
The National Association of Nurse Practitioners in Women’s Health (NPWH) affirms the right of all individuals to quality, evidence-based sexual and reproductive health (SRH) care that is non-judgmental, respectful, and culturally appropriate. SRH is an important component in individuals’ overall physical, emotional, and social well-being. SRH encompasses sexuality, sexual relationships, and all matters related to the function and processes of the reproductive system.1 The SRH of one individual often intertwines with that of another individual or individuals.
Sexual and reproductive healthcare includes health promotion, disease prevention, and identification and treatment of disease. As such, SRH care addresses issues such as sexuality, reproductive life planning, fertility, contraception, preconception health, all pregnancy options, reproductive assistance options, sexually transmitted infections (STIs)/HIV infection, SRH-related vaccinations (e.g., HPV vaccination), sexual dysfunction, reproductive health-related illnesses such as breast and cervical cancers, and violence within relationships.2,3
NPWH asserts that women’s health nurse practitioners (WHNPs) have a uniquely strong educational foundation to provide SRH care for all individuals, inclusive of all gender identities and sexual orientations. The specific purpose of this position statement is to support the role of WHNPs in the provision of SRH care for males. Providing quality SRH care to males not only helps them preserve and promote their own health but also helps optimize SRH outcomes in females. Of note, throughout this position statement, we use the terms male, female, man, and woman to denote both cisgender and transgender individuals.
The role and the competencies of WHNPs are not setting specific. However, the environment in which WHNPs practice may or may not include opportunities for direct interaction with males as patients. WHNPs who provide healthcare in settings that include male and female patients (e.g., family practice offices, family planning clinics, school- and college-based health centers, reproductive endocrinology/fertility centers) can reach males who might not otherwise receive SRH care. WHNPs who provide care in settings where males are generally not seen as patients (e.g., Ob/Gyn offices/clinics) may still have opportunities to reach male partners for a coordinated approach to SRH.
Background
Providing SRH care for males requires attention to removing barriers and innovation to engage them in a variety of settings. Males, as they move into adolescence and young adulthood (and exit pediatric care), are less likely than their female counterparts to seek preventive healthcare that can include SRH services.4,5 In fact, a large proportion of young men do not know where to access SRH care.4,6,7 Even when adolescent or young adult males are seen in a healthcare setting, many healthcare providers (HCPs) do not address SRH.4,8-10 Recent studies indicate that if discussion about SRH with male patients does occur, it is often limited to how to decrease STI risk, and that although males are willing to discuss SRH-related issues, they prefer that the HCP initiate the discussion.7,9
Guidance for HCPs regarding the content and provision of SRH for males is often combined with recommendations for female SRH care. In 2014, the U.S. Office of Population Affairs (OPA) and the CDC developed and published recommendations for providing quality family planning and related preventive health services that include both female and male SRH services.2 Family planning services, as defined in this document, include reproductive life planning, contraception, preconception health , pregnancy testing and counseling, basic infertility services, and STI screening and treatment. Other important SRH care components include screening for reproductive cancers, providing appropriate immunizations, and providing or referring for prenatal and abortion care as needed.3 The audience for these recommendations extends beyond providers at sites dedicated to family planning services to providers in all primary care settings.
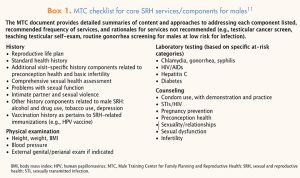
To support HCPs in providing male SRH services, the Male Training Center for Family Planning and Reproductive Health (MTC) elaborated on the OPA/CDC document with the publication of Preventive Male Sexual and Reproductive Health Care: Recommendations for Clinical Practice.11 The MTC document provides recommendations for eight health history components, three physical examination components, and six laboratory tests, as well as seven recommendations for counseling based on identification of risk.11 Box 1 outlines the MTC’s recommendations for SRH services for males. HCPs can find additional guidance regarding male SRH care through multiple organizations’ publications—and links to these publications—provided in Box 2.
Box 2. Sample resources for male sexual and reproductive health
|

Implications for WHNP practice
WHNPs provide SRH care for males directly (or indirectly) as primary care providers or as specialty care providers in areas such as reproductive endocrinology/fertility and breast health.
