
Faculty: Antay L. Parker, DNP, APRN, WHNP-BC, CNM, CRNFA, C-EFM, is Assistant Professor of Nursing at East Texas Baptist University in Marshall, Texas, and an OB triage advanced practice provider with the Acclaim Physician Group at JPS Health Network in Fort Worth, Texas.
Continuing education approval: This activity has been evaluated and approved by the Continuing Education Approval Program of the National Association of Nurse Practitioners in Women’s Health (NPWH) for 1.0 continuing education contact hours now through August 31, 2024.
Educational objectives: At the conclusion of this educational activity, participants should be able to:
- Identify the components of initial assessment of the pregnant individual with first-trimester bleeding.
- Discuss recommended management for threatened and actual early pregnancy loss.
- Discuss recommended management for ectopic pregnancy.
Antay L. Parker, DNP, APRN, WHNP-BC, CNM, CRNFA, C-EFM, has no actual or potential conflicts of interest in relation to this article.
Disclaimer: Participating faculty members determine the editorial content of the CE activity; this content does not necessarily represent the views of NPWH. This content has undergone a blinded peer review process for validation of clinical content. Although every effort has been made to ensure that the information is accurate, clinicians are responsible for evaluating this information in relation to generally accepted standards of care and integrating the information in this activity with that of established recommendations of other authorities, national guidelines, and individual patient characteristics.
Commercial support: This activity did not receive any commercial support.
Successful completion of the activity: Successful completion of this activity, J-22-04, requires participants to do the following:
- “Sign in” at the top right-hand corner of the page. If you have an NPWH account. You must be signed in to receive credit for this course. If you do not remember your username or password, please follow the “Forgot Password” link and instructions on the sign-in page. If you do not have an account, please click on the “Create an Account.”*
- Read the learning objectives, disclosures, and disclaimers.
- Study the material in the learning activity during the approval period (now through August 31, 2024).
- Complete the post-test and evaluation. You must earn a score of 70% or higher on the post-test to receive CE credit.
- Print out the CE certificate after you have successfully passed the post-test and completed the evaluation.
*If you are an NPWH member, were once a member, or have completed CE activities with NPWH in the past, you have a username and password in our system. Please do not create a new account. Creation of multiple accounts could result in loss of CE credits as well as other NPWH services. If you do not remember your username or password, either click on the “Forgot Username” or “Forgot Password” link or call the NPWH office at (202) 543-9693, ext. 1.
Vaginal bleeding is one of the most common reasons for seeking care in early pregnancy. Nurse practitioners and midwives must be vigilant to conduct thorough assessment and management to provide exceptional care for patients experiencing vaginal bleeding in early pregnancy, particularly related to ruling out life-threatening conditions including obstetric hemorrhage and ectopic pregnancy. It is important to understand the diagnostic tools and treatment options available to appropriately counsel patients including expectant, medical, and surgical management of various conditions.
Vaginal bleeding occurs at all stages of pregnancy and is a common reason for patients to present for care in the first trimester (prior to 14 weeks’ gestation). Bleeding typically results from disruption of blood vessels in the decidua, cervical or vaginal lesions, trauma, or undiagnosed infections. The clinician makes provisional diagnoses based on gestational age, bleeding characteristics, and physical examination, with confirmation based on laboratory and/or imaging studies. This article reviews assessment, diagnosis, and management for urgent causes of bleeding in the first trimester.
Vaginal bleeding emergencies
Severity dictates the urgency and location of the evaluation of vaginal bleeding in early pregnancy. If the patient is hemodynamically unstable, supportive measures and treatment should be rapidly implemented, ideally in the emergency room or labor and delivery unit. Some patients will have a massive blood loss prior to showing signs of hemodynamic instability and must be managed appropriately.
Validated obstetric triage acuity tools, such as the Association of Women’s Health, Obstetric and Neonatal Nurses’ Maternal-Fetal Triage Index, may improve efficiency and quality of care by providing a standardized approach to obstetric triage.1 This five-level acuity tool for nurses allows for the prioritization of provider evaluation based on presenting complaints, vital signs, fetal heart tones by Doppler (if applicable), and medication history, ultimately allowing for improved team communication and outcomes. Typically, obstetric triage volume exceeds overall birth volumes in a given hospital by 20% to 50%.2 Keeping in mind that a pregnant person could present at any institution providing emergency care, appropriate screening and disposition tools should be in place.
