
Pelvic floor health contributes to optimal urinary, bowel, and sexual function. The pelvic floor muscles act like a hammock that runs between the anterior (pubic bone) and posterior (coccyx) aspects of the pelvic girdle. Pelvic floor muscle tone can be categorized as normal tone, high tone/hypertonic, or low tone/hypotonic. Hypertonic pelvic floor muscles occur from increased stress when the muscles are in spasm or in a constant state of contraction. This constant muscle tension locally decreases blood circulation and exchange of oxygen and metabolites, which can lead to the formation of myofascial trigger points (MTrPs) or hypersensitive areas.1 The causes of hypertonic pelvic floor muscles are multifactorial and can include: injury or trauma, musculoskeletal dysfunction (from poor posture, prolonged sitting, gait abnormalities, pelvic misalignment), poor breathing mechanics, frequent holding of urine and/or stool, physical or sexual abuse, stress, and pain causing conditions.1–3 When assessed vaginally or rectally, these hypertonic muscles are typically hypersensitive and patient symptoms may be reproduced.3
Pelvic floor motor control is defined by pelvic floor muscles that can both contract and release.3 Pelvic floor muscle tone and motor control are assessed with a focused health history and targeted vaginal or rectal examination. Conducting a skilled pelvic floor assessment can inform specific relief strategies in cases of hypertonicity, facilitate patient education and reassurance, and guide referrals to pelvic health or other specialists as needed for further evaluation and management. This article provides a review of pelvic floor anatomy and function, an explanation of how high tone pelvic floor muscles correlate to urinary, bowel, and sexual dysfunction, guidance on how to assess for high tone pelvic floor dysfunction, and suggestions for patient education.
Pelvic floor anatomy and function
Pelvic floor muscles are like any other muscle in the body, except they are internal muscles that can only be palpated and assessed by a vaginal or rectal exam (Figure 1, Figure 2). Because the pelvic floor muscles are internal muscles, they are often overlooked. Although nurse practitioners (NPs) learn head-to-toe musculoskeletal assessment, not all receive education about pelvic floor muscle assessment, which includes assessment of pelvic floor motor control and muscle tone.4,5 Pelvic floor musculature is still not a required educational component for physical therapists who are musculoskeletal specialists. Additional training is required outside of physical therapy school to be a pelvic floor physical therapist. The NP also may obtain additional training to specialize in the diagnosis and management of pelvic floor dysfunction.
Figure 1. Pelvic floor muscles
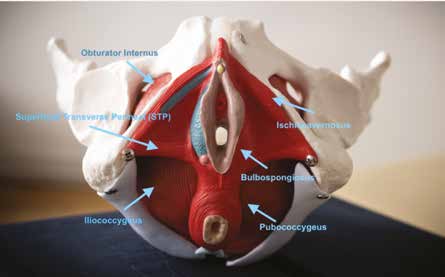
The pelvic floor muscles maintain continence (urinary and fecal), support the viscera, and aid in sexual appreciation. Numerous urinary, bowel, sexual, and other pelvic floor muscle dysfunction conditions may have an underlying hypertonic pelvic floor etiology. See the Table for a comprehensive, though not exhaustive list. Hypertonicity of the pelvic floor can be an etiology of urinary urgency, frequency, and burning, all symptoms that mimic a urinary tract infection (UTI).4 Tight pelvic floor muscles can create constipation. Insertional and deep dyspareunia often have an underlying hypertonic pelvic floor muscle etiology.1 Assessing the pelvic floor muscles and motor control will help guide differential diagnoses and better inform the patient on their unique plan of care. Attention to pelvic health can alleviate a wide range of patient conditions.
Rationale for pelvic floor assessment
It can be complex to determine the cause of urinary, bowel, and sexual dysfunction symptoms, especially when they are chronic or recurrent. Many patients with such symptoms will present with a laundry list of tests they have had performed to rule out different diagnoses. Some of that information is helpful, but a basic pelvic health workup could provide the same information. A simple assessment includes questions such as “What does your pelvic floor feel like when I press this muscle?,” “Does my palpation reproduce your symptoms?,” “Do you feel your pelvic floor muscles relax when you bear down or do you feel your pelvic floor muscles contract when you bear down?,” and provides crucial information for what to do next.
