
Nurse practitioners (NPs) who provide healthcare for individuals considering a pregnancy have the opportunity to discuss and offer genetic carrier screening as part of prepregnancy care, including it into reproductive life planning at routine wellness visits or during prepregnancy visits. Prepregnancy carrier screening provides individuals and couples with information about reproductive risks to assist them in making informed decisions about family planning, reproductive options, and care during pregnancy and birth. This article provides NPs with information they can use to incorporate routine prepregnancy genetic carrier screening into clinical practice using available evidence-based screening and education/counseling resources.
Key words: expanded carrier screening, mutations, chromosomes, autosomal recessive conditions, X-linked conditions, electronic medical record, prenatal, variants
The National Association of Nurse Practitioners in Women’s Health supports the role of nurse practitioners (NPs) in providing prepregnancy carrier screening for reproductive-age individuals and couples.1 The American College of Obstetricians and Gynecologists (ACOG) committee opinion on carrier screening for genetic conditions emphasizes the importance of establishing a routine and consistent approach in ob/gyn practice in offering carrier screening, ideally prepregnancy.2 Components of this approach include using family history risk-assessment tools; explaining the benefits, risks, implications of carrier screening, tests available, and costs; providing resources for individuals and couples who want to seek additional information; and having in place a means for individuals and couples to obtain counseling concerning the screening results.
Nurse practitioners who choose to offer prepregnancy genetic carrier screening in their clinical practice will want to review what components are already in place and what needs to be added. Basic knowledge about carrier screening, prescreening education for patients, and recommended follow-up is essential. An assessment of how the components can fit into clinic flow will facilitate a smooth process.
Genetic carrier screening
Genetic carrier screening is done to determine if a person who has no signs or symptoms of a genetic disease has a pathogenic variant/mutation within a gene that is associated with a particular genetic disorder.1 This testing primarily looks for autosomal recessive conditions (eg, cystic fibrosis, sickle cell anemia, spinal muscular atrophy, Tay-Sachs disease), which means that to have the condition, both copies of the gene need to be nonfunctioning. If a person is a carrier, they have only one affected gene for the disorder and have no overt medical or health issues. If both persons in a reproductive couple are carriers of the same autosomal recessive gene mutation, there is a 25% chance they will have a child with both copies of the mutated gene and will have the genetic condition (Figure 1).3 Other than autosomal recessive conditions, however, expanded carrier screening (ECS) can typically include significant X-linked recessive disorders (eg, Fragile X, Duchenne muscular dystrophy). These are sex-linked disorders located on the X chromosome only and commonly affect the male. If a male inherits a nonfunctioning gene on his X chromosome, he will likely have that condition because he does not have a second functioning copy of that gene. A female usually has a working copy of that gene on her other X chromosome, so she may have mild or no symptoms at all as a carrier (Figure 2).3
Figure 1. Autosomal recessive inheritance pattern3
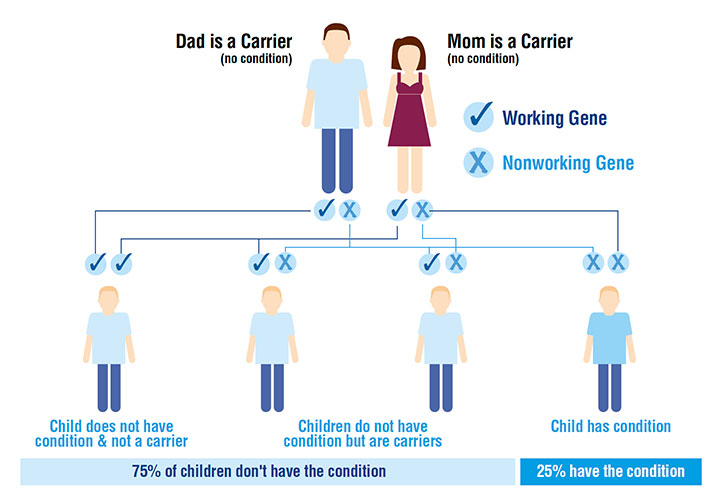
Figure 2 . X-linked recessive inheritance-pattern3
Carrier screening can be done before or during pregnancy via a simple blood test or buccal saliva swab. Serious recessive and X-linked conditions affect approximately 1 in 300 pregnancies.4 These conditions can potentially reduce lifespan, may cause intellectual or physical disabilities that require early and lifelong treatment, or may have no treatment available. When screening is done prior to a pregnancy, the results provide the individual or couple with information about reproductive risks that can assist them in decision making on family planning and reproductive options. Options that may be considered when carrier screening for both individuals is positive for disease include pursuing in vitro fertilization with preimplantation genetic diagnosis, donor egg or sperm, adoption, deciding not to have a child, opting for prenatal diagnostic testing during a pregnancy, obtaining referrals to specialists for potentially high-risk prenatal care and birth, and planning for medical and social services they may need if they have a child with the condition.2
Family history risk assessment
Obtaining a family history of genetic conditions for the patient and reproductive partner is an important part of prepregnancy care. A screening tool for inherited genetic carrier risk also can be used. The use of the one key question, “Do you want to become pregnant in the next year,” can be a prompt for initiating a family history risk assessment.
