
| Key words: pregnancy, perinatal period, perinatal anxiety, generalized anxiety disorder, perinatal anxiety screening scale |
Routine assessment for perinatal anxiety disorders, using established diagnostic criteria and standardized tools, can facilitate early diagnosis, guide management, and optimize outcomes for pregnant women and their offspring.
An anxiety disorder can disrupt a woman’s abilities to enjoy life and to self-care. When an anxiety disorder is present during the perinatal period—that is, during pregnancy and/or the first year postpartum—it can change how a woman experiences her pregnancy and how she interacts with and cares for her child.1 Limited data suggest a possible association between severe perinatal anxiety disorders and adverse pregnancy outcomes such as preterm birth, low birth weight, and postpartum depression.2,3 In addition, maternal anxiety disorders have been linked to developmental and mental health problems in offspring.2-4 Healthcare providers (HCPs) who see women during pregnancy and postpartum need to know the risk factors and signs and symptoms associated with perinatal anxiety disorders so that these disorders can be identified early and treated as needed. This article focuses primarily on assessment for and management of a common anxiety disorder—generalized anxiety disorder (GAD)—in this patient population.
Generalized anxiety disorder
Generalized anxiety disorder (GAD) is a mental disorder characterized by frequent and intense worry or anxiety about many aspects of one’s life (e.g., health, work, family), even if these aspects of life are going well.5 A person with GAD has difficulty controlling this anxiety, which can interfere with daily functioning.
Prevalence
Approximately 40 million adults in the United States, or 18% of the adult U.S. population, are diagnosed with an anxiety disorder each year, with 22.8% of these cases classified as severe.6 In addition to GAD, anxiety disorders include phobias, social anxiety disorder, post-traumatic stress disorder (PTSD), panic disorder, and obsessive-compulsive disorder. Many adults have more than one anxiety disorder.6 GAD, with a prevalence of 3.1% and an average age of onset of 31 years, is twice as common in women as in men,7 Anxiety disorders affect 4%-39% of women during pregnancy and up to 18% during the postpartum period.8
Risk factors
Perceived lack of partner and/or social support, a history of intimate partner violence or other abuse, a personal history of mental illness, having an unplanned or unwanted pregnancy, past or present pregnancy complications, and past pregnancy loss are risk factors for perinatal GAD.9 Women experiencing a high-risk pregnancy are also at greater risk for developing GAD.10,11 Other risk factors for perinatal GAD include failure to complete high school, unemployment, and nicotine use.12
Symptoms
Some degree of anxiety is common during pregnancy and postpartum, so HCPs should aim to differentiate between “normal” anxiety and GAD. Persons in the general population with GAD may report trembling, twitching, shakiness, muscle aches, sweating, nausea, diarrhea, and an exaggerated startle response.7 In the perinatal period, GAD may manifest as excessive and persistent nervousness, worry, or even panic about pregnancy and childbirth, the infant’s health, and parenting. Physical features—in addition to those listed for GAD in general—may include stomach pain, headaches, dizziness, palpitations, and shortness of breath.13 GAD can exacerbate sleep disturbances and fatigue in women during the perinatal period. Because anxiety and depressive disorders often co-exist, a pregnant or postpartum woman with GAD may exhibit manifestations of depression as well.14
Screening for perinatal GAD
Routine screening is essential for early recognition of GAD, which may otherwise go undetected and untreated in pregnant and postpartum women. Some of the most common clinical features of GAD may be attributed to normal physiologic changes of pregnancy or expected psychosocial adjustments to pregnancy and child care. A woman may be reluctant to report signs/symptoms of GAD for fear of being perceived as an excessive worrier or a hypochondriac.
The American College of Obstetricians and Gynecologists (ACOG) advises screening women at least once during the perinatal period for anxiety and depression using a standardized, validated tool.15 Although ACOG does not provide a recommendation for timing or frequency of this screening, the organization does advise HCPs to closely monitor women who have a history of, or risk factors for, anxiety or depressive disorders.
