
Mental health disorders are common among adolescents, with anxiety and depression being the most frequently encountered. To reduce severity of illness and risk of lifelong implications, it is essential for women’s health nurse practitioners and other clinicians who provide adolescent primary care to be skilled at routine mental health screening and evaluation, and able to confidently manage findings. This article provides a brief overview of the prevalence of and risks for depression and anxiety among adolescents in the United States, evidence-based resources for patient evaluation, and management options for these common mental health conditions identified in primary care settings.
At least 1 in 5 youth experience a significant, diagnosable mental health condition in the United States.1 More than half of mental health problems begin by age 14 years and 75% begin by age 24.2,3 Unfortunately, the delay in treatment from symptom onset averages more than 10 years.3 In fact, only half of adolescents with mental health conditions obtain professional counseling or medical management.4 Generalized anxiety disorder (GAD) and depression are the most common mental illnesses experienced by youth, with a significant number of adolescents having symptoms of both disorders.5
The 2019 National Survey on Drug Use and Health showed that 15.7% of adolescents age 12 to 17 years had experienced a major depressive episode (MDE) during the past year and 11.1% experienced an MDE with severe impairment.6 According to the 2019 Youth Risk Behavior Survey (YRBS) adolescents reported an increase in feelings of depression, thoughts of suicide, and suicide attempts over the past year compared to previous years. It is therefore essential that women’s health nurse practitioners and other clinicians who provide primary care for adolescents routinely screen and evaluate for mental health conditions and be prepared to confidently address concerns to reduce long-term consequences. This article provides a brief overview of the prevalence of and risk for depression and anxiety among adolescents in the US, evidence-based resources for patient evaluation, and management options for these common mental health conditions identified in primary care settings.
Vulnerable populations
While any adolescent may experience depression or anxiety, there are specific populations recognized as being particularly vulnerable to these conditions and other associated mental health issues. Among them are individuals who have substance use disorders (SUDs), those who identify as lesbian, gay, bisexual, transgender, queer, or questioning (LGBTQ), and those who have had adverse childhood experiences (ACEs).
Adolescents with an MDE are more likely to use substances (eg, illicit drugs, marijuana, opioids, alcohol, cigarettes) compared with their counterparts without an MDE (Table 1).6

Approximately 3.1% of adolescents with an MDE with or without severe impairment have a substance use disorder (SUD).6 The order of onset of MDE and SUD among adolescents has not been established, that is, whether the onset of an MDE preceded the SUD or vice versa.6 Substance use is of particular concern among this age group considering its association with other risk behaviors, unintentional injuries, and suicide, the leading causes of mortality in adolescents.6,7,9,10
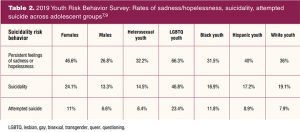
Adolescents who identify as LGBTQ have higher rates of depression, anxiety, substance use, and suicidal ideation compared to heterosexual and cisgender adolescents.7–9,11 LBGTQ adolescents often experience bullying in social settings and are at risk for negative reactions from adult caregivers and peers because of their sexual orientation or gender identity. They have rates twice that of heterosexual/cisgender adolescents of reported persistent feelings of sadness or hopelessness, more than three times the rates for suicidality, and almost four times the rates of attempted suicide, with transgender and nonbinary adolescents having the highest rates among groups (Tables 2,3).7,9,11
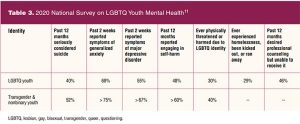
An additional vulnerability for anxiety and depression is adverse childhood experiences (ACEs) such as psychological or physical trauma, homelessness, or sexual abuse. Females age 16 to 19 years are four times more likely to have experienced rape, attempted rape, or sexual assault than the general population, and 25% of girls experience sexual abuse in childhood, putting females at higher risk for ACEs and the resulting mental health ramifications.12,13 LGBTQ youth are particularly vulnerable, with 30% experiencing physical threat or harm (40% of transgender and nonbinary youth) and 29% experiencing homelessness, being kicked out, or running away due to their identity.11 Children and adolescents with multiple ACEs have higher rates of substance use and mental illness.14
Screening and assessment in the primary care setting
An adolescent-focused psychosocial history taking approach, using the acronym HEEADSSS (Home, Education/Employment, Eating, Activities [including social media and sleep pattern], Drugs, Sexuality, Suicide [mood], and Safety), offers a standardized process for gathering psychosocial data, a starting place for clinicians caring for adolescent patients.15,16 The HEEADSSS approach facilitates discussion about environmental stressors, identifies risk-taking behaviors, and provides opportunity for the clinician to illuminate strengths, promote resiliency, and offer education. It is important to establish a safe, trusting environment that is patient centered and ensures confidentiality. Establishing this routine policy of confidential care for adolescents, with the caveat that safety concerns such as suicidal ideation or self-harm behaviors would be shared, is an effective strategy for patient-centered care. Ensuring confidentiality and using a standardized psychosocial assessment tool such as HEEADSSS enhances the likelihood of honest responses to guide evaluation and interventions, and also promotes a smooth transition of adolescents to adult healthcare.17 The HEEADSSS assessment provides valuable overall insight into an adolescent’s life, creates opportunities for further discussion about areas of concern, and is applicable to all adolescents, making it the preferred psychosocial history tool for this age group. If the HEEADSSS assessment reveals incidence or risk of substance use, anxiety, or depression, additional evaluation should be employed.
