
Faculty: Heather C. Quaile, DNP, WHNP-BC, SANE, is CEO, Founder, and Clinical Director of the Sexual Health Optimization and Wellness (SHOW) Center in Kennesaw, Georgia, a women’s health integrated practice and telehealth platform that focuses on personalized approaches to care for women facing the challenges of sexual dysfunction, sexual trauma, and pelvic conditions using trauma-informed care. She is also the Clinical Director for Wellspring Living, Receiving Hope Center for Human Trafficking, in Georgia.
Intended audience: This continuing education (CE) activity has been designed to meet the educational needs of nurse practitioners and other healthcare providers who provide primary care for women.
CE approval period: Now through August 31, 2022
Estimated time to complete this activity: 1 hour
CE approval hours: 1.0 contact hour of CE credit
Goal statement: Nurse practitioners and other healthcare providers who provide primary care for women will increase their knowledge about the long-term effects of trauma and providing trauma-informed care.
Needs assessment: In the United States, 70% of adults have experienced some type of traumatic event at least once in their lives. Trauma survivors may experience serious long-term effects on their mental, physical, social, and emotional well-being. Providing care that promotes healing and recovery for trauma survivors requires a particular set of attitudes, knowledge, and skills encompassed in trauma-informed care. Nurse practitioners and other healthcare providers who provide primary care for women need to be knowledgeable about and able to implement trauma-informed care.
Educational objectives: At the conclusion of this educational activity, participants should be able to:
1. Describe the long-term effects experiencing trauma can have on mental, physical, social, and emotional well-being.
2. Identify cues that trauma may be part of the patient’s life experience.
3. Discuss the four R’s and six principles for implementing trauma-
informed care in the primary care setting.
Accreditation statement: This activity has been evaluated and approved by the Continuing Education Approval Program of the National Association of Nurse Practitioners in Women’s Health (NPWH) and has been approved for 1 contact hour of CE credit.
Faculty disclosures: NPWH policy requires all faculty to disclose any affiliation or relationship with a commercial interest that may cause potential, real, or apparent conflict of interest with the content of a CE program. NPWH does not imply that the affiliation or relationship will affect the content of the CE program. Disclosures provide participants with information that may be important to their evaluation of an activity. In addition, faculty will identify any unlabeled/unapproved uses of drugs or devices discussed in their presentations.
Heather C. Quaile, DNP, WHNP-BC, SANE, has no actual or potential conflicts of interest in relation to the contents of this article.
Disclosure of unlabeled/unapproved use: NPWH policy requires authors to disclose to participants when they are presenting information about unlabeled use of a commercial product or device, or an investigational use of a drug or device not yet approved for any use.
Disclaimer: Participating faculty members determine the editorial content of the CE activity; this content does not necessarily represent the views of NPWH. This content has undergone a blinded peer review process for validation of clinical content. Although every effort has been made to ensure that the information is accurate, clinicians are responsible for evaluating this information in relation to generally accepted standards in their own communities and integrating the information in this activity with that of established recommendations of other authorities, national guidelines, FDA-approved package inserts, and individual patient characteristics.
Successful completion of the activity: Successful completion of this activity, J-20-04, requires participants to:
1. “Sign in” at the top right-hand corner of the page https://www.npwh.org/courses/home/details/1542 if you have an NPWH account. You must be signed in to receive credit for this course. If you do not remember your username or password, please follow the “Forgot Password” link and instructions on the sign-in page. If you do not have an account, please click on “Create an Account.”*
2. Read the educational objectives, disclosures, and disclaimers on the next page and then click on the “Continue” button.
3. Study the materials in the learning activity during the approval period (now through August 31, 2022).
4. Complete the post-test and evaluation. You must earn a score of 70% or higher on the post-test to receive CE credit.
5. Print out the CE certificate after you have successfully passed the post-test and completed the evaluation.
*If you are an NPWH member, were once a member, or have taken CE activities with NPWH in the past, you have a username and password in our system. Please do not create a new account. Creation of multiple accounts could result in loss of CE credits as well as other NPWH services. If you do not remember your username or password, either click on the “Forgot Username” or “Forgot Password” link or call the NPWH office at (202) 543-9693, ext. 1.
