
Traditional contraceptive counseling has involved provider and patient discussion during office visits. This pilot study sought to introduce a technology-enhanced counseling intervention utilizing features of the Bedsider website. This article describes the experiences of patients and clinic staff in a Title X family planning clinic in the northeastern United States during implementation of this project.
| Key words: contraception counseling, bedsider.org, family planning, long-acting reversible contraceptives, LARC |
In the United States, approximately 50% of pregnancies are unintended; the U.S. continues to have one of the highest rates of unintended pregnancy among all developed countries.1 Although unintended pregnancies occur among women of all demographic groups, those who are young, unmarried, poor, and from an ethnic or racial minority group have the highest rates of unintended pregnancy.2 For women aged 18-29 years, high unintended pregnancy rates have been associated with a low level of contraceptive knowledge, low use, and fear of side effects, as well as ambivalence regarding pregnancy and mistrust of government-supported family planning services.3,4 To reduce these high rates, the CDC now recommends counseling patients about the use of long-acting reversible contraceptives (LARC), including intrauterine contraceptives (IUCs) and the subdermal implant, as first-line, highly effective options for pregnancy prevention.5,6
Researchers have documented the superiority of LARC methods over short-acting methods (pills, patches, rings, barrier methods) in lowering rates of unintended pregnancy.7,8 The short-acting contraceptives are less effective than LARC methods because they are more likely to be used incorrectly or inconsistently or to not be used at all.9 If 10% of women aged 20-29 years switched from oral contraceptives to LARC, total costs would be reduced by about $288 million per year.10 Also, LARC methods could reduce disparities associated with unintended pregnancy by enabling women to have greater control over the timing of their pregnancies.11
According to researchers who analyzed data from the 2011-2013 cycle of the National Survey of Family Growth, LARC use increased five-fold over the past decade among females aged 15-44 years.12 Even with this increase, overall rates of LARC use are low, with only 7.2% of women choosing them. For females aged 15-24, LARC use is even lower, accounting for only 5% of the contraceptive methods in this age group.12 Low utilization has been ascribed to a variety of barriers, including high cost (especially higher initial cost), lack of awareness and knowledge about LARC, lack of access to a healthcare provider (HCP) trained in LARC insertion, and restrictive clinic protocols.13-16
With recent advances in technology and new approaches to healthcare delivery, patient education has moved from passive delivery of healthcare information to a more interactive approach. These changes allow patients to be more knowledgeable and active participants in the healthcare decision-making process. This model of patient education has resulted in technology-based patient decisional-aid tools and a plethora of Internet-based applications (apps) and mobile health apps, including apps focused on contraceptive methods and choices. These decisional-aid tools can assist HCPs in delivering health education content that is visible, colorful, auditory, and interactive, facilitating the transfer and retention of information.17
Based on learning theories, the most effective decisional-aid tools are available in multiple languages, are suitable for patients with low literacy, are readily available for repeated use, and require limited knowledge of technology.18 Researchers have demonstrated that these decisional-aid tools are effective, increase patient knowledge, are acceptable both to patients and HCPs, and are cost effective.19-22
Considering the low rate of LARC use and the consistently high rate of unintended pregnancy in the U.S., the authors sought to implement a pilot trial of technology-enhanced contraceptive counseling to increase LARC use among young women who sought care at a Title X family planning clinic in the northeastern U.S. For the purpose of this study, LARC methods were defined as either the subdermal implant or an IUC (progesterone or copper).
Purpose
Specific aims of the study were (1) to incorporate a technology-enhanced counseling intervention utilizing features of the Bedsider website23 at family planning visits to increase LARC use, (2) to determine the feasibility and acceptability of the technology-enhanced counseling intervention for both patients and HCPs, and (3) to measure the difference in LARC use between the intervention and control groups.