Assessment
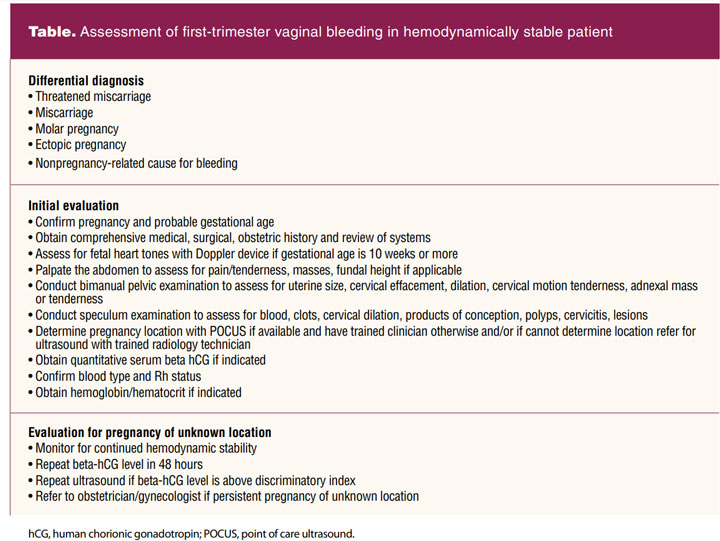
Initial assessment of vaginal bleeding in early pregnancy consists of pregnancy confirmation and determining the location of the pregnancy and hemodynamic status. Although the goal of evaluation of first-trimester bleeding remains a definitive diagnosis, this is not always possible. Exclusion of serious complications should be the top management priority—particularly ectopic pregnancy. If the patient has not had a pelvic ultrasound, a transvaginal ultrasound is the gold standard of evaluation.3 Prior ultrasound confirming an intrauterine pregnancy narrows the differential diagnosis, but it does not necessarily exclude the rare yet possible heterotopic pregnancy, that is, occurrence of both an intrauterine and ectopic pregnancy.
A comprehensive medical, surgical, and obstetric history also provides valuable insight into the potential cause of first-trimester bleeding. The clinician should be especially alert to risk factors for ectopic pregnancy including, but not limited to, previous ectopic pregnancy, history of sexually transmitted infections, history of pelvic inflammatory disease, or previous fallopian tube surgery such as tubal ligation reversal/tubal reanastamosis.4 Thorough review of systems and physical assessment, including speculum examination, should be initiated to determine the extent of bleeding, possible source (ie, uterine vs cervical vs vaginal), and systemic involvement (ie, lightheadedness, dizziness, pelvic pain, nausea/vomiting).
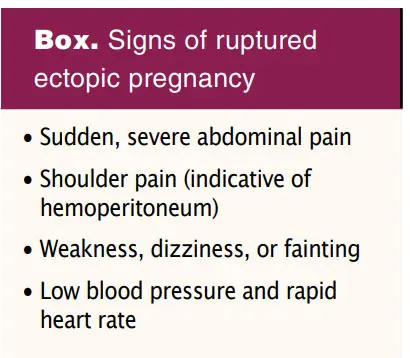
In patients presenting with abdominal or pelvic pain in conjunction with vaginal bleeding, an urgent cause should be considered. Abdominal examination should be performed prior to pelvic examination. Midline pelvic or suprapubic pain is more consistent with early pregnancy loss, whereas unilateral pain is more consistent with ectopic pregnancy. Shoulder pain also may accompany ectopic pregnancy, particularly if ruptured. However, it is important to remember that painless vaginal bleeding does not exclude the possibility of a life-threatening complication, including ectopic pregnancy. Any tissue passed by the patient or removed by the provider during a pelvic examination should be carefully examined as blood clots may be mistaken for products of conception. If the pregnancy is at least 10 to 12 weeks’ gestation, a handheld Doppler may be used to auscultate fetal heart tones for reassurance. Inability to auscultate fetal heart tones by Doppler in the first trimester is not necessarily diagnostic.