Commercial support: No commercial support was supplied for this activity.
Before reading the article, click here to take the pretest.
In the United States, 70% of adults have experienced some type of traumatic event at least once in their lives. Over 90% of patients who are seen in public behavioral health clinics have experienced trauma. In this article, the author discusses what is trauma-informed care (TIC), the road and four R’s to it, TIC for healthcare providers using six key principles, and its relevance to clinical practice.
Key words: trauma-informed care, realization, recognition, responding, resisting, re-traumatization
Valuing the human experience and abiding by the golden rule is often what guides providers to care and advocate for their patients through the health–illness continuum. The enactment of these values is vital
to creating a trusting patient–provider relationship and providing trauma-informed care (TIC). Lack of awareness concerning the implications of trauma can result in harmful and widespread effects for the patient, the healthcare system, and society. Healthcare providers (HCPs) working in the primary care setting have an opportunity and obligation to be knowledgeable about and have the skills to provide TIC.
What is trauma?
A universal definition of trauma does not clearly exist, but overall trauma refers to any experience that causes an intense psychological or physical stress reaction.1 It may occur as a result of violence, abuse, neglect, loss, disaster, war, and other emotionally harmful experiences. Trauma may occur as the result of a single event, a series of events, or a set of circumstances. The extent to which an event is traumatic depends on how an individual interprets, applies meaning to, and is disrupted by that event.2 Trauma can result in a wide range of responses including intense feelings of fear, loss of trust in others, decreased sense of personal safety, guilt, and shame. Trauma does not discriminate, and it bridges itself across age groups, gender, socioeconomic status, race, ethnicity, geography, and sexual orientation.2 In the United States, 70% of adults have experienced some type of traumatic event at least once in their lives. Over 90% of patients who are seen in public behavioral health clinics have experienced trauma.2
Experiencing trauma can have serious long-term effects on mental, physical, social, emotional, and spiritual well-being. High-risk behaviors such as excessive alcohol use, illicit drug use, unsafe sex, and disordered eating are often used in an attempt to cope with the intense negative feelings associated with trauma.3 Individuals who have experienced trauma, in part as a result of high-risk behaviors, are at increased risk for substance use disorders, sexually transmitted infections, and chronic health conditions such as lung, heart, and liver disease. Their traumatic experiences can also place them at risk for depression, anxiety, sleep disorders, and suicidal ideation/attempts.2–5
When a child or adolescent is exposed to traumatizing events, it can be particularly significant, as documented by the landmark adverse childhood experiences (ACE) study that was conducted by Kaiser Permanente and the Centers for Disease Control and Prevention.1,2,4,5 In this study, ACEs included, but were not limited to, experiencing or observing physical, sexual, and emotional abuse; childhood physical or emotional neglect; having a family member with a mental health or substance use disorder; experiencing or witnessing violence in the home or community, parental separation or divorce, or having an incarcerated household member. The study has demonstrated an association of ACEs with health and social problems across the lifespan. For example, in adulthood, the history of ACE can result in complex clinical problems with several coexisting mental and somatic disorders such as posttraumatic stress disorder, depression, borderline personality disorder, compromised immune system, obesity, and diabetes. It has been suggested that during certain vulnerable developmental phases, the risk for subsequent ACE-related disorders is increased. As well, some evidence now implicates sensitive periods and specificity of ACE subtypes in the development of neurobiologic alterations such as volumetric and functional changes in the amygdala and hippocampus.6 All developmental domains may be affected by ACEs and trauma (ie, attachment, physical, affect regulation, behavioral control, cognitive, self-image).1,3,4,7
- Reduce the impact of trauma on individuals, families, and communities
- Develop/implement trauma-informed approach across systems and workplaces; for users and providers of services
- Make trauma-informed screening, early intervention, and treatment common practice
- Promote recovery, well-being, and resilience
Adverse childhood experiences are a critical public health issue. In the United States, 45% of children have experienced at least one ACE and 1 in 10 children have experienced three or more ACEs, placing them in a category of high risk.8 Children of different races and ethnicities do not experience ACEs equally. Nationally, 61% of black non-Hispanic children and 51% of Hispanic children have experienced at least one ACE, compared with 40% of white non-Hispanic children and only 23% of Asian non-Hispanic children.
