
DV, a 22-year-old Black female, presented to the urgent care clinic with complaints of severe headache centered in the occipital area, bilateral eye pain, blurred vision, with associated nausea and vomiting. Vital signs showed blood pressure of 140/90 mm Hg, heart rate of 118, respiratory rate of 28, and a temperature of 98.8°F, and body mass index (BMI) was 31.6. A complete blood count was normal, and there were no electrolyte abnormalities on the basic metabolic profile. DV reported this headache had been escalating over a 6-week period and, at this visit, rated her pain as 10 on a scale of 1 to 10. She had received treatment in the emergency room the prior week for a suspected sinus infection. There was also record of a 2-week course of prednisone prescribed by a different urgent care for these same complaints. She reported the headache had not improved with these interventions and had continued to increase in severity. Additionally, she was having trouble with daily activities and nursing school studies due to double vision, blurriness, and pulsatile tinnitus. DV used no prescription medications and denied the use of any recreational drugs. She did note that she had a levonorgestrel intrauterine device (IUD) inserted about 16 months ago for birth control. She had been rotating acetaminophen and ibuprofen for headache relief with a modest decrease in pain level from 9 to 7. At night, she was taking an over-the-counter acetaminophen sinus and cough remedy for sleep. A review of systems revealed no history of surgical or medical problems.
Physical assessment findings
The patient had visual field deficits with cranial nerve 6 paresis and bilateral double vision. A funduscopic exam was deferred because the patient reported photophobia. Mental status was oriented but answers to questions were brief. Gait and speech were normal. There was mild nuchal rigidity but no positive Kernig’s sign or Brudzinski’s sign. The patient vomited when abdominal palpation was performed. There were no enlarged lymph nodes, masses, or redness about the head and neck. The patient’s throat was without swelling, exudate, or erythema. The frontal sinuses were tender to palpation.
Discharge instructions included to continue over-the-counter ibuprofen and acetaminophen and included an explanation that excessive use could cause a medication overuse headache. An intravenous dose of promethazine and ketorolac was administered. She was observed for 30 minutes and reported the pain level decreased to 5. She was instructed to follow up with a primary care provider.
Patient’s perception
The patient’s perception of her multiple (three) urgent care visits and (three) ED visits, each to a different site, was that she was labeled as drug seeking. She chose different sites because she believed if she kept asking that someone would care enough to see her pain. She felt her providers did not listen respectfully to her complaints. The providers seemed impatient and doubted the severity of the headache. Some providers did not provide eye contact. It is her perception that there was a lack of empathy due to her racial background, which differed from her providers. One provider believed that she had a stress headache due to being a student nurse in final exams week. Her persistence in seeking care resulted in multiple bruises on her arms from laboratory draws and intravenous line insertions. One provider focused history questioning exclusively on possible endocarditis due to the needle-associated vascular damage. All the follow-up instructions at each ED and urgent care referred her to find a primary care provider. However, the earliest appointment for primary care was more than 1 month out from her acute headache episode.
Red flags in the assessment of acute headaches
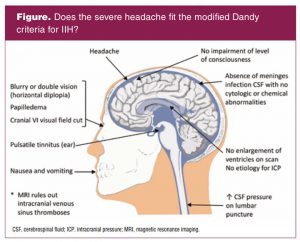
Assessment of acute headache must include the differential diagnosis of sinus thrombosis, meningitis, stroke, cranial nerve 6 palsy, atypical migraine, and idiopathic intracranial hypertension (IIH). Idiopathic intracranial hypertension is a disorder that is diagnosed by exclusion plus evaluation of the symptoms by use of the Dandy criteria (Figure).1
Even with photophobia, an eye examination for papilledema is paramount in making an accurate diagnosis.
Diagnosis and management
DV decided to have an ocular exam because of increasing visual problems and saw an optometrist the day after the visit to urgent care. The optometrist then made an urgent referral to an ophthalmologist. The ophthalmologist noted bilateral papilledema and consulted a neurosurgeon asking him to admit DV for a magnetic resonance imaging (MRI) scan, removal of the IUD, and checking intracranial pressure by lumbar puncture. The ophthalmologist reported that he had seen three other young women with levonorgestrel IUDs who also had problems with increased intracranial pressures.