Diagnosis
The exact etiology of first-trimester vaginal bleeding often cannot be determined despite careful evaluation. Differential diagnoses for consideration should include ectopic pregnancy; threatened abortion; early pregnancy loss; cervical, vaginal, or uterine pathology (ie, polyps, infection, gestational trophoblastic disease); implantation bleeding; and trauma. See the Table for an outline of assessment of a hemodynamically stable patient with first-trimester bleeding. Most common nontraumatic causes of first-trimester bleeding include threatened abortion and early pregnancy loss, accounting for 10% of all clinically recognized pregnancies.5 Approximately 80% of all pregnancy losses will occur in the first trimester.
Threatened early pregnancy loss may include a wide variety of presentations, but it is typically characterized by vaginal bleeding and/or abdominal pain while an intrauterine pregnancy remains intact. Early pregnancy loss is defined as a nonviable, intrauterine pregnancy prior to 14 weeks’ gestation, with either an empty gestational sac or a gestational sac containing a fetal pole without cardiac activity.
Well-defined diagnostic guidelines for early pregnancy loss established by the Society of Radiologists provide strict discriminatory values for ultrasound visualization of a gestational sac, a yolk sac, an embryo, and cardiac activity.6 However, the clinician should always consider individual patient circumstances when interpreting ultrasound findings for diagnostic decision making.5 Point of care ultrasound (POCUS) may be utilized in time-critical situations by trained clinicians and may provide a cost-effective extension of the physical examination to confirm intrauterine pregnancy. POCUS should not be used as a replacement of formal ultrasound when a clear diagnosis cannot be made, intrauterine pregnancy cannot be confirmed, or when a trained clinician is unavailable.
Serial quantitative beta-human chorionic gonadotropin (hCG) monitoring may be useful in determining viability as part of the diagnostic workup. A single beta-hCG level is not diagnostic of any particular pregnancy outcome.
Ectopic pregnancy is much less common. Nevertheless, a recent study indicates ectopic pregnancy accounts for approximately 12.3 per 1,000 live births, with rates on the rise in the United States.7 A clear etiology is unclear, and it remains the most serious cause of first-trimester bleeding. Higher rates are linked with increasing maternal age, although up to 50% have no identifiable risk factors.8,9 A ruptured ectopic pregnancy is a potentially life-threatening condition, thus ectopic pregnancy must be excluded through ultrasound confirmation of intrauterine pregnancy. Unfortunately, cases have been reported of ruptured ectopic pregnancy with a beta-hCG below the discriminatory zone, the hCG level at which one would expect to be able to see landmarks of an intrauterine pregnancy. It is imperative that beta-hCG levels and ultrasound findings are interpreted in conjunction with clinical findings.8 Ectopic pregnancies outside the adnexa are often overlooked given these are not classic presentations. Other locations to evaluate for potential ectopic pregnancy include the abdomen (including the retroperitoneal space), uterine cornua, cesarean scars, and cervix.
A pregnant person without a confirmed intrauterine or ectopic pregnancy is considered to have a “pregnancy of unknown location.” Ongoing efforts must be made to determine the location and status of the pregnancy, which can be done with serial beta-hCG trending and transvaginal ultrasound to confirm diagnosis.
Clinical management
Prevention of Rh D alloimmunization must be a priority and is often overlooked in nonviable pregnancies and with early pregnancy bleeding. Threatened early pregnancy loss, early pregnancy loss, ectopic pregnancy, molar pregnancy, and pregnancy termination are all potential sensitizing events. Any pregnant person experiencing first-trimester bleeding who is Rh D negative regardless of cause or pregnancy outcome should receive 50 μg anti-D immunoglobulin.5
Timely administration within 72 hours of the bleeding event is vital to prevent Rh D alloimmunization.10 The routine use of anti-D immunoglobulin has reduced the risk of alloimmunization in at-risk pregnancies from approximately 15% to 1%.11 Failure to prevent Rh D alloimmunization could lead to hemolytic disease of the newborn in future pregnancies.