When these muscles are hypertonic or dysfunctional, the pain pattern differs from other musculoskeletal conditions.1,3 For example, when a person’s neck is sore, they might experience tension throughout the neck and say that it aches and will try to stretch it out. They also may have specific tender spots or MTrPs within that neck tension and they may apply gentle pressure directly to the tender spots. But when a person’s pelvic floor is tight or hypertonic with MTrPs, it can create both functional and vasomotor symptoms such as discharge, rash, and burning pain.1 Understanding the complexity of the conditions listed in the Table (many causing chronic or recurrent pelvic pain), the importance of assessing for hypertonic pelvic floor muscles, and the attention to relieving this hypertonicity as part of treatment are key.
Table. Urinary, bowel, sexual health diagnoses that may have underlying hypertonic pelvic floor etiology1–3,5
- Urinary frequency
- Urinary urgency
- Dysuria
- Lower urinary tract symptoms
- Interstitial cystitis/bladder pain syndrome
- Anismus
- Constipation
- Irritable bowel syndrome
- Chronic pelvic pain
- Dyspareunia
- Pelvic and perineal pain
- Vaginismus
- Vulvodynia
High tone pelvic floor and urinary dysfunction
The urogenital muscles of the pelvic floor are a collection of superficial muscles that support the urethra and the bladder.1,3,5 The compressor urethrae is a muscle that wraps around the urethra. The urogenital muscles of the pelvic floor and compressor urethrae are surrounded by connective tissue called fascia.1,3 The connective tissue can become irritated and restricted (tight). As a result, the muscles can become hypertonic with MTrPs, which can impact the ability of the bladder to empty fully and obstruct urinary flow.4,6 Consider this scenario: A patient with a history of recurrent UTIs presents with burning with urination and no other systemic symptoms (no fever, costovertebral angle tenderness, or flank pain). If the urinalysis or urine culture is positive, the appropriate antibiotic would be prescribed. If the urine studies are negative, what is the next step? Out of frustration and not knowing what else to offer, the NP may prescribe another round of antibiotics. In this situation, what else can the NP do?
Here is where the pelvic floor should be considered. Inflammation and infection can create pelvic floor muscle dysfunction, especially if the patient has had recurrent diagnosed UTIs.1,3,4 Hypertonic pelvic floor muscles are a common cause of dysfunctional voiding including dysuria, urinary urgency, and frequency.4,6 Palpation of the pubococcygeus muscle at the posterior aspect of the pubic bone or gently moving the compressor urethrae will often reproduce the burning or irritation symptoms the patient is experiencing with urination if they have pelvic floor muscle dysfunction (Figure 2). Reproducing these symptoms on either or both of these muscles along with a feeling of tension or palpation of an MTrP underneath the examining finger could indicate a musculoskeletal and connective tissue component to the patient’s urinary complaints.1,3,4