Methods
Setting
The participating clinic in this study was Health Quarters, Inc., a non-profit, Title X provider of confidential reproductive healthcare. Services include contraceptive care, testing and treatment of sexually transmitted infections, gynecologic examinations, and sexual health education services for adolescents, women, and men in northeastern Massachusetts. This clinic provides care to uninsured and underinsured patients regardless of their ability to pay for services. Approximately 93% of patients who seek care at this site are at 250% below the federal poverty level. The clinic is located in a city in which nearly 75% of residents identify as Hispanic or Latino. It employs multilingual and multicultural staff members who reflect the community: the medical director is fluent in Spanish and the medical assistants (MAs), office assistant, and nurse practitioner (NP) are bilingual in English and Spanish.
Institutional Review Board approval to conduct the study was granted through the university of the principal investigator and supported by the clinic’s board of directors. All clinic staff members who interacted with study participants were trained in the ethical conduct of research. Data were collected from February 2015 through December 2015.
Sample
A convenience sample who met inclusion criteria—female gender; age, 18-29 years; a person seeking contraceptive services; and an English speaker—were asked to participate. At the time of the study, the Bedsider website was in English only, so women who could not read, speak, or understand English were excluded. Because the study incorporated features of the Bedsider website into contraceptive counseling, women who were pregnant or seeking pregnancy were excluded. Females younger than 18 years were excluded to ensure delivery of confidential services without parental notification of study participation.
Measures
Limited demographic information was collected to increase participant confidentiality. Contraceptive information, including history, use, and questions relating to reproductive and pregnancy coercion, were assessed via standardized questions adapted from the CDC.24,25
Procedure
Women who met inclusion criteria were recruited at the time of registration for their clinic visit and were asked by a front desk staff member if they wanted to participate in a study about contraceptive methods. Those who were interested were referred to the MA, who provided a brief overview of the study, obtained informed consent, and allowed the participant to join either the intervention group or the control group. All participants completed a pre-test study questionnaire on an iPad® prior to receiving any contraceptive counseling.
Women in the intervention group received the Bedsider website-based intervention. Specific Bedsider website features used in this intervention included the Method Explorer page, with emphasis on the most effective methods—that is, LARC—and the Compare Methods page, a side-by-side comparison of methods with respect to effectiveness, side effects, hormones, and cost. Participants were instructed to view information about the different methods while they waited for the NP to begin the visit (typical wait, 10-15 minutes). The NP reviewed the webpages with the patient as part of the contraceptive counseling process, which also included a discussion about the effectiveness, risks, benefits, method of action, medical eligibility, and instructions on use for the various contraceptives. The final choice of method was recorded. Post-intervention study questionnaires that measured contraceptive behaviors were completed at a 6-week follow-up appointment.
Women in the control group received usual care, which entailed a brief discussion with the MA about contraceptive methods and then face-to-face counseling with the NP, who discussed the effectiveness, risks, benefits, method of action, medical eligibility, and instructions on use for the various contraceptives. The final choice of method was recorded. Post-study questionnaires were completed at the 6-week follow-up.