The concept of historical trauma is based on the premise that specific cultural, ethnic, or racial groups historically subjected to long-term systemic abuse and injustices (ie, segregation/displacement, physical/psychological violence, economic destruction, cultural dispossession) may experience negative effects that span several generations. This multigenerational trauma has significance in terms of potential ongoing health disparities for families, communities, and cultures. Although more research is needed, there is evidence of a link between experiencing historical trauma and the prevalence of detrimental physical, psychological, and social responses (ie, heart disease, cancer, depression, anxiety, substance misuse and addiction, suicide).1,9
The road to trauma-informed care
Many aspects of how trauma survivors choose to engage in health behaviors and healthcare are influenced by their experiences. They may neglect their health, harm themselves, avoid healthcare, not trust HCPs, and not adhere to recommended therapies. Providing care that promotes healing and recovery for these patients requires a particular set of attitudes, knowledge, and skills encompassed in TIC. TIC is a strengths-based service delivery approach.1 This approach to care acknowledges the need to understand a patient’s life experiences to deliver effective care. It has the potential to improve patient engagement, treatment adherence, health outcomes, and provider and staff wellness.10 This integrated, comprehensive approach includes providing a safe environment for all patients and staff, identifying patients who are survivors of trauma and implementing practices to avoid re-traumatization, assessing patients’ needs and providing them with resources and referrals that will facilitate recovery, and monitoring both processes and outcomes in the clinical setting for ongoing quality improvement.
TIC is built on the assumption that an individual patient is more likely than not to have a history of trauma. This means that it is deemed important to provide a supportive and therapeutic environment for every patient that promotes safety, inclusion, collaboration, empowerment, and respect. Research has consistently shown that when the right supports are in place, the majority of people who grow up amid extremely challenging circumstances not only survive but end up thriving. Similarly, specific factors have been demonstrated to be protective against traumatic experiences. That ability to “bounce back” has been termed resilience.11 Individuals who experience trauma are more likely to develop resilience when their environments are responsive to their specific needs.
As a component of implementing TIC, the HCP should be observant for cues that trauma may be part of the patient’s life experience. Such cues may include body language, verbal indictors, other specific behaviors, and physical findings. A survivor of trauma may express through body language or verbal comments that they are fearful, anxious, and/or lack trust. Their affect when engaging with the HCP may be flat or submissive. They may avoid direct eye contact.8 If the patient is currently in an abusive situation and the perpetrator is present during the healthcare visit, that person may try to control the flow of information, insist on being present during all aspects of the visit, and exert control over the patient’s decision-making process.12
For survivors of trauma who have experienced physical violence, the HCP may find acute injuries or injuries in various stages of healing. The injuries may not match with the patient’s history if they are fearful or reluctant to disclose the trauma they have experienced. Self-injuries may also be observed.12 Universal screening for trauma, whether signs and symptoms are present or not, affirms to patients that the HCP believes the experience of trauma is important to acknowledge to provide the best healthcare. This approach shifts the focus from “What’s wrong with you?” to “What happened to you?” and provides the opportunity for disclosure in a safe and confidential environment. When trauma is identified, HCPs and other staff can actively resist re-traumatization that may cause the patient to experience emotional and biologic stress.1,3,13
The Brief Trauma Questionnaire (BTQ)
Stressful Life Events Screening Questionnaire (SLESQ)
The Traumatic Life Events Questionnaire (TLEQ)
(The scale is in the article’s appendix.)