To assess the compressor urethrae, insert the index finger to the proximal interphalangeal joint and direct it upward along the anterior vaginal wall, between 1 and 11 o’clock on either side of the urethra. To assess the pubococcygeus, insert the index finger to the metacarpophalangeal (MCP) joint, turn the finger up to the pubic bone, and palpate the anterior muscle fibers at the attachment on the pubic bone on either side of the urethra, between 5 and 7 o’clock on the pelvic clock. Turn the finger so the finger pad is pointing to the coccyx and palpate the posterior muscle fibers at 4 and 8 o’clock (Figure 2).5
Figure 2. The internal pelvic floor muscles
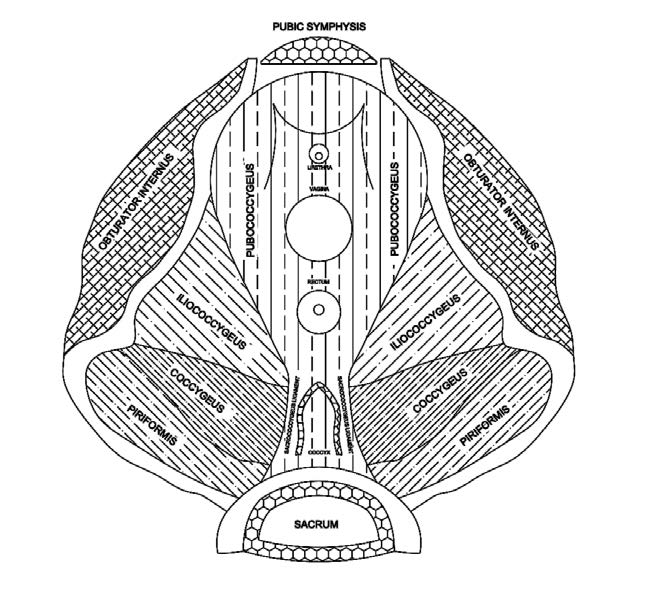
Hypertonicity of the pelvic floor muscles can compress or irritate the pudendal nerve. The pudendal nerve is the main pelvic floor nerve, innervates from S2 to S4, and goes through the pudendal (or Alcock’s) canal and through many pelvic floor muscles. Compression can create burning neuropathic pain, urinary urgency, frequency, and dysuria, all the hallmark symptoms of a UTI.1,3,4 To assess for pudendal nerve compression or irritation, insert the entire index finger to the MCP joint into the vaginal canal at midline and turn the index finger and wrist toward the hip. Place the other hand externally on the patient’s outer thigh and perform resisted hip external rotation. This will cause the obturator internus muscle to contract under your finger and may reproduce the patient’s burning pelvic pain (Figure 1, Figure 2).1,3
When MTrPs are identified, the NP can perform gentle trigger point release by applying gentle pressure to the pubococcygeus muscle, obturator internus muscle, or the compressor urethrae muscle with the examining finger. Gentle cross friction massage along the urethra can also be provided. These techniques help to break up some of the myofascial tightness and will bring blood flow to the area to create more mobility of the muscle. The NP can instruct the patient on three-dimensional diaphragmatic breathing to promote relaxation of pelvic floor muscles. Teach the patient to place their hands on their rib cage, gently breathing in and feeling the three-dimensional expansion of the rib cage, followed by a pause, and then breathing out, repeating this at least 10 times daily.7 There are home devices that the NP can prescribe. These include vaginal dilators, a pelvic wand, and a vibrator. There are no standard treatment protocols and each patient response is unique, but there is evidence to support the use of these devices for a reduction in pelvic floor muscle hypertonicity and to aid in releasing MTrPs.2 Vaginal dilators can be prescribed for daily use for desensitization and stretching of the pelvic floor muscles to aid in reducing hypertonicity.2,3,8 A pelvic wand to massage MTrP, twice weekly for 5 weeks, has been shown to reduce symptoms and can aid in releasing MTrPs.1–3,7,8
There is emerging evidence for the therapeutic use of vibrators given that vibration promotes vasodilation and blood flow to hypertonic pelvic floor muscles, leading to decreased hypertonicity of the pelvic floor muscles. In vulvodynia patients, the use of a vibrator for 5 to 10 min/day over 4 to 6 weeks has been shown to reduce pelvic floor hypertonicity.9 Follow-up for reassessment of symptoms and reinforcement of the use of self-management strategies is important. The exact treatment protocols vary and more well-designed trials are needed.2 If alleviation of patient symptoms is not obtained with self-management strategies, referral to a pelvic floor specialist should be considered.