Two anxiety screening instruments used in both pregnant and postpartum women are the Generalized Anxiety Disorder-7 (GAD-7) and the Perinatal Anxiety Screening Scale (PASS). The GAD-7 is a 7-item self-report questionnaire created to identify essential areas of anxiety (worry, restlessness, irritability, and fear) and its severity in the previous 2 weeks.16,17 The reported internal consistency of the GAD-7 is excellent (Cronbach’s α, .92), and its test/retest reliability is good (intraclass correlation coefficient [ICC], .83). The PASS is useful throughout the perinatal period to assess for a range of anxiety symptoms.18,19 Principal component analyses suggested a 4-factor structure addressing symptoms of acute anxiety and adjustment; general worry and specific fears; perfectionism, control, and trauma; and social anxiety. The PASS is validated for use in hospital, mental health, and community samples and has excellent reliability (Cronbach’s α, .96) and test/retest reliability (ICC, .74). The Box lists various anxiety screens and provides links to them for easy access.
{kind=link}
Validated anxiety screening instruments with a postpartum focus include the Postpartum Worry Scale-R (PWS-R) and the Penn State Worry Questionnaire-10 (PSWQ-10). The PWS-R was developed to identify the degree of uncontrollable worry, a major symptom of GAD in postpartum women.20 This revised format of the original PWS includes items related to the mother’s perception of the infant’s well-being in terms of health and development and the mother’s relationship with her child.21,22 The PSWQ-10 measures worry, often described as the cardinal feature of GAD.23 Although the PSWQ-10 cannot distinguish GAD from major depressive disorder, it can track worry, which may affect both treatment and recovery. The Edinburgh Postnatal Depression Scale (EPDS) has an anxiety subscale (EPDS-3A) and can reliably differentiate between depression and anxiety.24
Making the diagnosis
Establishing rapport with patients facilitates a discussion of the clinical features of anxiety, screening test results, and treatment options.
HCPs need to determine the extent to which anxiety, worry, and/or the physical manifestations of anxiety are causing impairment in social, occupational, or other areas of functioning.
Once perinatal anxiety is identified and diagnosed, the next step is to determine whether an underlying condition might be causing the signs/symptoms or exacerbating their severity (e.g., substance misuse/abuse, a physical health condition), as well as whether co-existing psychiatric conditions such as depression, substance abuse, bipolar disorder, psychosis, schizophrenia, or PTSD might be complicating the picture. Referral to a mental health specialist is imperative when a pregnant woman has suicidal ideation, a co-existing psychiatric condition, or need for a complex medication regimen. HCPs providing perinatal care should have resources available for initiating a multidisciplinary team approach in treating perinatal anxiety.25,26
Management
If perinatal anxiety is determined to be the primary problem, cognitive behavioral therapy (CBT), the first-line treatment for anxiety in the general population, is a reasonable first approach.27 Although less studied in women with perinatal anxiety, CBT has been shown to be effective in treating postpartum depression.28,29 Additional nonpharmacologic options include mindfulness-based cognitive therapy, interpersonal therapy, psychodynamic therapy, acupuncture, and massage.30 When nondrug therapies are ineffective or only partially effective, medication may be indicated. In these cases, HCPs and patients should weigh the risks of not fully treating the anxiety disorder, the potential risks to a fetus exposed to the medications chosen, and the potential benefits of easing the anxiety disorder.