Standardized screening beyond the use of HEEADSS is crucial in identifying risk for and existence of anxiety and depression in adolescents. The American Academy of Pediatrics (AAP) and the US Preventive Services Task Force recommend routine screening for depressive symptoms in adolescents age 12 years and older.18–20 The Women’s Preventive Services Initiative recommends routine screening for both anxiety and depression starting at age 13 years for females.21 The Patient Health Questionnaire-9 (PHQ-9), a standardized 9-question self-assessment tool for depressive symptoms, has been validated for use with adolescents (sensitivity 85%, specificity 78.8%).22 A shortened PHQ-2 consisting of the first two questions of the PHQ-9 can be used for initial depression screening, with a positive score (≥ 2 points) prompting full PHQ-9 screening for a more thorough assessment of depression and suicide risks.23–25
The Generalized Anxiety Disorder 7-item scale (GAD-7) is a helpful screening tool for identifying the presence of anxiety. It is well-validated in adults and has shown similar psychometrics with adolescents.26,27 The Screen for Child Anxiety Related Disorders (SCARED) questionnaire, another validated screening tool used among pediatric and adolescent populations, offers a standardized comprehensive risk assessment of overall anxiety symptoms and identifies specific forms of anxiety (generalized anxiety, panic disorder, social anxiety, separation anxiety, and school avoidance).28–30 This tool can help the primary care provider better assess anxiety and tailor recommendations to the patients’ needs. Both the GAD-7 and the SCARED questionnaires can be used to monitor symptoms over time with repeated measures, providing a quantifiable assessment of patient progress.
The PHQ-9 and GAD-7 are readily available from the American Academy of Pediatrics Bright Futures Tool Kit and the American Academy of Child and Adolescent Psychiatry (AACAP) Toolbox for Clinical Practice and Outcomes for use as pre-visit or in-person screening tools. The AACAP Toolbox also includes the SCARED questionnaire for clinical use. Both paper and electronic versions of these tools are available, with the AAP offering individual practice support for integration into electronic health records as well. When planning for implementation of adolescent screening tools, practice resources (personnel, finances, type of records used – electronic vs paper, availability of devices for patient use in office), individual patient access to technology and electronic health records, and completion rates of pre-visit requirements must be considered.
Patients older than age 11 years should also be routinely screened for use of tobacco, electronic nicotine products, alcohol, marijuana, and illicit substances using a standardized screening questionnaire or using HEEADSSS.18,19,21,31 General substance-use questions are included in the HEEADSSS assessment, but the SBIRT [Screening, Brief Intervention, and Referral to Treatment] framework provides a more structured evaluation consisting of Screening to Brief Intervention questions of how often the adolescent uses alcohol, tobacco, and marijuana.31,32 Considering the increasing use of electronic nicotine products by adolescents (4.9% of middle school and 20.8% of high school students in 2018) and that the current Screening to Brief Intervention questions use the language of tobacco only, it is essential for providers to inquire specifically about electronic nicotine products when screening patients.33 The terms “Juuling” and vaping are most familiar to adolescents and consistent with the vernacular used in their peer group.
During the adolescent physical examination, it is important to pay close attention to affect, language and behavioral cues, scarring or evidence of cutting/self-harm, bruising, or other indicators of physical abuse, sexual abuse, or trauma. Careful attention to changes in weight, specifically unexpected weight loss or gain, can provide additional cues for more extensive evaluation. Appropriate laboratory testing may include thyroid levels and/or drug screening if there are concerning physical exam findings or positive mental health screening results.