High tone pelvic floor and bowel dysfunction
Chronic or recurrent constipation represents a common bowel dysfunction with a potential etiology of high tone pelvic floor. Typically, clinicians will suggest a fiber supplement, educate about increasing dietary fiber, and if that does not work, may prescribe a laxative. If none of that works, they will often refer to a gastroenterologist. Before making a referral, consider that the constipation may be caused by pelvic floor dysfunction.3,5 From a mechanical standpoint, as the rectal tissue is contracting and stool is eliminated, the pelvic floor muscles need to lengthen and soften, allowing for stool to pass.3 There can be dysfunction with a specific muscle called the puborectalis muscle that wraps around the rectum. When an individual sits all day at a computer, they tuck their tailbone under and the tailbone gets pulled toward the pubic bone, shortening the whole pelvic floor. This causes increased tension of the puborectalis muscle. The puborectalis is medial to and cannot be differentiated from fibers of the pubococcygeus. When the puborectalis gets shortened or tight, it will not be able to descend or relax around the rectum when the patient tries to have a bowel movement.1
This mechanical dysfunction of the pelvic floor muscles will cause the person to get Bristol stool type 1 with a pebble-like stool or Bristol stool type 2 that is thin and ribbon-like.10 During the assessment, show patients the Bristol stool chart and have them point to what their stool looks like. Some patients will think that Bristol 2 (ribbon-like) stool is normal, but ribbon-like stool means that the puborectalis muscle is not relaxing or softening as much as it should and that is why the stool is so thin. Ask the patient, “When you have a bowel movement, do you completely empty? How are you bearing down?”
For patients with chronic or recurrent constipation, a pelvic examination may be informative. Before doing a bimanual exam, ask the patient to bear down and look at what happens externally to the perineal body. Does the perineal body elongate with Valsalva? If the perineal body elongates, the patient has appropriate pelvic floor motor control. Or does the perineal body shorten? The shortening of the perineal body with Valsalva is called a paradoxical contraction.1,3,11 This is inappropriate pelvic floor motor control. Many patients with constipation have a paradoxical contraction.1 The muscle needs to start to relax and the perineal body to elongate when there is the urge to have a bowel movement. Mechanically, what is happening for patients with a paradoxical contraction is the exact opposite. That makes it difficult to pass stool and might result in Bristol 1 or 2 type stools rather than a Bristol 3 or 4.10
Observe what the abdominal area is doing when the patient bears down. Is there visible tightening of the abdominal muscles? Simply cueing patients to take a couple of diaphragmatic breaths during the exam will help initiate the relaxation of those muscles, making the exam more comfortable.
Pelvic floor motor control, specifically of the pubococcygeus and puborectalis muscles, can be assessed vaginally or rectally as well. Insert a gloved index finger into the vaginal introitus and ask the patient to bear down. With Valsalva, appropriate pelvic floor motor control will feel like there is space created around your index finger as the pelvic floor muscles lengthen and soften. If you feel the pelvic floor muscles squeezing or tightening around your index finger with Valsalva, this is a paradoxical contraction.1
When paradoxical contraction is identified, the NP can perform a gentle trigger point release or apply gentle pressure to the pubococcygeus muscle to improve blood flow and mobility of the muscle. Instruct the patient on the use of diaphragmatic breathing with bowel movements to allow both the abdominal muscles and pelvic floor muscles to relax.7,12 Provide education on appropriate toileting position. Proper toileting position with the knees, higher than the hips, promotes the proper anorectal angle, promoting ease of passing stool.1 Prescribe devices (dilators and pelvic wand) as discussed.2,9,13 Encourage follow-up for reassessment of symptoms and reinforcement of self-management strategies.
High tone pelvic floor and sexual dysfunction
Pain with penetrative sexual activity is a commonly encountered sexual dysfunction that may have high tone pelvic floor as an etiology. Always use a trauma-informed lens and tailor history taking and exam appropriately when a patient presents with painful penetrative sex concerns.13 It can be helpful to ask specific questions: “Do you have pain with initial penetration, and what does that feel like, what is the sensation like? Is it burning? Is it sharp? Is it stabbing? What is the quality?” Ask the same questions about deeper penetration. Ask the patient, “Do you use lubricant during sexual activity? And if so, how are you applying it?” Asking the right questions will help determine the problem area and help the patient feel more comfortable and validate their experience of having sexual pain. Many people with sexual pain believe they have done something wrong. They feel that it is all in their head or that it is their fault, with much associated shame. Asking these questions and listening to the answers provides the opportunity to educate patients that their symptoms may have an underlying mechanical etiology.1,3 “The muscles are tight. You are trying to insert something into an area with tight muscles, so that could be part of the reason why it hurts.” If they are having a lot of pain with initial penetration, is it something that happens right away? Is it a burning pain that occurs as soon as there is penetration, or is it a burning pain that happens after a couple of minutes? Does the burning increase with time? If the burning pain happens right away on penetration, it is probably due to tight pelvic floor muscles. Again, pelvic floor tightness/hypertonicity can create burning pain.3