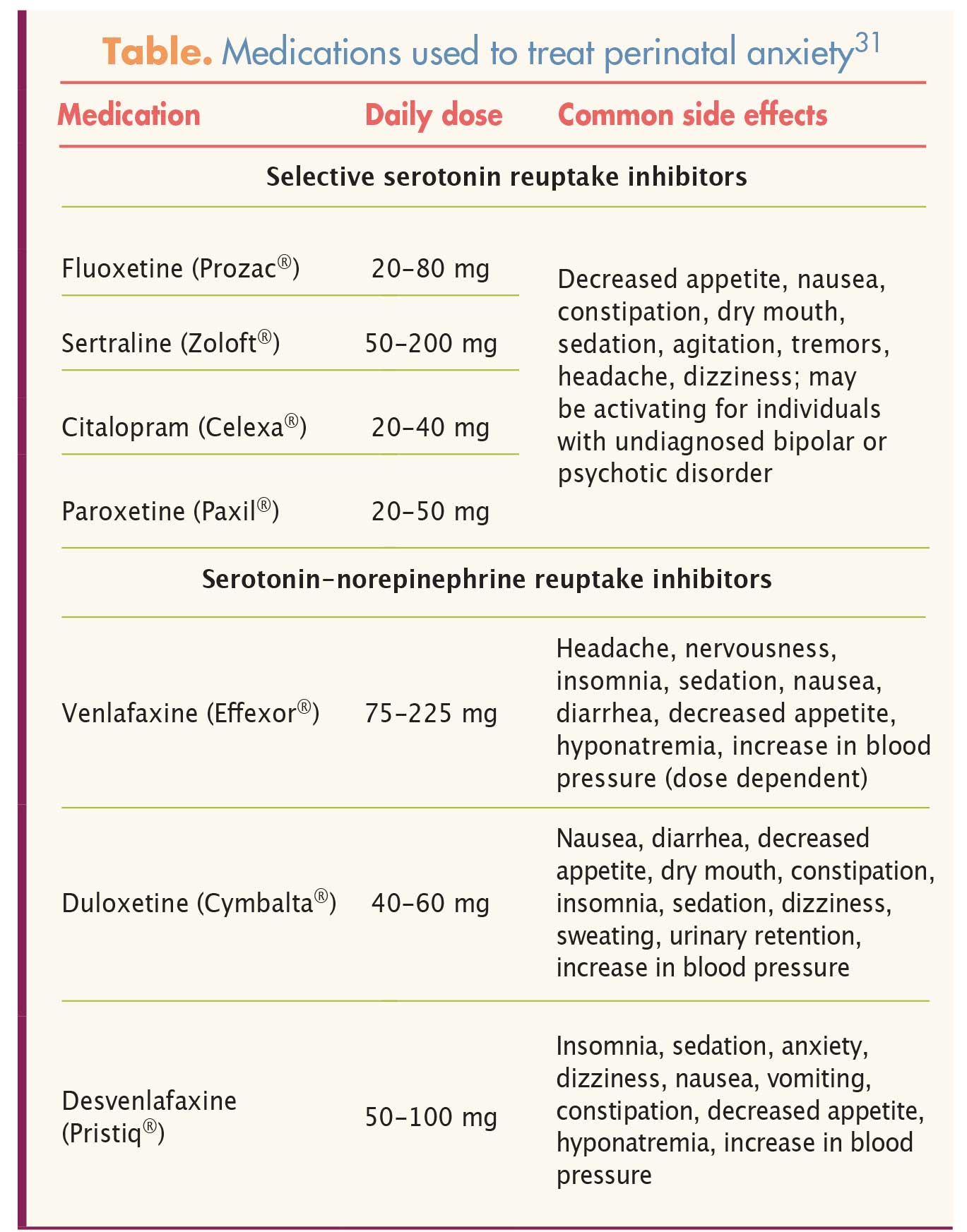
Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) are first-line drugs for the treatment of moderate or severe anxiety disorders.31 The Table lists commonly prescribed SSRIs and SNRIs, as well as their recommended daily doses and side effects.31 Taken together, data obtained over several years suggest that SSRIs and SNRIs are not teratogenic or associated with adverse pregnancy outcomes. Studies of the use of the SSRIs sertraline, fluoxetine, and citalopram during pregnancy provide the largest databases indicating no teratogenic effects.32,33 Although study results are conflicting, some reports have suggested a small increased risk for congenital heart defects associated with use of paroxetine during pregnancy.34,35 No teratogenic effects have been reported with use of SNRIs during pregnancy, although these agents may be associated with a small increased risk for pre-eclampsia.36
{kind=link}
The SSRIs fluoxetine and paroxetine and the SNRI venlafaxine, if taken around the time of birth, have been most closely associated with postnatal adaptation syndrome (PNAS).37 However, a recent study found that these agents did not cross the placenta to a greater extent than other antidepressants.37 Maternal use of SSRIs in late pregnancy may also be associated with a potentially increased risk of persistent pulmonary hypertension of the newborn.38 The absolute risk is small, and, according to a recent study, the increased risk appears more modest than that suggested in previous studies.38
Both SSRIs and SNRIs may be used for treatment of an anxiety disorder in a woman who is breastfeeding.34,39 Infants whose mothers are using the SSRIs fluvoxamine, paroxetine, or sertraline or the SNRI venlafaxine have been found to have low or undetectable serum drug levels, and no adverse effects have been reported.40
In the general population, use of benzodiazepines should be reserved for acute anxiety on a short-term basis because of the multiple associated risks: worsening of depressive symptoms, possible dependence, and possible overdose.32 Benzodiazepine use should be avoided in pregnancy because of these risks. Some data show a small increased risk for preterm birth, low birth weight, and floppy infant syndrome (hypotonia) in infants whose mothers used benzodiazepines during pregnancy. Data are inconclusive in terms of any teratogenic effect. If benzodiazepines are considered for women who are breastfeeding, those with a shorter half-life such as lorazepam and oxazepam are preferred because they are reported to result in low levels in breast milk and because they do not cause adverse effects in breastfed infants.34,41 Alprazolam and diazepam, with longer half-lives than some of the other benzodiazepines, should be avoided because of reports of infant sedation.34,41
Implications for practice
Perinatal anxiety is fairly common, and, when severe, has been linked to adverse pregnancy outcomes and to developmental and mental health problems in offspring. Early identification of and intervention for perinatal anxiety can help alleviate signs and symptoms, improve the perinatal experience, and reduce the risk for adverse outcomes. HCPs need to screen women for anxiety both during pregnancy and postpartum. When anxiety is identified, HCPs should conduct further assessment to determine whether the patient has a co-existing psychiatric disorder that merits referral and collaboration with a mental health specialist. Nonpharmacologic treatments such as CBT should be considered as first-line treatment, although some women may require medication to manage symptoms adequately. Risks and benefits of using medications to treat anxiety during the perinatal period should be considered on an individualized and ongoing basis.