The HCP can seek to further understand how trauma has affected the patient and offer appropriate resources and referrals, such as cognitive behavioral therapy, meditation, mindfulness, breathing exercises, and eye movement desensitization and reprocessing as pathways to healing and recovery.14
 The four R’s
The four R’s
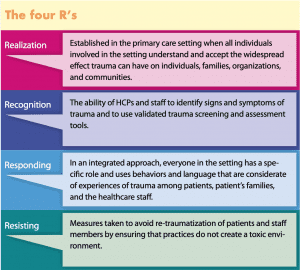
The four R’s of the trauma-informed approach to care from the Substance Abuse and Mental Health Services Administration (SAMHSA) can be used to effectively implement TIC in the primary care setting. These four key assumptions are: realization, recognition, responding, and resisting.1,2
Realization is established in the primary care setting when all individuals involved in the setting understand and accept the widespread effect trauma can have on individuals, families, organizations, and communities. When staff realize that particular patient behaviors may represent coping strategies designed to survive adversity and overwhelming circumstances that may have happened in the past or may be going on in the present, they are better equipped to provide TIC. HCPs can extend the support they provide when they are aware of the influence of trauma on family members, first responders, service providers, and others who may experience secondary stress, also known as vicarious trauma (trauma-related reactions to exposure to another person’s traumatic experience).15
Recognition requires the ability of HCPs and staff to identify signs and symptoms of trauma and to use validated trauma screening and assessment tools (Table). There is an understanding that trauma reactions and symptoms of trauma vary by gender, age, type of trauma, or setting, as well as that these symptoms may be seen in families, staff, and others involved with the patient.
Responding goes beyond realizing and recognizing to integrate a trauma-informed approach throughout the healthcare setting. In an integrated approach, everyone in the setting has a specific role and uses behaviors and language that are considerate of experiences of trauma among patients, patient’s families, and the healthcare staff. Policies, procedures, and practices used in the setting reflect a commitment to creating a culture of resilience, recovery, and healing from trauma. Staff are trained and provided with guidance on secondary traumatic stress, and there is an apparent commitment to a physically and psychologically safe environment.
Resisting entails measures taken to avoid re-traumatization of patients and staff members by ensuring that practices do not create a toxic environment. These measures include actively shaping the setting to avoid triggers (ie, sounds, sights, smells, objects, places, people reminding an individual of the original trauma, invasive procedures, removal of clothing, physical touch, personal questions that may be distressing or embarrassing, vulnerable physical position, and loss or lack of privacy). The goal is to protect the individual from further trauma and avoid exacerbating negative impacts that can interfere with the healing process.15
Six key principles
Trauma-informed care as a strengths-based approach is founded on six key principles more than on a set of prescribed practices or procedures.1,2 The six key principles are safety; trustworthiness and transparency; peer support; collaboration and mutuality; empowerment, voice, and choice; and cultural, historical, and gender issues.1
Safety involves ensuring that all people in the healthcare setting feel safe. This includes the safety of the physical setting and the nature of interpersonal interactions. Trust-
worthiness is fostered by transparency in decision making and processes in the healthcare setting with the goal of building and maintaining trust with patients and among staff. Peer support from other trauma survivors is important in establishing safety and hope that promotes recovery and healing. Collaboration and mutuality places importance on partnering and leveling of power experiences between patients and staff and among all categories of staff including clerical, professional, and administrative. There is a recognition that everyone in the healthcare setting has a role to play in a trauma-
informed approach to providing care. Empowerment, voice, and choice is about acknowledging and building on the strengths of patients and staff within the healthcare setting. Patients are supported in shared decision making, choice, and goal setting to determine the plan of action they need to heal. The development of self-advocacy skills is facilitated. The staff working in the healthcare setting are empowered to do their work as well as possible through adequate organizational support. Cultural, historical, and gender issues are addressed in the healthcare setting to actively move past biases and stereotypes (ie, gender, region, sexual orientation, race, age, religion). The potential effects of historical trauma are recognized. Processes and policies that are responsive to diverse needs are incorporated.16