Electronic medical records (EMRs) have obstetrics/prenatal history intake elements that may be helpful in identifying at-risk individuals and couples. The March of Dimes family history form is also a useful tool: marchofdimes.org/family-health-history-form.pdf.5 Family history risk assessment tools can be built and customized for any patient population or practice. A practice may use an established form or develop its own form for review at a wellness visit if the patient indicates she is considering a pregnancy in the next year. Placing this form on a clinic website to complete prior to appointment would create an efficient workflow and help identify risk factors prior to the visit. Creating a “hard stop” in the EMR, meaning the chart cannot be ready for provider until the family health assessment risk intake is completed, would reduce important information from being overlooked.
When possible, the family history should include any known genetic conditions or risks of children, siblings, parents, aunts, uncles, cousins, nieces and nephews, and grandparents of both the patient and reproductive partner.3 Individuals or couples with a positive family history of a genetic condition should be offered carrier screening for the specific condition and may benefit from genetic counseling for optimal screening strategies. If the individual chooses to have genetic carrier screening, it is important to include all ethnicity and positive condition-related information obtained from family history with as much detail as possible on the lab requisition.
The evolving challenge in assessing genetic risks via a family history has increased with many individuals having multiple ethnic genetic backgrounds, some of which they are unaware, such as an Ashkenazi Jewish ancestry, which increases the risk of being a carrier of several conditions. These conditions for which carrier screening is offered are more common in individuals of Ashkenazi Jewish descent than other ethnic groups because of specific mutations that occurred in “founders” of the population. Because Jewish individuals historically married within their own ethnic group, these mutations increased in frequency over generations.6 Other challenges include being adopted, family dynamics that impede communication about health conditions, and losing touch with extended family members when moving results in geographic distancing.3 The family history remains important in identifying risks, yet it does not tell the whole story because a gene can be passed down silently for generations. Most children born with a genetic disorder have no known family history.1 The limitations of the family history and potential to overlook ethnic risk factors for genetic conditions support the benefits of ECS rather than targeted ethnic-specific screening. Expanded carrier screening provides screening for several disorders on a chosen panel using a single sample without regard to race or ethnicity. Targeted carrier screening focuses on disorders based on race, ethnicity, or family history.7 The use of ECS, however, does not replace the need for family risk assessment or genetic counseling, nor does it replace mandated newborn screening.8
Benefits, risks, implications for prepregnancy genetic carrier screening
Prepregnancy carrier screening enables individuals and couples to learn about their reproductive risk and consider the most complete range of reproductive options versus waiting until pregnancy when choices become more limited. The NP should provide clear, objective, and nondirective counseling so individuals and couples can make informed decisions in the context of their own needs and values. Respect for patient autonomy and confidentiality is crucial. Individuals and couples should be informed of the protections and limitations of the Genetic Information Discrimination Act (GINA), which makes it illegal for most health insurers to require genetic testing results or use results to make decisions about coverage, rates, or preexisting conditions. GINA also makes it illegal for employers to discriminate against employees or applicants because of genetic information. However, GINA does not apply to life insurance, long-term-care insurance, or disability insurance.9 The option to not have prepregnancy screening should always be offered and honored and ideally documented in the chart. Generally, informed consent stating the purpose of testing, what is tested, and whether the patient accepts or declines would clarify what testing was offered and accepted. Individuals and couples may decide at any time prepregnancy or during pregnancy to have screening.