Marian L. Farrell is Professor of Nursing at the University of Scranton in Scranton, Pennsylvania. She is also in private practice as a psychiatric nurse practitioner and clinical nurse specialist. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
1. Ross LE, McLean LM. Anxiety disorders during pregnancy and the postpartum period: a systematic review. J Clin Psychiatry. 2006; 67(8):1285-1298.
2. Bauer A, Knapp M, Parsonage M. Lifetime costs of perinatal anxiety and depression. J Affect Disord. 2016;192:83-90.
3. Bayrampour H, Al E, McNeil DA, et al. Pregnancy-related anxiety: a concept analysis. Int J Nurs Stud. 2015;55:115-130.
4. Rubertsson C, Hellström J, Cross M, Sydsjö G. Anxiety in early pregnancy: prevalence and contributing factors. Arch Womens Ment Health. 2014;17(3):221-228.
5. National Institute of Mental Health (NIMH). Generalized Anxiety Disorder Among Adults.
6. National Institute of Mental Health. Any Anxiety Disorder Among Adults.
7. American Psychiatric Association. Anxiety disorders. In: Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Arlington, VA: APA; 2013:222-226.
8. Marchesi C, Ossola P, Amerio A, et al. Clinical management of perinatal anxiety disorders: a systematic review. J Affect Disord. 2016;190:543-550.
9. Biaggi A, Conroy S, Pawlby S, Pariante CM. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J Affect Disord. 2016;191:62-77.
10. O’Hara MW, Stuart S, Watson D, et al. Brief scales to detect postpartum depression and anxiety symptoms. J Womens Health. 2012;21(12):1237-1243.
11. Zadeh MA, Khajehei M, Sharif F, Hadzic M. High-risk pregnancy: effects on postpartum depression and anxiety. Br J Midwifery. 2012;20(2):104-113.
12. Fairbrother N, Janssen P, Antony MM, et al. Perinatal anxiety disorder prevalence and incidence. J Affect Disord. 2016;200:148-155.
13. Hoang S. Pregnancy and anxiety. Int J Childbirth Educ. 2014;29(1):67-70.
14. Grigoriadis S, de Camps Meschino D, Barrons E, et al. Mood and anxiety disorders in a sample of Canadian perinatal women referred for psychiatric care. Arch Womens Ment Health. 2011;14(4):325-333.
15. American College of Obstetricians and Gynecologists. Screening for perinatal depression. Washington, DC: ACOG; 2015.
16. Spitzer RL, Kroenke K, Williams JB, Lowe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-1097.
17. Simpson W, Glazer M, Michalski N, et al. Comparative efficacy of the generalized anxiety disorder 7-item scale and the Edinburgh Postnatal Depression Scale as screening tools for generalized anxiety disorder in pregnancy and the postpartum period. Can J Psychiatry. 2014;59(8):434-440.
18. Somerville S, Dedman K, Hagan R, et al. The perinatal anxiety screening scale: development and preliminary validation. Arch Womens Ment Health. 2013;17(5):443-454.
