
Dalisa Barquero, DNP, MPH, WHNP-BC, is a women’s health nurse practitioner, clinical lead, at Mountain Park Health Center in Phoenix, Arizona.
Amber S. Shapton, DNP, FNP-BC, WHNP-BC, is medical director at Lincoln Avenue Medical-Dental Center, Yakima Valley Farm Workers Clinic, in Yakima, Washington.
Continuing education approval: This activity has been evaluated and approved by the Continuing Education Approval Program of the National Association of Nurse Practitioners in Women’s Health (NPWH) for 1.0 continuing education contact hours including 0.50 contact hours of pharmacology content now through February 28, 2025.
Target audience: Women’s health nurse practitioners and other advanced practice registered nurses who provide women’s and gender-related healthcare.
Educational objectives: At the conclusion of this educational activity, participants should be able to:
1.
Differentiate three primary headache types and red flags for secondary headaches.
2.
Discuss nonpharmacologic options for prevention and management of primary headaches during pregnancy and lactation.
3.
Describe pharmacologic options and special considerations for their use in prevention and management of primary headaches during pregnancy and lactation.
The authors have no actual or potential conflicts of interest in relation to this article.
Disclaimer: Participating faculty members determine the editorial content of the CE activity; this content does not necessarily represent the views of NPWH. This content has undergone a blinded peer review process for validation of clinical content. Although every effort has been made to ensure that the information is accurate, clinicians are responsible for evaluating this information in relation to generally accepted standards of care and integrating the information in this activity with that of established recommendations of other authorities, national guidelines, and individual patient characteristics.
Commercial support: This activity did not receive any commercial support.
Successful completion of the activity: Successful completion of this activity, J-23-01, requires participants to do the following:
1.
“Sign in” at the top right-hand corner of the page pathlms.com/npwh/courses/49662 if you have an NPWH account. You must be signed in to receive credit for this course. If you do not remember your username or password, please follow the “Forgot Password” link and instructions on the sign-in page. If you do not have an account, please click on the “Create an Account.”*
2.
Read the learning objectives, disclosures, and disclaimers.
3.
Study the material in the learning activity during the approval period (now through February 28, 2025).
4.
Complete the post-test and evaluation. You must earn a score of 70% or higher on the post-test to receive CE credit.
5.
Print out the CE certificate after you have successfully passed the post-test and completed the evaluation.
*
If you are an NPWH member, were once a member, or have completed CE activities with NPWH in the past, you have a username and password in our system. Please do not create a new account. Creation of multiple accounts could result in loss of CE credits as well as other NPWH services. If you do not remember your username or password, either click on the “Forgot Username” or “Forgot Password” link or call the NPWH office at (202) 543-9693, ext. 1.
Three primary headache types have been described by the International Headache Society, including migraine, tension-type, and cluster headaches.1,2 Primary headaches, although not associated with specific underlying physiologic or structural pathology, can affect cognitive and daily function and can be debilitating when severe. Up to 17% of pregnant persons experience primary headaches, mostly tension-type, and migraine.3 These headaches can exacerbate pregnancy-related discomforts and can potentially have significant consequences to the pregnant patient, fetus, and subsequently in the postpartum period, maternal–child bonding.3–5 The approach to management for primary headaches in pregnancy and lactation should be balanced with consideration for the potential risk of fetal harm or impact to the newborn, while providing symptomatic relief for the affected patient.3,5 Further, because pregnancy increases the risk for some secondary headache disorders associated with underlying pathology, headaches must be evaluated in the context of the overall pregnancy and postpartum presentation.6 This article provides an overview of assessment, diagnosis, and considerations for the treatment of primary headaches during pregnancy and lactation.
Primary headaches in pregnancy and during lactation
Patients may experience primary headaches due to a pre-existing diagnosis or for the first time during pregnancy or postpartum.3 In patients considering pregnancy or who are currently pregnant with a history of primary headaches, a review of headache symptoms, frequency, and intensity provides a baseline. These patients may be using medications for acute headache episodes or for headache prevention that may need to be adjusted during pregnancy and lactation.