The opening pressure for the lumbar puncture was greater than 45, and the cerebrospinal fluid (CSF) was clear with normal chemistry. The MRI revealed no abnormalities of the brain ventricles or presence of a tumor. The IUD was removed with the patient’s consent. DV was admitted to the neurocritical care unit with a diagnosis of IIH. She was treated with acetazolamide 1,000 mg every 12 hours for 72 hours and hourly neurologic checks. Acetazolamide is a carbonic anhydrase inhibitor medication and observational evidence supports that the drug reduces the rate of CSF production.2–4 Prior to administering this medication it was confirmed that the patient did not have sulfa allergy, important because cross sensitivities have occurred.2 Her pain and vision changes resolved over a 1-week period as intracranial pressures gradually normalized. She was discharged after 5 days but continued to be followed by the ophthalmologist until total resolution of her visual complaints. DV was also advised to see her primary care provider to discuss contraceptive options.
Since her experience, DV has been speaking to other nurses about the importance of an eye exam when a headache is not resolving in a timely manner. She estimates that she was examined by 10 healthcare providers prior to receiving the correct diagnosis. She is grateful to not have been one of the IIH patients who have experienced permanent vision loss due to unnecessary delay in diagnosis. She is aware that weight loss can diminish the symptoms and that about 8% of patients may have a reoccurrence.4 The patient requested the nurse authors to publish her experience because she had additional persons in her community circle who also had this diagnosis. One is permanently blind due to prolonged delay to diagnosis. Prior to initiating this case report, signed informed consent was obtained and Institutional Review Board approval was completed.
Idiopathic intracranial hypertension
Idiopathic intracranial hypertension occurs when there is an imbalance in the normal production and reabsorption of CSF without ventricular enlargement, tumor, or infection.2–5 This disorder can be induced by medications and is then classified as a drug-induced disease. It may also manifest without an identifying trigger.5 Historically, IIH has been called different names such as pseudotumor cerebri and benign intracranial hypertension. Changing terminology indicates that the pathophysiology is not well delineated.4 The currently preferred hypothesis is that there is dural sinus obstruction due to compression within the abdominal compartment, which leads to decreased CSF resorption.1,5,6 The symptoms most closely mimic the presentation of a dural sinus thrombosis. The healthcare provider should rule out a sinus thrombosis by imaging prior to making the IIH diagnosis.
This disorder is considered rare, but the incidence is increasing and linked to the increasing BMI in the United States population.5 IIH patients are typically women of reproductive age who have high BMI. The incidence with a BMI greater than 30 is 13 to 19 per 100,000.5,7,8 A systematic review completed in 2020 pertinent to drug-induced IIH found that predominantly cases were associated with vitamin A derivatives, tetracycline antibiotics, and lithium.5 This systematic review also contained case reports of progestin-only contraceptives and combined oral contraceptive-associated IIH but noted a weaker association.5 A case-control design study stated in the data analysis that combined oral contraceptives are not a stimulus of IIH.7 One article links IIH to hormonal cross talk of abdominal adipokines and steroid hormones.9 At this time, there is no consensus in the literature concerning the association between hormonal contraception and development of IIH.
Implications for women’s healthcare
Although the etiology of IIH is unknown, the incidence is increasing. The typical presentation is that of a woman of reproductive age with an increased BMI (> 30).8 Earlier diagnosis results in earlier treatment and prevention of long-term sequelae including permanent visual impairment. Therefore, recognition and intervention are tantamount priorities for the healthcare provider caring for this population.2
Most patients with IIH present with headaches and elevated BMI. Loss of visual fields, tinnitus, dizziness, nausea, vomiting, lethargy, and neck pain/stiffness may also be present less commonly.2 The defining characteristic of IIH is papilledema. All women presenting with severe and/or persistent headache should undergo a funduscopic exam to evaluate for papilledema.6 This is of particular importance in reproductive-age women with increased BMI, vision changes, and/or other red flags for a secondary cause of a headache. Suspected papilledema should always be confirmed through formal ophthalmic evaluation and examination.2 Once papilledema is established, further evaluation is necessary to confirm the diagnosis of IIH and allow for adequate treatment. Although it is necessary to rule out other etiologies of papilledema through imaging, the most common etiology in this demographic is IIH.6
Once a diagnosis of IIH is confirmed and treatment is initiated, the women’s healthcare provider is faced with concerns over contraceptive options for the patient. Levonorgestrel IUDs are highly effective and safe contraceptive options for most women. The levonorgestrel is released by the IUD locally to the endometrium with minimal systemic absorption. Serum absorption levels are so low that they do not reach the threshold for ovulation suppression and most women continue to ovulate normally. This results in normal cyclic hormonal activity despite endometrial progestational effect.10
Case reports have questioned the connection between levonorgestrel IUDs and IIH. Although data from some studies have demonstrated an increase of IIH reported in progestin users including those with IUDs, the numbers are limited given the vast number of users of these methods.11 In 2019, all lawsuits regarding IIH against the manufacturer of the most common progestin-releasing levonorgestrel IUD in the US were dismissed due to lack of sufficient evidence.12 It is not clear that the levonorgestrel IUD is a factor in the etiology of IIH, and removal is not recommended or required.13 Progestin-only methods including levonorgestrel IUDs can be a popular contraceptive choice for women with increased BMI if they have other risk factors that make estrogen-containing methods less desirable.