Despite advancement in the technologic use of ECS, there are still some challenges to its implementation into routine practice. Individuals or couples may be disinterested in ECS for an array of reasons. One primary reason is that the general population has a lack of understanding of genetic conditions in general and may not see themselves at risk of being a carrier, thereby not being fully aware of the benefits of screening. Although some may see ECS as valuable to prevent a future child’s suffering or to prepare emotionally or financially for a child with serious disease, some may not change any decisions regarding care if there is a positive test result. Some may be concerned about cost of testing or for further workup if one is a carrier. For many, advanced reproductive treatment may not be realistic financially. There is also lack of consensus among medical experts as to whom ECS is appropriate for, making it confusing for providers to fully understand what and how to offer screening to their patients.10 Finally, provider and clinic time needed to provide pre- and post-test counseling may also be seen as a burden in an already busy practice. Continuous education of both healthcare professionals and the community is critical to reduce misconceptions and confusion about testing.11
Implications of potential positive screening results and available resources for counseling should be discussed. If an individual is found to be a carrier for a specific condition, the reproductive partner also should be offered testing. Tandem reflex testing, when available, can reduce waiting time and anxiety. With reflex testing, the patient and partner’s samples are sent to the lab together, but the partner’s sample is only tested and charged for if the patient screens positive for a condition. This strategy can also streamline workflow and reduce follow-up calls and appointments. When both individuals of the reproductive couple are identified as carriers of a genetic condition, genetic counseling should be offered to receive detailed information about potential reproductive outcomes and options.1
Most carrier screening labs have genetic counselors available to the clinician for guidance on test results if needed. They also typically offer online or phone counseling for the patient to discuss their results and implications, which can reduce some of the time burden for office staff and clinician. When an individual is found to be a carrier for a genetic condition, his or her relatives are at risk of carrying the same mutation. The individual should be encouraged to inform relatives of the risk and availability of carrier screening.
Prepregnancy genetic carrier screening services and costs
Lab or diagnostic companies that offer genetic carrier screening vary in the technologies utilized, expertise in what variants are screened, as well as in what pre- and post-test patient genetic counseling and resources are offered. Most labs that offer genetic carrier screening provide a streamlined approach so information can be integrated into clinic order sets, patient encounter forms, flowsheets, and lab inboxes. Kits are usually provided with blood draw or saliva kit collection supplies, and specimens can be collected by staff during or after an appointment. Virtual testing kits are now available, with a kit sent to the patient’s home to be drawn at specified labs, including partner testing.
Clear and concise results and simplified resources for patients with any positive results should be provided by the lab. Many companies offer easy-to-read brochures, tutorials, videos, links, and text message portals to help patients understand what the testing is, how much it may cost, and its implications. Genetic carrier screening lab representatives can provide more detailed information on these variables and services.
Conditions included in carrier screening panels vary from a range of 2 to 170 plus. Expanded carrier screening utilizes next-generation sequencing to efficiently and effectively screen for multiple conditions. Professional organizations with a focus on genetics and/or reproductive health recognize ECS as an appropriate screening strategy.1,4 According to ACOG, ethnic-specific, panethnic, and ECS are acceptable strategies for prepregnancy and prenatal carrier screening.7 The American College of Medical Genetics and Genomics, ACOG, National Society of Genetic Counselors, Perinatal Quality Foundation, and Society of Maternal-Fetal Medicine issued a joint statement in 2015 on points to consider for ECS.8 With ECS, a custom panel can be created for a clinic to provide consistent screenings for patients.
With the advancement in technology in next-generation sequencing testing strategies, the cost of ECS is decreasing.3 Many companies provide online portals where patients can obtain an estimate of the cost of testing. ECS may be covered completely by insurance. Patients with health savings accounts or flexible spending accounts as part of employee health benefits may be able to use these funds toward payment for testing. Most genetic screening lab companies offer patients without insurance coverage reduced cash pay options and income-driven price reductions. When considering cost, it may be helpful to let the patient know they only need this testing once in their lifetime as results do not change.