Results
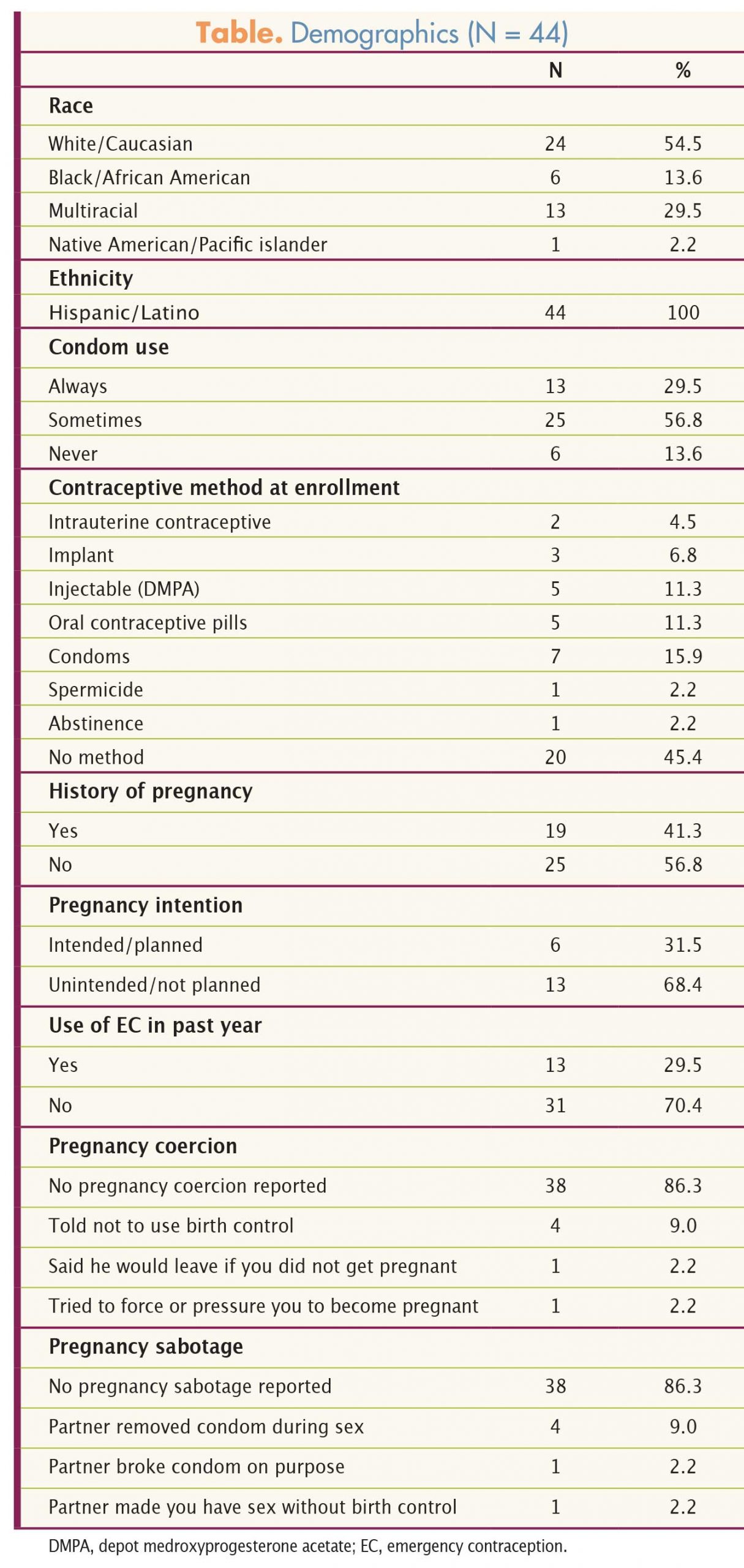
A total of 44 women enrolled in the study, 24 in the Bedsider intervention group and 20 in the control group. Twenty-five women completed the 6-week follow-up measures. Mean age for all participants was 22.2 years. Most participants self-identified as white/Caucasian (n = 24; 54.5%) or multiracial (n = 13; 29.5%). All participants reported their ethnicity as Hispanic, which is representative of the city and clinic populations. At enrollment, 20 participants (45.4%) reported using no contraceptive. In the previous year, 13 participants (29.5%) reported using emergency contraception one or more times. The Table provides demographic and contraceptive history information.
{kind=link}
Aim 1
At the beginning of the study, 11% of the women were using an IUC or implant. Regardless of whether women chose to join the intervention group or to receive usual care, LARC use increased during the study. Of the 25 women who returned for the 6-week follow-up, 29% of those in the intervention group and 36.6% of those in the control group had chosen a LARC method. Overall contraceptive use increased. At enrollment, 45.4% of the participants reported not using any form of contraception. At the 6-week follow-up, only 12% of the 25 women were still undecided about their contraceptive method.