Implications for clinical practice: challenges and strategies for improvement
Implementing a trauma-informed approach to care within a primary care setting is not without its challenges. As previously described, trauma survivors may lack trust, not feel safe, or be ashamed to disclose the experiences they have had. Cultural differences can exacerbate these feelings and can lead to misperceptions in interpretation of signs and symptoms. Comorbidities of depression and substance use disorders may cause poor motivation. Any of these factors can result in not seeking needed care and not adhering to recommended treatment and follow-up.17
Other challenges to implementing a trauma-informed approach to care that can occur in the primary care setting include the lack of resources to provide training for providers and staff. In a busy setting where patients may present with comorbidities, HCPs may be frustrated with time constraints that do not always allow for trust building and the individualized care needed to promote recovery. Attention to staff affected by providing care for patients who are trauma survivors may not occur. In some areas, there may also be a lack of adequate behavioral health providers with expertise in TIC to allow for needed referrals for treatment.17–19
Inconsistency in treatment across multidisciplinary teams, disruption in the continuity of care, and lack of proper assessment and diagnosis can impact safety and cause re-
traumatization.
In a primary care setting, these challenges in part can be addressed by implementing the four R’s and the six key principles for TIC. These concepts and principles are not setting specific and do not require following one set of prescribed practices. Provider and staff training resources are available that can be tailored to a primary care setting of any size and in any location.
Some of the challenges go beyond the individual primary care setting and must be addressed within a larger framework that includes healthcare systems, communities, and educational institutions. In fact, the healthcare systems within which the primary care setting operates should adopt the four R’s (key assumptions) and the six key principles for TIC. This level of commitment is needed to support provider and staff training and ensure hiring of healthcare providers trained in trauma-focused therapy so that trauma survivors have opportunities for individual and group therapy and consistent care and follow-up. The procurement of resources and development of protocols to assist providers and staff experiencing their own trauma as the result of caring for trauma survivors is important. Healthcare systems can lead in facilitating discussions among all employees about trauma in a safe environment that builds trust and fosters empowerment in caring for trauma survivors.20–22
Although TIC training of existing providers and staff is important, so is preparing future providers through intentional incorporation of curriculum content in schools of nursing and medicine. Curriculum content should include attitudes, beliefs, knowledge, and skill components needed to implement the four R’s and the six key principles. Research on trauma, its effect on individuals’ health and well-being, and effective therapies for recovery and treatments to manage symptoms should be encouraged.20,21
Conclusion
Trauma-informed care cannot exist without organizational support
and a climate that is itself trauma-informed and adheres to and promotes the six principles of TIC with respect to organizational climate and culture and the treatment of patients, providers, and staff. Using a system-wide approach is the first step in creating change and paving the way for future TIC treatment and practices in the primary care setting. It is essential to emphasize the need and provide opportunities for self-care and empathy as well as other avenues of support for all clinicians and primary care staff. It is of utmost importance to reinforce the healthcare team to utilize their skills to build on strength, resiliency, and hope.
References
- Substance Abuse and Mental Health Services Administration. TIP 57: Trauma-Informed Care in Behavioral Health Services. Rockville, MD: SAMHSA; 2014.
- Substance Abuse and Mental Health Services Administration. SAMHSA’s Concept of Trauma and Guidance for a Trauma-Informed Approach. SAMHSA’s Trauma and Justice Strategic Initiative. Rockville, MD: SAMHSA; 2014.
- Leitch L. Action steps using ACEs and trauma-informed care: a resilience model. Health Justice. 2017;5(1):5.
- Felitti VJ, Anda RF, Nordenberg D, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: the adverse childhood experiences (ACE) study. Am J Prev Med. 1998;14(4):245-258.
- Public Health Management Corporation; Merritt MB, Cronholm P, Davis M, et al. Findings from the Philadelphia Urban ACE Survey. Institute for Safe Families. September 18, 2013.