Threatened early pregnancy loss
No effective interventions exist to prevent threatened early pregnancy loss from evolving to actual early pregnancy loss. Pelvic rest, uterine relaxants, and administration of beta hCG have not been proved to prevent early pregnancy loss. Bedrest should not be recommended. The use of progesterone supplementation in threatened early pregnancy loss remains controversial.5 Patient education should include potential outcomes, necessary follow-up, when to present for emergent evaluation and care, and emotional support, primarily that any outcome is no fault of the pregnant person.
Early pregnancy loss
Management of early pregnancy loss should be tailored to each patient and clinical circumstances. Available options include expectant, medical, and surgical management, each with their own risks and benefits and generally accepted by the medical community and public. Patients should be counseled on the risks, benefits, and safety of each option, but there is no known difference in long-term outcome based on any particular method.
Expectant management should be limited to the first trimester. With adequate time, expectant management is successful in approximately 80% of cases.11 Expectant management may be more effective in patients already experiencing bleeding and cramping. It is important to counsel the patient about experiencing moderate-to-heavy bleeding, when to go to the emergency room, options for pain management, as well as that surgery may be required if complete uterine evacuation is not achieved. Consider use of ibuprofen or another nonsteroidal anti-inflammatory drug for pain management during early pregnancy loss management. Opioids should not be routinely used given the overdose risk and low rates of effectiveness in this clinical scenario. Follow-up includes ultrasound to confirm complete passage of gestational tissue or serial beta-hCG trending if ultrasound is not available. No consensus exists in the literature related to endometrial thickness consistent with complete miscarriage. All discussed cutoffs are arbitrary and not evaluated to determine a best value.12
Medical management should be considered if the individual desires expedited uterine evacuation without surgical intervention as long as there is no evidence of infection, hemorrhage, severe anemia, or bleeding disorders. Misoprostol-based regimens have been extensively studied and are the most widely used method of medical management. The largest randomized controlled trial completed in the US to date showed complete expulsion by day 3 in 71% of women after misoprostol 800 μg vaginally. The success rate increased to 84% after a second dose.12 Multiple studies have demonstrated vaginal and sublingual misoprostol is more successful than oral dosing but sublingual dosing is associated with higher rates of diarrhea. Mifepristone 200 mg orally can also be given 24 hours prior to misoprostol to decrease the duration of bleeding, although studies have shown patients often experienced increased pain and it is not readily available in many facilities.13 As with expectant management, it is important to counsel patients that they will experience moderate-to-heavy bleeding (often heavier than menses), when to go to the emergency room, and options for pain management, as well as that surgery may be required if complete uterine evacuation is not achieved. Follow-up includes ultrasound to confirm complete passage of gestational tissue or serial beta-hCG trending if ultrasound is not available.
Surgical evacuation should be utilized on patient request after thorough counseling or in patients who are hemodynamically unstable, hemorrhaging, or have signs of infection. This is typically completed in the operating room with an electric suction device followed by sharp curettage. Although this does provide immediate process completion, the patient must understand the risks associated with the procedure and with general anesthesia.
One exceptionally underutilized tool in the management of early pregnancy loss is manual uterine aspiration (MUA), particularly in the emergency room setting. It provides an additional choice for individuals who desire surgical management but prefer to avoid general anesthesia. Patients may be provided with a paracervical block or IV sedation as needed in the emergency department. This also can be performed in the office with only a paracervical block. MUA devices can be either reusable or single use. The handheld suction device with a size-appropriate sterile cannula is introduced into the uterus through the cervix and contents evacuated with a rotating motion. Complete evacuation is typically confirmed by point of care ultrasound by a trained clinician. Integrating MUA in the emergency department has been shown to be both safe and effective as well as having the potential to reduce healthcare resource utilization while improving patient care. Many patients choose this option when available for convenience and ease of scheduling because coordination with the operating room is not required.14
Overall, serious complications are rare following early pregnancy loss treatment. Hemorrhage and infection can occur with all treatment modalities.3 As no approach has been proven clinically superior, patient preference should guide the treatment process.