Aim 2
Technology-enhanced counseling using the Bedsider website was both feasible and acceptable. Although no formal qualitative interviews were conducted, study meetings with the clinic staff (MAs and NP) elicited positive feedback and no reports of technology-related problems from staff or participants. Staff members thought that the Bedsider website was a helpful adjunct to counseling. It neither shortened nor lengthened the total amount of time spent discussing contraceptive methods.
Aim 3
Overall LARC use increased with contraceptive counseling, regardless of whether it was traditional face-to-face counseling by the NP or traditional counseling enhanced by use of the Bedsider website. The intervention and control groups did not differ significantly with respect to LARC use.
Clinical implications
Although the results of this small pilot study were not statistically significant for an increase in LARC use, they are clinically interesting and have important implications for NPs who work with women at risk for unintended pregnancy. Of note, almost half the participants were not using any form of contraception at study enrollment even though they were sexually active and at risk for pregnancy. At follow-up, only 12% of participants were still undecided about their contraceptive method. Contraceptive counseling, whether done in a traditional face-to-face format with the NP or enhanced with technology, was effective in helping women choose a method.
Initial aims of this study were to incorporate technology-enhanced contraceptive counseling into practice and determine the feasibility and acceptability of this process. Use of digital media as an adjunct to traditional conversations about contraception has been noted to fill gaps that women experience when trying to access contraceptive information.26 The clinic did not previously use any technology-based counseling for patients who were trying to choose a contraceptive method. Because of their ease of use, iPads were the electronic devices chosen to access the Bedsider website. To eliminate possible distractions, all preloaded applications were removed; only a shortcut to the Bedsider website was visible to participants. The Methods Explorer and Compare Methods webpages were chosen for inclusion in the study because of their application to clinical practice in helping patients understand available methods, as well as the benefits and limitations of each method. These webpages are colorful and easy to understand, and provide pictures and brief text describing the main features of each method.
No technology-related problems were reported during the study. Prior to data collection, the iPads were connected to the clinic’s password-protected wireless Internet. Webpages loaded quickly, and participants were able to navigate the Bedsider website easily after orientation by the MA. Tablets were stored in a locked cabinet when not in use and the MAs were responsible for distributing and collecting the devices when participants were done with their visit. Although clinic staff initially expressed concerns about damaged or stolen tablets, no instances of theft or breakage occurred during the study.
Consistent with existing research, the participants were receptive to using the Bedsider website. In the past, patients have found the website convenient and easy to navigate and appreciated feature formats such as videos and pictures.27 Decisions about contraceptives are complex, multifaceted, and personal. Aids such as the Bedsider website can facilitate contraceptive decision making by allowing women to consider their own needs, values, and personal preferences, and may be particularly useful in low-resource settings.28
At enrollment, LARC use was low (11%). The authors noted an increase in LARC use for both the intervention group (29%) and the control group (36.6%)—the difference between groups was not significant—highlighting that either technology-enhanced counseling or usual care delivered by an NP favorably affected LARC use rates. The control group had slightly higher LARC uptake, but the reasons for this difference are unclear. It may have been related to individual women’s preferences or selection bias (the women self-selected into the intervention or control group). Other researchers have reported that use of the Bedsider website over a 12-month period increased the likelihood that women would use a more effective birth control method.29 Those findings were not statistically supported by this study, but the small sample size and shorter (6-week) measurement point must be considered when interpreting the results.
Although the overarching aim of the study was to increase the use of LARC methods by women attending a family planning clinic, attention was paid to each woman’s preferences and concerns. HCPs need to ensure that all contraceptive counseling is provided in a respectful manner that supports each woman in identifying the method that best suits her needs, whether or not it is a LARC method. In this study, participants received non-biased contraceptive counseling regardless of whether they joined the intervention group or the control group. Their final choice of method was supported irrespective of the method selected.