An essential first step in the pelvic examination when a patient has pain with initial penetration is the Q-tip test. Picture the vaginal opening like a clock. For example, 12 o’clock is the clitoris/urethra and 6 o’clock is the bottom of the vaginal opening (Figure 1). Start at the perineal body, begin at 6 o’clock, directly on the vulvar vestibule, and gently palpate to see the patient’s response and make note of any tenderness. Ideally, the test needs to be performed a couple of times to ensure that it is accurate. If patients have sensitivity between 5 o’clock and 7 o’clock, this may indicate hypertonic pelvic floor muscles. That is where all the pelvic floor muscles interconnect and attach to the central tendon area. This assessment provides information that can be used to locate muscles of concern during the vaginal or rectal exam. Before an intravaginal exam, note any external dryness or erythema of the vulva, labia majora, labia minora, and vestibule. Dry or thin tissue externally or internally could contribute to a patient’s sexual pain symptoms.14,15 The deep pelvic floor muscles known as the levator ani muscles include the pubococcygeus, iliococcygeus, and coccygeus and are innervated by the pudendal nerve S2, S3, S4. To assess these muscles for MTrPs, insert the entire index finger into the vaginal canal at midline to the MCP joint, noting tension or hypersensitivity under your finger bilaterally on the pubococcygeus, iliococcygeus, and coccygeus. These three muscles are illustrated in Figure 2.
Consider performing gentle trigger point release or applying gentle pressure to any of the hypertonic levator ani muscle group for reasons previously stated. Provide education on correct use of lubricant, that is, apply lubricant inside of the vagina and apply on whatever is going inside of the vagina. Lubricants with high osmolality (> 1,200 mOsm/kg per World Health Organization) can dry out the vulvovaginal tissues.16 The NP can encourage the patient to visit the lubricant company website to obtain the osmolality, as well as instruct the patient on diaphragmatic breathing prior to penetrative activity, allowing both the abdominal muscles and pelvic floor muscles to relax.7,12 Consider mindfulness-based stress reduction techniques.17 Prescribe devices (vaginal dilators, pelvic wand, vibrators).9 Encourage follow-up for reassessment of symptoms and reinforcement of education.
Pelvic health specialist
NPs and physical therapists with specific training can offer services as a pelvic health specialist. Training is available through workshops and courses. For management and long-term alleviation of hypertonic pelvic floor, the pelvic health specialist helps the patient to become aware of the pelvic floor muscles and improves the mind-body connection to the pelvic floor. They do this through extensive hands on treatment (externally and intravaginally or intrarectally), through various manual techniques to release myofascial restrictions that are causing external pelvic misalignment and internal hypertonicity of the pelvic floor muscles.2,18 While working intravaginally or intrarectally, the index finger of the specialist acts as biofeedback to improve pelvic floor motor control.11 The goal is to promote relaxation of the pelvic floor muscles, to improve pelvic floor motor control and for the patient to have a home maintenance program to prevent recurrence of symptoms. Each patient is unique. Some patients will respond quickly and can be discharged from care after 8 to 12 sessions, whereas others will need weekly treatment for months or even years.2
Implications for practice
The pelvic floor muscles play a pivotal role in women’s health, and many common health conditions are caused by pelvic floor dysfunction. The diagnoses listed in the Table are multifactorial and complex. Although other attention and treatment is likely needed for some of these conditions, attention to hypertonic pelvic floor muscles should be included to provide comprehensive care that will benefit the patient. The NP can use pelvic floor muscle assessment skills, implement some simple strategies for relief of symptoms when high muscle tone is discovered, and educate patients to enhance their own empowerment in managing pelvic health. This assessment also facilitates appropriate referrals to pelvic floor or other specialists when additional evaluation and management are needed. A multidisciplinary team approach that allows for an individualized and comprehensive plan of care is of most benefit to the patient.
Kathy Kates and Melissa Hines are cofounders of the Institute for Pelvic Health in Boston, Massachusetts. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(5):30-36. doi: 10.51256/ WHC102330
References
1 Tim S, Mazur-Bialy AI. The most common functional disorders and factors affecting female pelvic floor. Life (Basel). 2021;11(12):1397.