Ectopic pregnancy
Unless a definitive ectopic pregnancy is identified, follow-up should be conducted to preclude unnecessary methotrexate exposure or surgery. When an ectopic pregnancy is identified, the patient should be referred immediately to an obstetrician-
gynecologist for treatment that may be either medical or surgical.
Intramuscular methotrexate, a folate antagonist that binds to the catalytic site of dihydrofolate reductase, interrupting the synthesis of purine nucleotides and amino acids and ultimately inhibiting DNA synthesis, remains the single available treatment for medical management of ectopic pregnancy. Three published protocols are currently in use in the US: single dose, two dose, and fixed multiple dose.4 As both relative and absolute contraindications for methotrexate therapy exist, careful evaluation must be completed. Comprehensive counseling should be provided related to risk of ectopic rupture and treatment failure. The patient should be instructed on signs of ectopic rupture and the need for immediate medical attention should these occur (Box).
Extensive patient teaching should be completed related to necessary dietary and medication adjustments to exclude any folate-containing items or use of nonsteroidal anti-inflammatory drugs that may decrease the efficacy of methotrexate. Acetaminophen is usually adequate to manage mild abdominal pain that may occur. Sun exposure should be limited to avoid the occurrence of methotrexate dermatitis. Serial beta-hCG trending must be followed to ensure complete resolution of ectopic pregnancy. The patient should be advised to avoid sexual intercourse and vigorous physical activity until beta-hCG levels are undetectable and to avoid pregnancy for 2 to 3 menstrual cycles.5
When surgical management is chosen or required, salpingectomy and salpingotomy are options. Salpingectomy is the preferred method when significant damage to the fallopian tube is present or there is significant bleeding. Randomized controlled trials comparing salpingectomy and salpingotomy found no statistically significant difference in rates of subsequent intrauterine pregnancy or recurrent ectopic pregnancy.15 Although medical management avoids the inherent risks of surgery and anesthesia, there is an overall lower success rate compared with surgical management. Medical management also requires longer surveillance to ensure resolution.4
Emotional support following early pregnancy loss
Emotional support following pregnancy loss, including ectopic pregnancy, is essential to the holistic care of the patient. Although often overlooked, especially in emergent situations, providing emotional support during and following pregnancy loss is imperative. Women and men alike have expressed dissatisfaction with the level of emotional support provided in hospital settings following miscarriage and describe a number of hospital-related factors as exacerbating to their levels of emotional distress. These hospital-related factors primarily relate to lack of privacy and delays related to diagnosis and treatment. The clinician should explain everything clearly in layman’s terms, not withhold information, provide privacy, and above all acknowledge the loss and associated pain.16
A grief counselor or a local support group also may be considered helpful. Adequate social support and strategies to strengthen one’s sense of control and self-efficacy can have a positive impact on psychosocial wellbeing of patients who have experienced pregnancy loss beyond medical management.17
Future fertility counseling
Ovulation may occur as soon as 2 weeks after miscarriage. Encouragement to be both physically and emotionally ready for pregnancy after miscarriage is vital. Contraception may be offered and provided if desired.
Generally, no fertility workup is recommended after a first or sporadic early pregnancy loss. The majority of sporadic early pregnancy losses result from chromosomal abnormalities.18 Additional evaluation with a reproductive endocrinology or maternal-fetal medicine specialist should be considered after a patient experiences a second consecutive early pregnancy loss.18
Available evidence does not suggest that the use of methotrexate in the treatment of ectopic pregnancy affects future fertility. In patients undergoing surgical treatment of ectopic pregnancy, there is no evidence of improved fertility by undergoing salpingotomy versus salpingectomy.4
Conclusion
Evaluation and management of first-trimester bleeding often presents challenges to the clinician. Nevertheless, knowledge of potential causes and the use of evidence-based guidelines and recommendations allow for confidence in the diagnostic and treatment process. Vaginal bleeding in early pregnancy can be anything from benign to life-threatening and should always be treated with urgency until a diagnosis is reached. Clinicians have a key role in providing emotional support for the patient during the diagnostic process and during all aspects of treatment.
