendations/all/depression.html. - Rompala KS, Cirino N, Rosenberg KD, et al. Prenatal depression screening by certified nurse-midwives, Oregon. J Midwifery Womens Health. 2016;61(5):599-605.
- Fedock GL, Alvarez C. Differences in screening and treatment for antepartum versus postpartum patients: are providers implementing the guidelines of care for perinatal depression? J Womens Health. 2018;27(9):1104-1113.
- Council on Patient Safety in Women’s Health Care. Maternal mental health: Depression and anxiety. Perinatal depression and anxiety patient safety bundle. 2016. https://safehealthcareforeverywoman.org/patient-
safety-bundles/maternal-mental-health-depression-
and-anxiety/#link_acc-1-3-d.