If the choice is made to remove the IUD because of concerns about the levonorgestrel, then further decisions must ensue regarding contraception. All hormonal contraception options contain progestins. Shared and informed decision making is important for the patient to be able to choose a contraceptive option that is safe, effective, and meets their personal considerations. Any adverse effects potentially related to a medical device should be reported to the US Food and Drug Administration via MedWatch.14
Powerful, complex relationships exist between health and physical attributes and between health and socioeconomic attributes that influence both individuals and populations. US minority populations have demonstrated significant disparities in healthcare outcomes. Black women are particularly susceptible. Overcoming these disparities is a goal on the national, local, and individual level. Healthcare providers can make a difference and overcome bias through a thoughtful purposeful approach to their own practice. This includes humanizing the patient and identifying implicit and explicit bias while promoting and supporting patient engagement, understanding, and involvement.15
Amy S. D. Lee is Clinical Associate Professor and Angela Collins-Yoder is Clinical Professor at Capstone College of Nursing in Tuscaloosa, Alabama. Dr. Collins-Yoder is also a critical care clinical specialist for the neuroscience service line at Ascension Sacred Heart in Pensacola, Florida. Verdlynn Dalge Sylvains is a per diem critical care nurse in South Florida. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
References
- Friedman DI, Liu GT, Digre KB. Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology. 2013;81(13):1159-1165.
- Rehder D. Idiopathic intracranial hypertension: review of clinical syndrome, imaging findings, and treatment. Curr Probl Diagn Radiol. 2020;49(3):205-214.
- Radojicic A, Vukovic-Cvetkovic V, Pekmezovic T, et al. Predictive role of presenting symptoms and clinical findings in idiopathic intracranial hypertension. J Neurol Sci. 2019;399:89-93.
- Xu W, Prime Z,Papchenko T, Danesh-Meyer HV. Long term outcomes of idiopathic intracranial hypertension: observational study and literature review. Clin Neurol Neurosurg. 2021;205:106463.
- Tann MG, Worley B, Kim WB, et al. Drug-induced intracranial hypertension: a systematic review and critical assessment of drug-induced causes. Am J Clin Dermatol. 2020;21(2):163-172.
- Crum OM, Kilgore KP, Sharma R, et al. Etiology of papilledema in patients in the eye clinic setting. JAMA Netw Open. 2020;3(6): e206625.
- Togha M, Martami F, Rahmanzadeh R, et al. The role of opening CSF pressure in response to treatment for idiopathic intracranial hypertension (IIH). J Clinl Neurosci. 2020; 76:171-176.
- Kilgore KP, Lee MS, Leavitt JA, et al. A population-based, case-control evaluation of the association between hormonal contraceptives and idiopathic intracranial hypertension. Am J Ophthalmol. 2019; 197:74-79.
- Markey KA, Uldall M, Botfield H, et al. Idiopathic intracranial hypertension, hormones, and 11-hydroxysteroid dehydrogenases. J Pain Res. 2016; 9:223-232.
- Beatty MN, Blumenthal PD. The levonorgestrel-releasing intrauterine system: safety, efficacy, and patient acceptability. Ther Clin Risk Manag. 2009;5(3):561-574.
- Etminan M, Luo H, Gustafson P. Risk of intracranial hypertension with intrauterine levonorgestrel. Ther Adv Drug Saf. 2015;6(3):110-113.
- Jackson I. MDL judge dismisses all pseudotumor cerebri lawsuits over Mirena IUD birth control. June 12, 2019.
- Valenzuela RM, Rai R, Kirk BH, et al. An estimation of the risk of pseudotumor cerebri among users of the levonorgestrel intrauterine device. Neuroophthalmology. 2017;41(4):192-197.
- US Food and Drug Administration. Medical Device Reporting (MDR): How to Report Medical Device Problems. Updated October 2, 2020.
- White AA, Stubblefield-Tave B. Some advice for physicians and other clinicians treating minorities, women, and other patients at risk of receiving health care disparities. J Racial Ethn Health Disparities. 2017;4(3):472-479.