Clinicians should be apprised of the hormonal impact on migraine headaches, cognizant that while estrogen fluctuations can contribute to migraines outside of pregnancy, rising estradiol levels during pregnancy often lead to an improvement regarding frequency and intensity.1 Up to three-fourths of pregnant persons with a history of migraines experience complete resolution during pregnancy.6 This symptom improvement also can extend to the postpartum period during lactation.7 Hormonal changes during pregnancy contribute only modestly to an improvement of tension-type headaches, but it is uncommon for tension-type headaches to worsen during pregnancy. Cluster headaches are not as common as the other primary headaches and typically have no change during pregnancy in relation to frequency and intensity with limited data on course during lactation.7,8
Assessment and diagnosis
When a pregnant patient presents with a headache, the health history should include onset, duration, location, characteristics and intensity of pain, any aggravating or alleviating factors, and previous treatments.2,7,9 A systematic approach to the evaluation of headaches during the postpartum period also should be incorporated.7 Current medications should be reviewed. Blood pressure should be assessed and if the patient has neurologic symptoms other than the headache itself, a focused neurologic physical examination should be completed. This encompasses evaluating mental status as well as appearance and speech. Clinicians should include an assessment of cranial nerves including vision with visual fields, fundoscopy, pupils, eye movements, and observation for facial symmetry. Additionally, monitoring muscle strength for unilateral weakness and coordination along with reflexes is indicated.9,10
Pain with migraine headaches is typically characterized as unilateral, moderate-to-severe intensity, throbbing in nature, and may be exacerbated by physical activity. Migraines are generally preceded by prodromal symptoms. These symptoms may include but are not limited to photophobia or phonophobia, nausea, mood changes, food cravings, or difficulty concentrating. Prodromal symptoms can last up to 48 hours and may or may not continue once the headache begins.1,11 Up to 25% of patients experience an aura, with reversible focal neurologic symptoms that precede or accompany the headache. Vision changes are most common and manifest as lights or lines spreading peripherally, vision loss, or a combination of these. The patient may report numbness or tingling and may exhibit word-finding difficulty.12 Aura symptoms can last up to 60 minutes. Pain may not resolve without treatment and can last up to 72 hours. Patients will often experience a postdromal phase similar to the symptoms in the prodromal phase with migraine headaches.1,11
Tension-type headache pain is described as bilateral mild-to-moderate pressure that does not pulsate. Tension-type headaches are not associated with aura or aggravated by physical activity. Rarely do patients have nausea, photophobia, or phonophobia. These headaches frequently respond to over-the-counter medication and can last from 30 minutes to 7 days.1,13