- WHNPs who provide healthcare solely for females can give their patients information on male SRH to share with their male partners. The goal is to support male SRH that enhances the health of female patients and optimizes family planning, pregnancy outcomes, and the physical and emotional health of relationships.
- WHNPs who provide healthcare solely for females may consider incorporating male SRH care in a couple’s approach in the clinical setting. Again, the goal is to support male SRH, which enhances the health of female patients and optimizes family planning, pregnancy outcomes, and the physical and emotional health of relationships.
- WHNPs providing care in settings where males are routinely seen (e.g., family practice offices, family planning clinics, school- and college-based health centers, reproductive endocrinology/fertility centers) have opportunities to provide direct male SRH care in such settings. The goal expands beyond enhancing the health of female patients to enhancing the SRH of males.
- WHNPs are educationally prepared to provide SRH care for individuals inclusive of all gender identities and sexual orientations. WHNPs provide SRH care based on the individual needs of each patient.
Recommendations
NPWH recommends that WHNPs do the following:
- Engage in learning opportunities to maintain, update, and/or expand knowledge and skills that enable them to provide and promote SRH care for all individuals and couples within the context of their clinical setting.
- Include provision of SRH care for individuals inclusive of all gender identities in collaborative practice agreements in states where such written agreements are required.
- Establish referral resources for SRH concerns to meet the needs of patients and partners.
NPWH will provide leadership to ensure that:
- Faculty of WHNP programs have resources to continue to provide up-to-date, evidence-based male SRH content in the curriculum.
- Continuing education programs and resources are available for WHNPs to maintain, update, and/or expand their knowledge and skills with regard to male SRH care.
- WHNPs have SRH informational resources to share with both male and female patients.
- WHNPs’ scope of practice regulations do not restrict them from providing male SRH care within the parameters of their education and competency.
References
- World Health Organization. Defining Sexual Health: Report of a Technical Consultation on Sexual Health, 28-31 January 2002. Geneva, Switzerland: WHO Press, 2006. www.who.int/reproductivehealth/publications/sexual_health/defining_sexual_health.pdf.
- Gavin L, Moskosky S, Carter M, et al. Providing quality family planning services: recommendations of CDC and the U.S. Office of Population Affairs. MMWR Recomm Rep. 2014;63(RR04):1-54.
- United Nations Population Fund. Sexual and Reproductive Health. 2016. unfpa.org/sexual-reproductive-health
- Chabot M, Lewis C, de Bocanegra H, Darney P. Correlates of receiving reproductive health care services among U.S. men aged 15 to 44 years. Am J Mens Health. 2011;5(4):358-366.
- Bersamin M, Fisher DA, Marcell AV, Finan LJ. Defi cits in young men’s knowledge about accessing sexual and reproductive health services. J Am Coll Health. 2017;65(8):579-584.
- Bersamin M, Fisher DA, Marcell AV, Finan LJ. Reproductive health services: barriers to use among college students. J Community Health. 2017;42(1):155-159.
- Tyler C, Warner L, Gavin L, Barfield W. Receipt of reproductive health services among sexually experienced persons aged 15-19 years—National Survey of Family Growth, United States, 2006-2010. MMWR Suppl. 2014;63(2):89-98.
- Choiriyyah I, Sonenstein FL, Astone NM, et al. Men aged 15-44 in need of preconception care. Matern Child Health J. 2015;19(11):2358-2365.
- Same RV, Bell DL, Rosenthal SL, Marcell AV. Sexual and reproductive health care: adolescent and adult men’s willingness to talk and preferred approach. Am J Prev Med. 2014;47(2):175-181.
- Warner JN, Frey KA. The well-man visit: addressing a man’s health to optimize pregnancy outcomes. J Am Board Fam Med. 2013;26(2):196-202.
- Marcel AV, Male Training Center for Family Planning and Reproductive Health. Preventive Male Sexual and Reproductive Health Care: Recommendations for Clinical Practice. 2014. maletrainingcenter.org/wp-content/uploads/2014/09/MTC_White_Paper_2014_V2.pdf
- NPWH/AWHONN. Women’s Health Nurse Practitioner: Guidelines For Practice and Education. 7th ed. Washington DC: NPWH/AWHONN; 2014.
- National Certifi cation Corporation. 2018 Candidate Guide Women’s Health Nurse Practitioner. Chicago, IL: National Certifi cation Corporation; 2018.