References
- Ruhl C, Scheich B, Onokpise B, Bingham D. Content validity testing of the maternal fetal triage index. J Obstet Gynecol Neonatal Nurs. 2015;44(6):701-709.
- Association of Women’s Health, Obstetric, & Neonatal Nurses. Guidelines for professional registered nurse staffing for perinatal units executive summary. J Obstet Gynecol Neonatal Nurs. 2011;40(1):131-134.
- Casikar I. How to effectively diagnose ectopic pregnancy using ultrasound? Expert Rev Obstet Gynecol. 2013;8(6):493-495.
- American College of Obstetricians and Gynecologists. Practice bulletin no. 193: Tubal ectopic pregnancy. Obstet Gynecol. 2018;131(3):e91-e103.
- American College of Obstetricians and Gynecologists. Practice bulletin no. 200: Early pregnancy loss. Obstet Gynecol. 2018;132(5):e197-e207.
- Rogers SK, Chang C, DeBardeleben JT, Horrow MM. Normal and abnormal US findings in early first-trimester pregnancy: review of the Society of Radiologists in Ultrasound 2012 consensus panel recommendations. Radiographics. 2015;35(7):2135-2148.
- Mann LM, Kreisel K, Llata E, et al. Trends in ectopic pregnancy diagnoses in United States emergency departments, 2006-2013. Matern Child Health J. 2020;24(2):213-221.
- Surampudi K, Gundabattula SR. The role of serum beta hCG in early diagnosis and management strategy of ectopic pregnancy. J Clin Diagn Res. 2016;10(7):QC08-QC10.
- Creanga AA, Syverson C, Seed K, Callaghan WM. Pregnancy-related mortality in the United States, 2011-2013. Obstet Gynecol. 2017;130(2):366-373.
- de Hass M, Finning K, Massey E, Roberts DJ. Anti-D prophylaxis: past, present and future. Transfus Med. 2014;24(1):1-7.
- American College of Obstetricians and Gynecologists. Practice bulletin no. 181: Prevention of Rh D alloimmunization. Obstet Gynecol. 2017;130(2):e57-e70.
- Zhang J, Gilles JM, Barnhart K, et al; National Institute of Child Health Human Development (NICHD) Management of Early Pregnancy Failure Trial. A comparison of medical management with misoprostol and surgery management for early pregnancy failure. N Engl J Med. 2005;353(8):761-769.
- Roe AH, McAllister A, Flynn AN, et al. The effect of mifepristone pretreatment on bleeding and pain during medical management of early pregnancy loss. Contraception. 2021;104(4):432-436.
- Whittaker L, Pymar H, Liu X-Q. Manual uterine aspiration in the emergency department as a first line therapy for early pregnancy loss: a single-centre retrospective study. J Obstet Gynaecol Can. 2022;S1701-2163(22)00070-6. Online ahead of print.
- Cheng X, Tian X, Yan Z, et al. Comparison of the fertility outcome of salpingotomy and salpingectomy in women with tubal pregnancy: a systematic review and meta-analysis. PLoS One. 2016;11(3):e0152343.
- Galeotti M, Mitchell G, Tomlinson M, et al. Factors affecting the emotional wellbeing of women and men who experience miscarriage in hospital settings: a scoping review. BMC Pregnancy Childbirth. 2022;22(270).
- Iwanowicz-Palus G, Mroz M, Bien A. A quality of life, social support and self-efficacy in women after a miscarriage. Health Qual Life Outcomes. 2021;19(16).
- Practice Committee of the American Society for Reproductive Medicine. Evaluation and treatment of recurrent pregnancy loss: a committee opinion. Fertil Steril. 2012;98(5):1103-1111.
Web resource
Key words: vaginal bleeding, early pregnancy loss, miscarriage, ectopic pregnancy, threatened early pregnancy loss
Womens Healthcare. 2022;10(4):9-14,28. doi:10.51256/WHC082209