Limitations
Results of this pilot study must be viewed in terms of several limitations. The study was conducted at one clinical site. At the time of the study, the Bedsider website was in English only, thereby excluding women who were not English proficient. Likewise, in order to complete the questionnaires, participants needed to be proficient in reading English, another limitation. The final sample was small, and included only women aged 18-29 years. Also, only 57% of the participants returned for 6-week follow-up measures.
Additional recruitment difficulties revolved around the weather and the political climate at the time. In January and February 2015, the northeastern Massachusetts region of the country received historic snowfall amounts, resulting in multiple canceled clinic sessions and transportation challenges that extended into March. Most women who attended the study clinic were of Hispanic descent; some were also undocumented. In addition to the language barrier, some of these women may have been reluctant to participate in the study because of the heated rhetoric regarding Hispanic and Mexican immigrants that was dominating the media at the time.
The ensuing sample characteristics and limited follow-up data restricted generalizability beyond this sample. In addition, as with all self-report measures, issues of social desirability must be considered.
Despite these limitations, important insights were gained. The clinic that served as the research site provides low-cost healthcare, quick-start contraception, and flexible, open-access scheduling. Even with removal of access and cost barriers and the liberal policies for starting the contraceptive methods, women who enrolled in the study reported low levels of contraceptive use. The reasons for this low level of use are unclear. However, NP counseling, with or without the addition of technology, increased LARC use and overall use of contraception.
Conclusion
Providers of today encounter complex and challenging health problems within a multicultural and multilingual patient population. In this environment, patient education can be challenging. Given the move toward greater patient involvement in the healthcare decision-making process, technology-based decisional-aid tools offer an effective and acceptable adjunct for patient health education. The women who participated in this study were receptive to using the Bedsider website as an adjunct to contraceptive counseling with the NP. Participants easily navigated the webpages and did not encounter technology-related problems. Although LARC use did not differ significantly between women who received traditional face-to-face contraceptive counseling and those who received technology-enhanced counseling, the use of online/digital media to enhance contraceptive counseling was both feasible and acceptable to patients. Practice settings should consider novel ways to deliver and reinforce contraceptive teaching that will help women choose the most effective method that reflects their individual needs.
Heidi Collins Fantasia is Assistant Professor at the University of Massachusetts Lowell College of Health Sciences, School of Nursing, in Lowell, Massachusetts. Allyssa L. Harris and Holly B. Fontenot are Assistant Professors at Boston College, William F. Connell School of Nursing, in Chestnut Hill, Massachusetts. All authors practice clinically as women’s health nurse practitioners. The authors state that they do not have a financial interest in or other relationship with any commercial product named in this article.
Funding
This study was funded by a grant from Bedsider awarded to Dr. Fantasia and Health Quarters, Inc.
Acknowledgment
The authors thank the staff and patients of Health Quarters, Inc., who graciously agreed to take part in this study.
References
- Finer LB, Zolna MR. Unintended pregnancy in the United States: incidence and disparities, 2006. Contraception. 2011;84(5):478-485.
- Finer LB, Henshaw SK. Disparities in rates of unintended pregnancy in the United States, 1994 and 2001. Perspect Sex Reprod Health. 2006;38(2):90-96.
- Frost JJ, Lindberg LD, Finer LB. Young adults’ contraceptive knowledge, norms and attitudes: associations with risk of unintended pregnancy. Perspect Sex Reprod Health. 2012;44(2):107-116.
- Zolna M. Lindberg L. Unintended Pregnancy: Incidence and Outcomes Among Young Adult Unmarried Women in the United States, 2001 and 2008. New York, NY: Guttmacher Institute; 2012.
- CDC. U.S. selected practice recommendations for contraceptive use, 2016. MMWR Recomm Rep. 2016;65(4):1-66.
- CDC. Providing quality family planning services: recommendations of CDC and U.S. Office of Population Affairs. MMWR. 2014;63(4):1-54.
- Lotke PS. Increasing use of long-acting reversible contraception to decrease unplanned pregnancy. Obstet Gynecol Clin N Am. 2015;42(4):557-567.