Cluster headaches have an abrupt onset, are unilateral, with pain often behind the eye described as severe stabbing, and may be associated with lacrimation, nasal congestion, and ptosis on the affected side. These headaches occur in clusters lasting a few weeks with each episode lasting 15 to 180 minutes. Cluster headaches are much more common in biologic males than in biologic females.1,7,13,14
A low threshold and timely investigation of headaches during pregnancy and in the postpartum period that do not fit the characteristics of primary headaches is warranted. Some serious conditions such as preeclampsia, stroke, benign intracranial hypertension, and enlarging pituitary adenomas may manifest with headache.1,6 Red flags for potential secondary headaches include a change in baseline headache, thunderclap headache, fever, elevated blood pressure, neurologic deficits, change in consciousness, or abnormal labs including elevated liver enzymes, creatinine, thrombocytopenia, or thrombocytosis.1,15 Patients with red flags need an immediate referral for further evaluation. Brain magnetic resonance imaging (MRI) is warranted for primary headaches in certain scenarios including situations where a migraine with aura occurs for the first time in pregnancy or if the headache is prolonged and not improved with analgesics. A brain MRI also is indicated for first-time cluster headaches due to the rare occurrence of this type of headache.6
Management
Nonpharmacologic methods are the first-line approach for primary headache management in pregnancy and lactation.7 Lifestyle modifications such as incorporating healthy foods, regular exercise, getting adequate sleep, and using relaxation techniques may be helpful. Behavioral modalities such as the use of a headache diary and identifying triggers will empower patients as they learn more about their body’s response and take a more proactive approach to headache prevention. Mindfulness-based interventions such as mindful breathing, yoga postures, and meditation as part of relaxation training can reduce stress and have potential as a nonpharmacologic modality for prevention and management of acute headache.16 Nevertheless, undermanaged headaches can lead to stress, sleep deprivation, depression, and poor nutritional intake, which in turn can have negative consequences for the pregnant patient, fetus, lactating person, or newborn.6
Preventive therapy
Although not all studies support the use of pharmacologic interventions to prevent primary headaches in pregnancy, prophylactic therapy is a consideration for patients who have frequent or severe episodes. A discussion on the benefits and risks of available treatment options as part of shared decision making is warranted, avoiding exposure to medications with known or uncertain risks.1,3,5
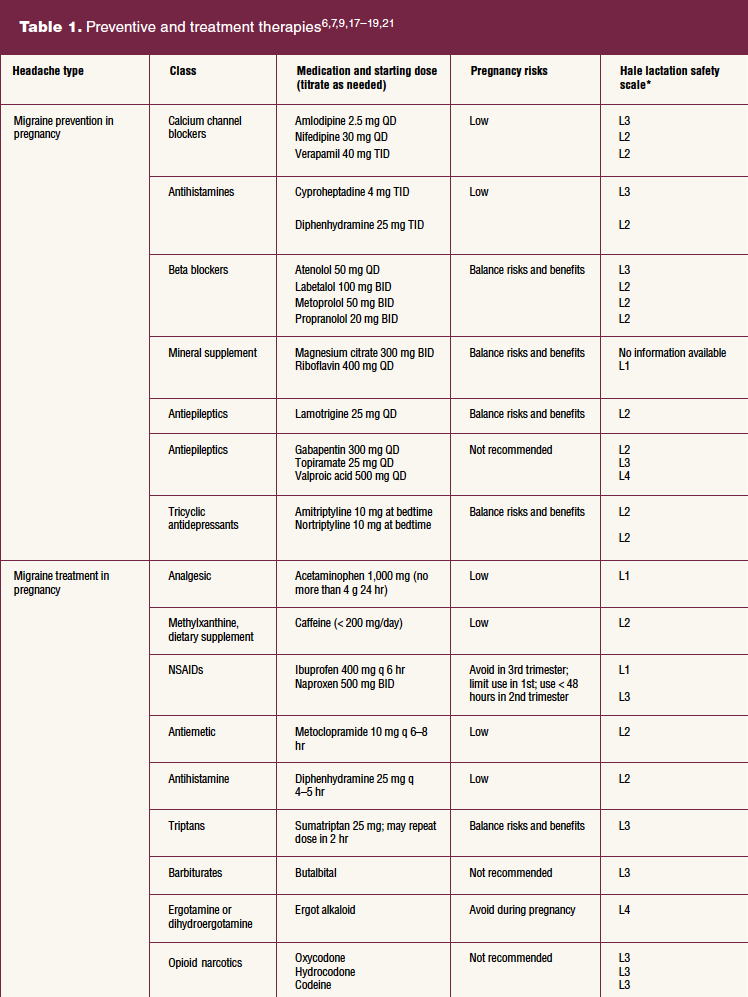