19. Somerville S, Byrne SL, Dedman K, et al. Detecting the severity of perinatal anxiety with the Perinatal Anxiety Screening Scale (PASS). J Affect Disord. 2015;186:18-25.
20. Wenzel A, Haugen EN, Jackson LC, Robinson K. Prevalence of generalized anxiety at eight weeks postpartum. Arch Womens Ment Health. 2002;6(1):43-49.
21. Moran TE, Polanin JR, Wenzel A. The Postpartum Worry Scale-Revised: an initial validation of a measure of postpartum worry. Arch Womens Ment Health. 2014;17(1):41-48.
22. Moran TE, Polanin JR, Segre L, Wenzel A. The Postpartum Worry Scale-Revised: continuing validation with a sample of NICU mothers. Arch Womens Ment Health. 2015;18(2):221-228.
23. Yao B, Sripada RK, Klumpp H, et al. Penn State Worry Questionnaire-10: a new tool for measurement-based care. Psychiatry Res. 2016;239:62-67.
24. Matthey S, Fisher J, Rowe H. Using the Edinburgh postnatal depression scale to screen for anxiety disorders: conceptual and methodological consideration. J Affect Disord. 2013;146(2):224-230.
25. Ali NS, Azam IS, Ali BS, et al. Frequency and associated factors for anxiety and depression in pregnant women: a hospital-based cross-sectional study. Scientific World Journal. 2012;2012:653098.
26. Dunkel Schetter C, Tanner L. Anxiety, depression and stress in pregnancy: implications for mothers, children, research, and practice. Curr Opin Psychiatry. 2012;25(2):141-148.
27. Otte C. Cognitive behavior therapy in anxiety disorders: current state of the evidence. Dialogues Clin Neurosci. 2011;13(4):413-421.
28. Sockol LE, Epperson CN, Barber JP. A meta-analysis of treatments for perinatal depression. Clin Psychol Rev. 2011;31(5):839-849.
29. Stuart S, Koleva H. Psychological treatments for perinatal depression. Best Pract Res Clin Obstet Gynaecol. 2014;28(1):61-70.
30. Kittel-Schneider S, Reif A. Treatment of mental disorders in pregnancy and lactation: psychotherapy and other non-drug therapies. Neurologist. 2016;87(9):967-973.
31. Stahle S. Stahl’s Essential Psychopharmacology Prescriber’s Guide. 5th ed. New York, NY: Cambridge University Press; 2014.
32. Woo TM, Robinson MV. Pharmacotherapeutics for Advanced Practice Nurse Prescribers. Philadelphia, PA: F.A. Davis; 2016.
33. Rubinchik SM, Kablinger AS, Gardner JS. Medications for panic disorder and generalized anxiety disorder during pregnancy. Prim Care Companion J Clin Psychiatry. 2005;7(3):100-105.
34. Malm H, Artama M, Gissler M, Ritvanen A. Selective serotonin reuptake inhibitors and risk for major congenital anomalies. Obstet Gynecol. 2011;118(1):111-120.
35. Stephansson O, Kieler H, Haglund B, et al. Selective serotonin reuptake inhibitors during pregnancy and risk of stillbirth and infant mortality. JAMA. 2013;309(1):48-54.
36. Palmsten K, Setoguchi S, Margulis AV, et al. Elevated risk of preeclampsia in pregnant women with depression: depression or antidepressants? Am J Epidemiol. 2012;175(10):988-997.
37. Ewing G, Tatarchuk Y, Appleby D, et al. Placental transfer of antidepressant medications: implications for postnatal adaptation syndrome. Clin Pharmacokinet. 2015;54(4):359-370.
38. Huybrechts KF, Bateman BT, Palmsten K, et al. Antidepressant use late in pregnancy and risk of persistent pulmonary hypertension of the newborn. JAMA. 2015;313(21):2142-2151.
39. Ellfolk M, Malm H. Risks associated with in utero and lactation exposure to selective serotonin reuptake inhibitors. Reprod Toxicol. 2010;30(2):249-260.
40. LactMed: A Toxnet Database.
41. Brucker MC, King TL. Pharmacology for Women’s Health. 2nd ed. Burlington, MA: Jones & Bartlett Learning; 2017.
Web resources
A. integration.samhsa.gov/clinical-practice/GAD708.19.08Cartwright.pdf
B. drsarahallen.com/wp-content/uploads/2015/10/PerinatalAnxietyScreeningScale2.pdf