- Speidel JJ, Harper CC, Shields WC. The potential of long-acting reversible contraception to decrease unintended pregnancy. Contraception. 2008;78(3):197-200.
- Frost JJ, Darroch JE. Factors associated with contraceptive choice and inconsistent method use, United States, 2004. Perspect Sex Reprod Health. 2008;40(2):94-104.
- Trussell J, Henry N, Hassan F, et al. Burden of unintended pregnancy in the United States: potential savings with increased use of long-acting reversible contraception. Contraception. 2013;87(2):154-161.
- Parks C, Peipert JF. Eliminating health disparities in unintended pregnancy with long-acting reversible contraception. Am J Obstet Gynecol. 2016;214(6):681-688.
- Branum AM, Jones J. Trends in long-acting reversible contraception use among U.S. women aged 15-44. NCHS Data Brief. 2015;(188):1-8.
- Secura GM, Allsworth JE, Madden T, et al. The contraceptive CHOICE project: reducing barriers to long-acting reversible contraception. Am J Obstet Gynecol. 2010;203(2):115.e1-7.
- Eisenberg D, McNicholas C, Peipert JF. Cost as a barrier to long-acting reversible contraceptive (LARC) use in adolescents. J Adolesc Health. 2013;52(4 suppl):S59-S63.
- Biggs MA, Arons A, Turner R, et al. Same-day LARC insertion attitudes and practices. Contraception. 2013;88(5):629-635.
- Thompson KMJ, Rocca CH, Kohn JE, et al. Public finding for contraception, provider training, and use of highly effective contraceptives: a cluster randomized trial. Am J Public Health. 2016;106:541-546.
- Fox MP. A systematic review of the literature reporting on studies that examined the impact of interactive, computer-based patient education programs. Patient Educ Couns. 2009;77(1):6-13.
- Wofford JL, Smith ED, Miller DP. The multimedia computer for office-based patient education: a systematic review. Patient Educ Couns. 2005;59(2):148-157.
- Evans AE, Edmundson-Drane EW, Harris KK. Computer-assisted instruction: an effective instructional method for HIV prevention education? J Adolesc Health. 2000;26(4):244-251.
- Homer C, Susskind O, Alpert HR, et al. An evaluation of an innovative multimedia educational software program for asthma management: report of a randomized, controlled trial. Pediatrics. 2000;106(1 pt 2):210-215.
- Martin JT, Hoffman MK, Kaminski PF. NPs vs. IT for effective colposcopy patient education. Nurse Pract. 2005;30(4):52 -57.
- Shaw MJ, Beebe TJ, Tomshine PA, et al. A randomized, controlled trial of interactive, multimedia software for patient colonoscopy education. J Clin Gastroenterol. 2001;32(2):142-147.
- Bedsider website. 2015.
- Groves RM, Mosher WD, Lepkowski J, Kirgis NG. Planning and development of the continuous National Survey of Family Growth. National Center for Vital Health Statistics. Vital Health Stat 1. 2009;(48):1-64.
- CDC. Sexual and reproductive health of persons aged 10-24 years – United States, 2002- 2007. MMWR Surveill Summ. 2009;58(6):1-58.
- Strasburger VC, Brown SS. Sex education in the 21st century. JAMA. 2014;312(2):125-126.
- Gressel GM, Lundsberg LS, Illuzzi JL, et al. Patient and provider perspectives on Bedsider.org, an online contraceptive information tool, in a low income, racially diverse clinic population. Contraception. 2014;90(6):588-593.
- Wyatt KD, Anderson RT, Creedon D, et al. Women’s values in contraceptive choice: a systematic review of relevant attributes included in decision aids. BMC Women’s Health. 2014;14(1):1-13.
- Antonishak J, Kaye K, Swiader L. Impact of an online birth control support network on unintended pregnancy. Soc Market Q. 2015;21(1):23-36.