Calcium channel blockers and antihistamines have relatively safe profiles and can be considered as first-line treatment for the prevention of migraine headaches during pregnancy.1,7 Beta blockers also can be considered for migraine headache prevention, as some data support their use in the nonpregnant population and in obstetric populations for other indications, but risks and benefits should be carefully weighed when determining whether to use.1,5 When possible, tapering off prior to labor should be achieved with beta blockers in the third trimester, as they can induce neonatal pharmacologic effects like bradycardia, hypotension, and hypoglycemia.6 Mineral supplements like riboflavin and magnesium citrate have limited data and require balancing risks and benefits but are generally believed safe during pregnancy.1,7 Antiepileptics like sodium valproate are contraindicated for the prevention of migraine headaches in pregnancy due to their teratogenicity and adverse neurocognitive outcomes.5,6 Topiramate also is associated with increased risk of adverse fetal effects. Data on gabapentin are limited, but there is suspicion for associated fetal osteologic deformities and it is therefore also not recommended. Lamotrigine has a good safety profile when compared to other antiepileptic drugs but warrants a thorough discussion regarding risks and benefits.3,6 Similarly, patients should be counseled that the use of tricyclic antidepressants for prevention of migraine headache has a potential risk for teratogenic effects, although clear causal relationship cannot be proved.5,6
There is an increase in options for prevention of migraines during lactation when compared to pregnancy.9 Supplements such as riboflavin and magnesium citrate would be considered the safest but have been shown to be the least effective for prevention of migraines.7,9,17 Alternative medications with relatively safe profiles for the infant and lactating parent include calcium channel blockers, beta blockers, tricyclic antidepressants, and antiepileptics with the exception of valproic acid.7,9,18 There are more safety concerns for medication use during lactation for preterm infants and newborns, but these decrease as the infant ages.7
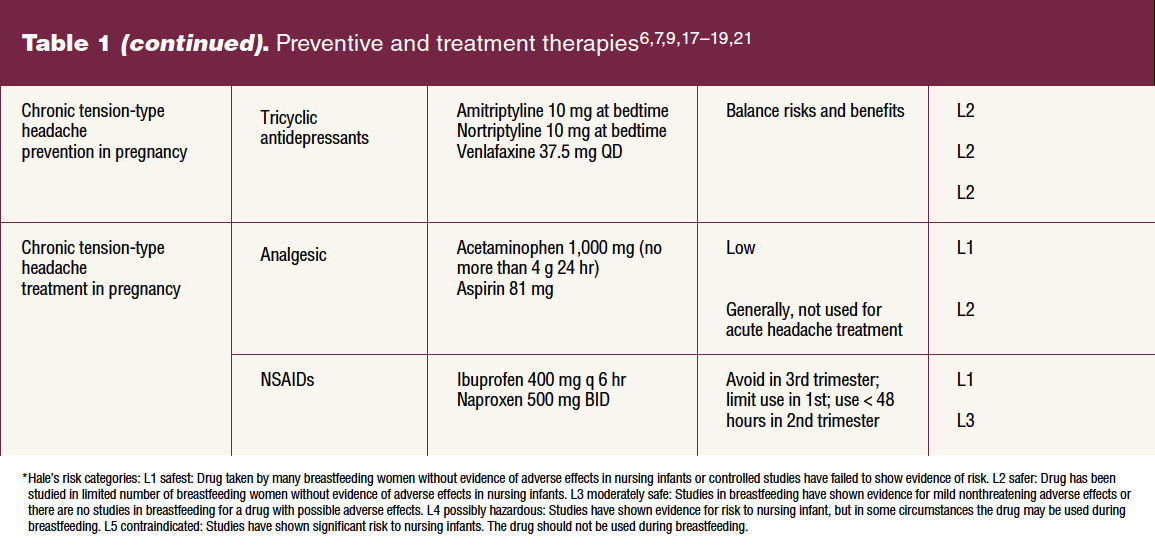
Tension-type headaches are common but generally do not cause patients to seek out medical attention due to their mild-to-moderate intensity.7 If during shared decision making, preventive treatment for tension-type headache is sought, pregnant patients can consider the use of tricyclic antidepressants, balancing the risks and benefits of use.9 These also can be used during lactation for the prevention of tension-type headache as they appear to be safe based on limited data.1,9,18
Acute therapy
Pharmacologic treatment of acute episodes of primary headaches in pregnancy should be approached in a stepwise fashion guided by the severity and frequency of the headache and consideration for therapies with known fetal and maternal safety, while balancing risks and benefits.1,3,7,9 The management of acute primary headaches in pregnancy at home should be limited to 2 days or less per week to avoid chronic headaches caused by medication overuse. Acetaminophen can be used as initial therapy for acute migraine, with total exposure limited to 4 g over 24 hours.1,9 Combination products containing acetaminophen and caffeine can be used but should not exceed 200 mg of caffeine a day.1,19 The use of nonsteroidal anti-inflammatory medications (NSAIDs) for intractable migraine should be limited to the second trimester and, if repeated administration is necessary, should not exceed 48 hours. For persistent migraine headache in pregnancy, the use of intravenous or enteral metoclopramide 10 mg alone or in combination with diphenhydramine 25 mg is an option.1,7