2 Wallace SL, Miller LD, Mishra K. Pelvic floor physical therapy in the treatment of pelvic floor dysfunction in women. Curr Opin Obstet Gynecol. 2019;31(6):485-493.
3 Shrikhande A, Ullger C, Seko K, et al. A physiatrist’s understanding and application of the current literature on chronic pelvic pain: a narrative review. Pain Rep. 2021;6(3):e949.
4 Scharp D. Hypertonic pelvic floor muscle dysfunction and urinary tract infection: a comprehensive approach to diagnosis and treatment. Urologic
Nursing. 2020;40(5):225-255.
5 Meister MR, Shivakumar N, Sutcliffe S, et al. Physical examination techniques for the assessment of pelvic floor myofascial pain: a systematic review. Am J Obstet Gynecol. 2018;219(5):497.e1-497.e13.
6 Clothier JC, Wright AJ. Dysfunctional voiding: the importance of non-invasive urodynamics in diagnosis and treatment. Pediatr Nephrol. 2018;33(3):381-394.
7 Talasz H, Kremser C, Talasz HJ, et al. Breathing, (S)training and the pelvic floor–A basic concept. Healthcare (Basel). 2022;10(6):1035.
8 Berghmans B. Physiotherapy for pelvic pain and female sexual dysfunction: an untapped resource. Int Urogynecol J. 2018;29(5):631-638.
9 Dubinskaya A, Horwitz R, Scott V, et al. Is it time for doctors to Rx vibrators? A systematic review of pelvic floor outcomes. Sex Med Rev. 2023;11(1):15-22.
10 Bordeianou LG, Anger JT, Boutros M, et al. Measuring pelvic floor disorder symptoms using patient-reported instruments: Proceedings of the consensus meeting of the Pelvic Floor Consortium of the American Society of Colon and Rectal Surgeons, the International Continence Society, the American Urogynecologic Society, and the Society of Urodynamics, Female Pelvic Medicine and Urogenital Reconstruction. Dis Colon Rectum. 2020;63(1):6-23.
11 Ghaderi F, Bastani P, Hajebrahimi S, et al. Pelvic floor rehabilitation in the treatment of women with dyspareunia: a randomized controlled clinical trial. Int Urogynecol J. 2019;30(11):1849-1855.
12 Bonis M, Lormand J, Walsh C. Immediate effects of exercise and behavioral interventions for pelvic floor dysfunction and lumbopelvic pain. J Womens Health Phys Ther. 2020;44(2):54-62.
13 Ross V, Detterman C, Hallisey A. Myofascial pelvic pain: an overlooked and treatable cause of chronic pelvic pain. J Midwifery Womens Health. 2021;66(2):148-160.
14 Potter N, Panay N. Vaginal lubricants and moisturizers: a review into use, efficacy, and safety. Climacteric. 2021;24(1):19-24.
15 Waetjen LE, Crawford SL, Chang P-Y, et al; Study of Women’s Health Across the Nation (SWAN). Factors associated with developing vaginal dryness symptoms in women transitioning through menopause: a longitudinal study. Menopause. 2018;25(10):1094-1104.
16 Shelby RA, Coleman JN, Arthur SS, et al. Sexual and reproductive health concerns. In: Kimmick GG, Shelby RA, Sutton LM, eds. Common Issues in Breast Cancer Survivors: A Practical Guide to Evaluation and Management. Springer Cham; 2021:47-84.
17 Brotto LA, Bergeron S, Zdaniuk B, et al. A comparison of mindfulness-based cognitive therapy vs cognitive behavioral therapy for the treatment of provoked vestibulodynia in a hospital clinic setting. J Sex Med. 2019;16(6):909-923.
18 Bonnema R, McNamara M, Harsh J, Hopkins E. Primary care management of chronic pelvic pain in women. Cleve Clin J Med. 2018;85(3):215-223.
KEY WORDS: pelvic health, pelvic floor muscles, hypertonic pelvic floor muscles, recurrent urinary tract infections, constipation, dyspareunia