Prepregnancy carrier screening implementation
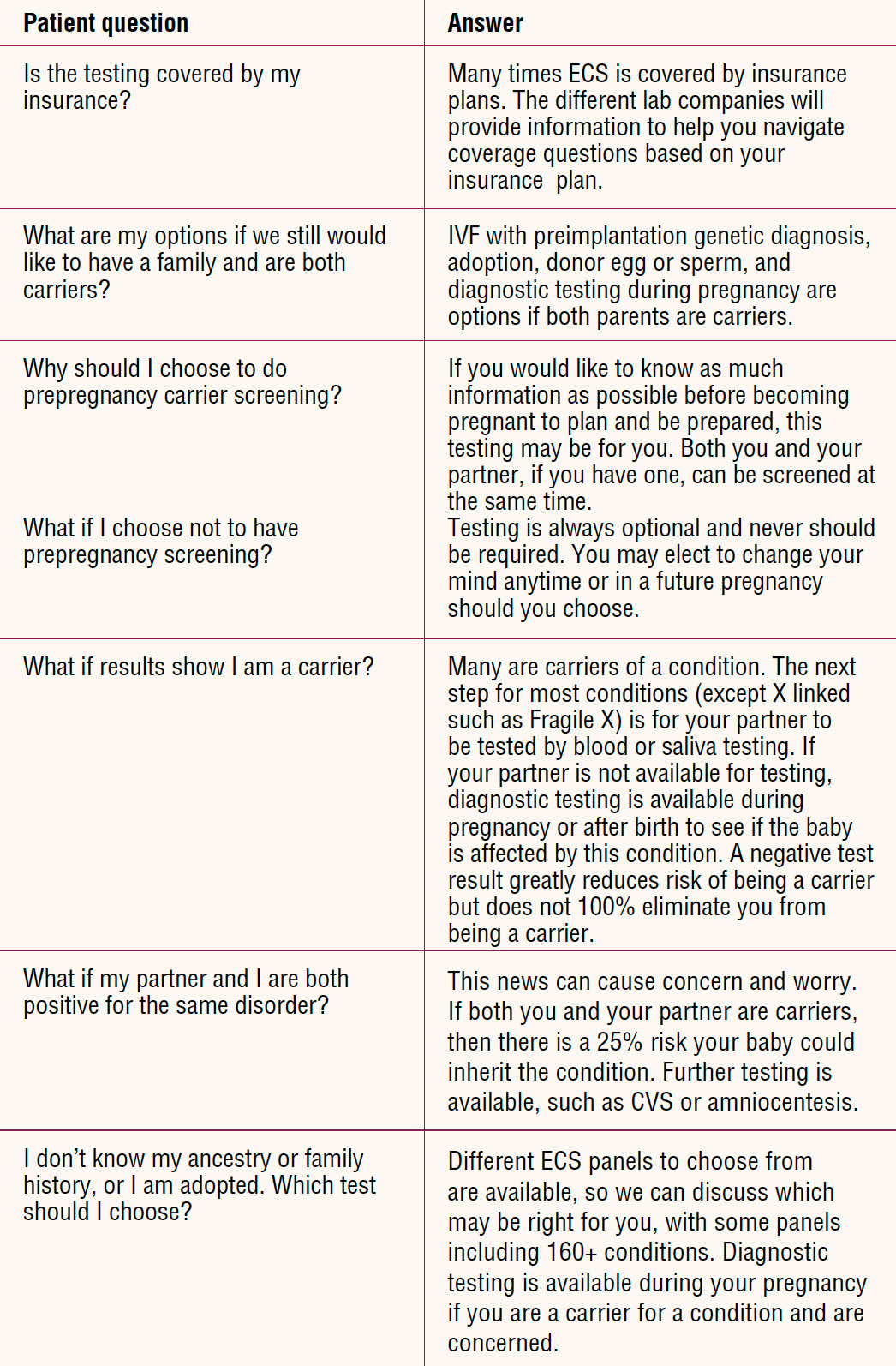
The NP who wants to implement prepregnancy carrier screening as a routine service for patients will want to do some preimplementation assessment and planning to ensure adequate preparation for success. As well, the NP may want to build in an evaluation component to monitor for any needed adaptations. Box 1 provides key points. Box 2 provides links to resources that may be useful for provider, staff, and patient education on basic genetic concepts and common genetic conditions. The Table provides examples of responses for frequently asked patient questions.
Box 1. Key points for implementation
- Assess what components are in place, what needs to be added (family history risk assessment, EMR obstetric/prenatal history, consent form) and where components will fit in clinic flow.
- Explore lab and diagnostic companies that provide genetic carrier screening to determine what panels are available, services they provide to patients before and after testing, education and consultation services available for providers and staff, and costs of tests.
- Educate self and staff with basic knowledge about genetic carrier screening, prescreening education for patients, and recommended follow-up.
- Develop a provider and staff routine for introducing and discussing the implications, risks, and benefits of prepregnancy genetic carrier screening.
- Obtain resources for individuals and couples who want to seek additional information.
- Establish referral resources for genetic counseling concerning screening and test results.
- Develop an evaluation tool to monitor for needed adaptations.
EMR, electronic medical record.