The use of combination products containing butalbital is not recommended due to concern for medication-overuse headaches and addiction.1,7 Ergot alkaloid-containing products should not be used during pregnancy as these can stimulate myometrial contractions. Opioid narcotics should not be used due to the potential impact on the fetus.1,6,7 Cautious use of sumatriptan and prednisone as secondary therapies can be considered when headache remains unresolved.1,7 On occasion, acute headache management during pregnancy may include hospital admission for parenteral administration.1
Treatment of tension-type headaches during pregnancy is limited to acetaminophen and very limited use of ibuprofen and naproxen for less than 48 hours during the second trimester. The use of ibuprofen, acetaminophen, and low-dose aspirin during lactation has a supported safe profile. Data are limited, but it is probably safe to use naproxen for treatment of tension-type headaches during lactation.1,9,18 Table 1 provides information on medications for the prevention and treatment of primary headaches during pregnancy and lactation.
Patient education and resources
A multicomponent program for headache management during pregnancy and lactation should be incorporated. This should include lifestyle modifications, conventional pharmacologic therapies, patient education, and supportive complementary measures. These complementary measures include dietary changes and behavioral modification.16 Referral to a registered dietitian can be considered to explore dietary habits, with emphasis on the importance of appropriate hydration and avoiding fasting states, and to provide support for healthy diet in pregnancy and lactation. Additionally, a referral to a behavioral health specialist can support the patient with headache by focusing on techniques for stress reduction and mindfulness practices to increase self-efficacy.20
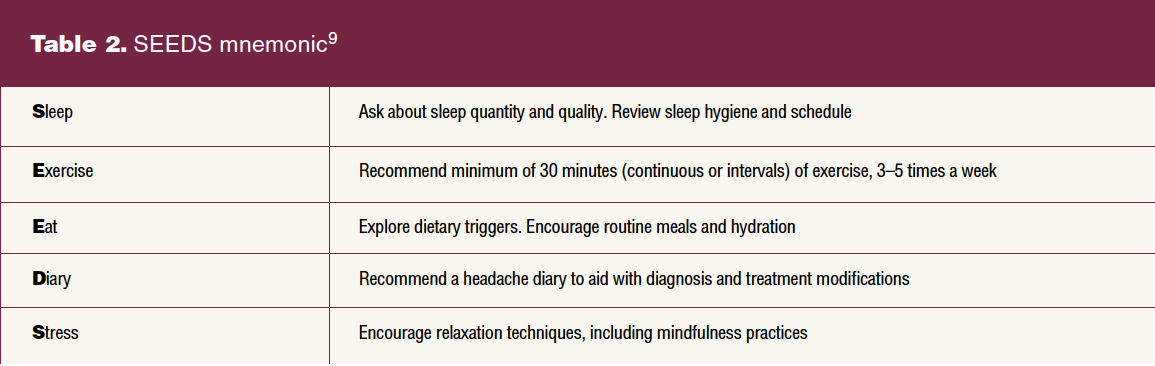
Patients should be counseled on red flags that indicate an urgent need for evaluation. Severe headache can be the first indicator of preeclampsia. Clinicians can help the pregnant or lactating person mitigate the severity and frequency of headaches by modifying common headache triggers using the mnemonic SEEDS (sleep, exercise, eat, diary, stress) as described in more detail in Table 2.20
Conclusion
It is imperative for the clinician to systematically engage in the assessment and management of headaches in pregnancy and during lactation. Failure to differentiate between primary and secondary headaches or recognize red flags may contribute to morbidity or mortality. Risks and benefits should be balanced when determining appropriate pharmacologic treatment and prevention strategies for primary headaches. Utilizing nonpharmacologic interventions also can provide benefit in symptomatic relief. Understanding the phenomenon of primary headaches in pregnancy and lactation and available management options will facilitate safe and effective treatment.