- Herzog JI, Schmahl C. Adverse childhood experiences and the consequences on neurobiological, psychosocial, and somatic conditions across the lifespan. Front Psychiatry. 2018;9;420.
- Center for Early Childhood Mental Health Consultation. Tutorial 7: Recognizing and addressing trauma in infants, young children and their families. Georgetown University. https://www.ecmhc.org/tutorials/trauma/mod3_1.html.
- Sacks V, Murphey D. The prevalence of adverse childhood experiences, nationally, by state, and by race or ethnicity. Bethesda, MD: Child Trends; February 20, 2018. https://www.childtrends.org/publications/prevalence-adverse-childhood-experiences-nationally-state-race-ethnicity.
- Sotero MM. A conceptual model of historical trauma: implications for public health practice and research. J Health Disparities Res Pract. 2006;1(1):93-108.
- US Department of Health and Human Services. Agency for Healthcare Research and Quality. Trauma-informed care. April 2016. https://www.ahrq.gov/professionals/prevention-chronic-care/healthier-pregnancy/preventive/trauma.html.
- Walsh TB, McCourt SN, Rostad WL, et al. Promoting protective factors and strengthening resilience. In: Daro D, Donnelly AC, Huang LA, Powell BJ, eds. Advances in Child Abuse Prevention Knowledge: The Perspective of New Leadership. Switzerland; Springer; 2015:203-224.
- Knight C. Trauma informed practice and care: implications for field instruction. Clin Social Work J. 2019;47:79-89.
- Key KH. Foundations of Trauma-Informed Care: An Introductory Primer. Baltimore, MD:
LeadingAge Maryland; 2018. - Kinoglu S, Nelson-Dusek S, Skrypek M. Creating a Trauma-Informed Organization: Literature Review for Volunteers of America. St. Paul, MN: Wilder Research; January 2017.
- Bartlett JD, Steber K. How to implement trauma-informed care to build resilience to childhood trauma. Bethesda, MD: Child Trends; 2019. https://www.childtrends.org/publications/how-to-implement-trauma-informed-care-to-build-resilience-to-childhood-trauma.
- Purkey E, Patel R, Phillips SP. Trauma-informed care: better care for everyone. Can Fam Physician. 2018;64(3):170-172.
- Baird K, Kracen AC. Vicarious traumatization and secondary traumatic stress: a research synthesis. Counselling Psychol Quar. 2006;19(2):181-188.
- Elliott DE, Bjelajac P, Fallot RD, et al. Trauma-informed or trauma-denied: principles and implementation of trauma-informed services for women. J Community Psychol. 2005;33(4):461-477.
- Wilson A, Hutchinson M, Hurley J. Literature review of trauma-informed care: implications for mental health nurses working in acute inpatient settings in Australia. Int J Ment Health Nurs. 2017;26(4):326-343.
- Ades V, Wu SX, Rabinowitz E, et al. An integrated, trauma-informed care model for female survivors of sexual violence: the Engage, Motivate, Protect, Organize, Self-Worth, Educate, Respect (EMPOWER) Clinic. Obstet Gynecol. 2019;133(4):803-809.
- Stokes Y, Jacob JD, Gifford W, et al. Exploring nurses’ knowledge and experiences related to trauma-informed care. Glob Qual Nurs Res. 2017;4:2333393617734510.
- Spoont MR, Williams JW Jr, Kehle-Forbes S, et al. Does this patient have posttraumatic stress disorder?: rational clinical examination systematic review. JAMA. 2015;314(5):501-510.
Web resources
npwh.org/courses/home/details/1542
ptsd.va.gov/professional/assessment/documents/BTQ.pdf
georgetown.app.box.com/s/nzprmm2bn5pwzdw1l62w
ncbi.nlm.nih.gov/pmc/articles/PMC3115408/
ptsd.va.gov/professional/assessment/documents/PCL5_criterionA_form.PDF