Box 2. Helpful resources
- MedLine Plus: Genetic conditions–signs and symptoms, genetic cause, and inheritance pattern. medlineplus.gov/genetics/condition
- Help Me Understand Genetics: Introduction to fundamental topics related to human genetics, including illustrations and basic explanations of genetics concepts.medlineplus.gov/genetics/understanding
- Disease infosearch: Up-to-date information on inherited disease, clinical trials, support groups, and publications; register to receive updates on that condition.diseaseinfosearch.org
- What is Newborn Screening?: Information on screenable conditions and state-by-state newborn screening. BabysFirstTest.org
- ACOG carrier screening frequently asked questions. acog.org/womens-health/faqs/carrier-screening
Table. Patient FAQs on carrier screening
Conclusion
Prepregnancy carrier screening provides individuals and couples with information about reproductive risks to assist them in making informed decisions about family planning, reproductive options, and care during pregnancy and birth. Performing testing prior to pregnancy offers several advantages instead of waiting until pregnancy, when options for management are more limited.
Do you discuss genetic carrier screening with patients as part of prepregnancy care?
The NP who is interested in making this a part of routine practice will want to consider all components needed when offering and explaining testing. Utilizing the principles, recommendations, and resources discussed throughout this article will enhance provider confidence in providing this service, facilitate smooth workflow, limit added staff and provider burden, and maintain visit time efficiency. Establishing a routine may take some initial workflow changes but is certainly a highly achievable and likely rewarding implementation into practice. Offering proactive prepregnancy carrier screening to patients improves reproductive healthcare. For the patient who is considering a pregnancy, this opportunity may lead to an increased sense of satisfaction and autonomy in reproductive decision making.
Andrea L. Stevens is an advanced nurse practitioner with New U Womens Clinic and Aesthetics in Kennewick, Washington, and volunteer clinical faculty at University of Washington in Spokane. The author states that she serves as a consultant/speaker for Myriad Genetics, but has no source of financial support or other actual or potential conflicts of interest in relation to the contents of this article.
Note: Since this article was published in the journal, we have learned that the new practice resource by the American College of Medical Genetics and Genomics (ACMG) now includes the recommendation that genetic carrier screening be offered to all those who are pregnant or considering a pregnancy. As the article’s author explains, ACMG previously recommended more limited carrier screening and for only certain ethnicities in its last statement in 2013. ACMG states that when carrier screening is limited to only certain ethnicities, a substantial number of pregnancies affected by serious genetic conditions fail to be identified. Screening without regard to ethnicity, as ACMG now recommends, avoids such inequity in care. For the full practice resource go to: www.acmg.net/PDFLibrary/41436_2021_1203_OnlinePDF.pdf.
References
NPWH. Position statement. Prepregnancy genetic carrier screening.
Women’s Healthcare. 2020;8(3):13-16.
American College of Obstetricians and Gynecologists. Committee opinion no. 691: carrier screening for genetic conditions. Obstet Gynecol. 2017;129(3):e41-e55. Updated 2020.
Genetic Support Foundation. Prenatal carrier screening, 2018. https://geneticsupportfoundation.org/practice-guideline-summaries/reproductive-practice-guideline-summaries/expanded-carrier-screening-practice-guideline-summaries.
Johansen Taber KA, Beauchamp KA, Lasarin GA, et al. Clinical utility of expanded carrier screening: results-guided actionability and outcomes. Genet Med. 2019;21(5):1041-1048.
March of Dimes. Family health history form. 2013. https://www.marchofdimes.org/family-health-history-form.pdf.
University of California, San Francisco. Ashkenazi Jewish carrier testing.https:// www.ucsfhealth.org/education/ashkenazi-jewish-carrier-testing.
American College of Obstetricians and Gynecologists. Committee opinion 690. Carrier screening in the age of genomic medicine. Obstet Gynecol. 2017;129(3):e35-e40.
Edwards JG, Feldman G, Goldberg J, et al. Expanded carrier screening in reproductive medicine-points to consider: a joint statement of the American College of Medical Genetics and Genomics, American College of Obstetricians and Gynecologists, National Society of Genetic Counselors, Perinatal Quality Foundation, and Society for Maternal–Fetal Medicine. Obstet Gynecol. 2015;125(3):653-652.
American College of Obstetricians and Gynecologists. Patient resources. FAQs. Carrier screening. December 2020. www.acog.org/womens- health/faqs/carrier-screening.
Kraft SA, Duenas D, Wilfond BS, Goddard KAB. The evolving landscape of expanded carrier screening: challenges and opportunities. Genet Med. 2019;21(4):790-797.
Ong R, Howting D, Rea A, et al. Measuring the impact of genetic knowledge on intentions and attitudes of the community towards expanded preconception carrier screening. J Med Genet. 2018;55(11):744-752.