References
1 American College of Obstetricians and Gynecologists. Headaches in pregnancy and postpartum. ACOG Clinical Practice Guideline No. 3. Obstet Gynecol. 2022;139(5):944-972.
2 Headache Classification Committee of the International Headache Society (IHS). The international classification of headache disorders. Cephalgia. 2018;38:1-211.
3 Saldanha IJ, Cao W, Bhuma MR, et al. Management of primary headaches during pregnancy, postpartum, and breastfeeding: a systematic review. Headache. 2021;61(1):11-43.
4 Goadsby PJ, Lantéri-Minet M, Michel MC, et al. 21st century headache: mapping new territory. J Headache Pain. 2021;22(1):19.
5 Saldanha IJ, Roth JL, Chen KK, et al. Management of Primary Headaches in Pregnancy. Report No. 20(21)-EHC026. Comparative Effectiveness Review 234. Rockville, MD: Agency for Healthcare Research and Quality; 2020. https://www.ncbi.nlm.nih.gov/books/NBK564853/.
6 Negro A, Delaruelle Z, Ivanova TA, et al. Headache and pregnancy: a systematic review. J Headache Pain. 2017;18(1):106.
7 Rayhill M. Headache in pregnancy and lactation. Continuum (Minneap Minn). 2022;28(1):72-92.
8 Raffaelli B, Siebert E, Körner J, et al. Characteristics and diagnosis of acute headache in pregnant women – a retrospective cross-sectional study. J Headache Pain. 2017;18(1):114.
9 Becker WJ, Findlay T, Moga C, et al. Guideline for primary care management of headache in adults. Can Fam Physician. 2015;61:670-679.
10 Fritz D, Musial MK. Neurological assessment. Home Healthcare Now. 2016;34(1):16-22.
11 Goadsby P, Holland P, Martins-Olivera M, et al. Pathophysiology of migraine: a disorder of sensory processing. Physiol Rev. 2017;97:553-622.
12 Kalidas K. Migraines in women. Contemporary OB/GYN. 2017;62(8):12.
13 Goetz A, McCormick S, Phillips R, et al. Diagnosing and managing migraine. Am J Nurs. 2022;122(1):32-43.
14 Lindemann C. Cluster headache: a review of clinical presentation, evaluation, and management. JAAPA. 2022;35(8):15-19.
15 Chinthapalli K, Logan AM, Raj R, Nirmalananthan N. Assessment of acute headache in adults–what the general physician needs to know. Clin Med (Lond). 2018;18(5):422-427.
16 Riggins N, Ehrlich A. The use of behavioral modalities for headache during pregnancy and breastfeeding. Cur Pain Headache Rep. 2021;25(10):66.
17 National Library of Medicine. Drugs and lactation database: Magnesium. https://www.ncbi.nlm.nih.gov/books/NBK501339
18 Hale TW. Hale’s Medications & Mothers’ Milk, 2021: A Manual of Lactational Pharmacology. New York, NY: Springer; 2021.
19 National Library of Medicine. Drugs and lactation database: Caffeine. https://www.ncbi.nlm.nih.gov/books/NBK501467/.
20 Robblee J, Starling AJ. SEEDS for success: lifestyle management in migraine. Cleve Clin J Med. 2019;86(11):741-749.
21 Lampl C, Katsarava Z, Diener H-C, et al. Lamotrigine reduces migraine aura and migraine attacks in patients with aura. J Neurol Neurosurg Psychiatry. 2005;76:1730-1732.
Womens Healthcare. 2023;11(1):4-10. doi: 10.51256/WHC022304
Key words: primary headache, pregnancy, migraine, headache treatment, lactation