Clinical management of adolescent mental health
Effective treatment of anxiety and depression requires early identification of symptoms, mitigation of risks, and promotion of protective factors that reduce symptoms, risk of substance use disorder, and suicide. Conditions are diagnosed using specific criteria outlined in the Diagnostic and Statistical Manual of Mental Disorders, 5th ed., and treatment guidelines are available for managing adolescent anxiety and depression via primary care.34,35 Moderate-to-severe and complex/comorbid conditions managed with pharmacologic and cognitive behavioral therapies from mental health specialists have the best long-term outcomes. Although adolescents with suicidal ideation require immediate interventions, primary care providers may initiate pharmacologic therapy for adolescent depression and anxiety. Selective serotonin reuptake inhibitors (SSRIs; citalopram, escitalopram, fluoxetine) are the accepted first-line agents.34,35 It is important to remember that these medications do include a black box warning for possible increased suicidal thoughts and behaviors in children, adolescents, and young adults, requiring close monitoring and education of the patient and family. As multiple studies support the combination of an SSRI and psychotherapy as more effective than either of these treatment modalities alone, the clinician should also facilitate referral to mental health counseling.34,36 Adolescents with mild or transient symptoms of depression and anxiety may benefit from primary care interventions promoting well-being and relieving mild symptoms, reducing the risk for suicide, drug use, or acting out behaviors, and providing support and education. These include:
- Drink more water. Irritability is one of the first signs of mild dehydration. Promoting six to eight 8-ounce glasses of water/day improves hydration, mood, mental clarity, and gastric motility. Suggesting a personalized reusable water bottle or canteen often motivates adolescents. Those who dislike “plain water” may consider readily available flavor additives that are sugar and caffeine free.
- Get some rest. Sleep hygiene, aiming for 8 to 10 hours of uninterrupted sleep/night as recommended by the National Sleep Foundation, can ease symptoms of anxiety, irritability, and depression by “resetting” the brain and quieting the mind. Eliminating caffeine and avoiding vigorous exercise in the evening and blocking the blue light from devices at least an hour before bedtime are recommendations for all adolescents, especially those with mental health concerns. Recommending reading or other relaxing quiet activities, establishing a bedtime hygiene routine, and using mindfulness practices like slow-paced breathing 4-7-8 (inhaling for 4 counts, hold breath for 7 counts, exhale for 8 counts), brief meditation, or guided imagery are effective strategies to promote sleep. Taking melatonin an hour before designated sleep time may assist in establishing the routine to promote uninterrupted sleep.
- Attitude of gratitude. Mindfulness practices focusing on positive characteristics strengthen resiliency. The simple practice of identifying “three good things” daily, “ counting blessings,” or using words of gratitude throughout the day releases endorphins, promoting a sense of well-being and stimulating growth of neuro pathways.36 Other strategies include journaling, creative movement (dance/yoga), artistic expression, playing/listening to music, volunteering in the community, or spending time in nature.37,38 Cognitive behavioral therapy (CBT) is a mainstay of managing anxiety and depression—helping adolescents avoid negative thinking can help prevent feeling negative emotions. Utilizing the foundations of CBT and motivational interviewing skills to set mutual goals for gratitude thinking and including this practice at follow-up visits is an effective strategy.
- Build a bridge. Adolescents benefit from meaningful longitudinal relationships with adults and peers who serve as role models, mentors, coaches, or “safety nets” to promote resiliency and reduce rates of depression, drug use, and risky sexual behaviors.38,39 The supportive adult can be the parent or caregiver but can also include an educator, coach/advisor, community leader, or healthcare provider, as the common developmental task of adolescence is to separate self from parents. Providers establishing a long-term, trusting relationship with adolescents can leverage their influence to express concern, establish mutual goals to manage depression/anxiety symptoms, and maintain the relationship as their medical home by requesting follow-up visits with adolescents who have positive screening results. Evidence shows that telehealth, text messaging, phoning, or establishing peer-mentoring efforts are effective in promoting resiliency, reducing anxiety symptoms and hopelessness.40–42
Of special importance, are strategies to promote attentive care specific to vulnerable populations that can increase protective factors and promote further resiliency. As LGBTQ adolescents are at increased risk for ACEs, substance use, depression, anxiety, and suicidal ideation, it is important to provide intentional personalized support. Primary care providers must work diligently to demonstrate an accepting and safe environment for LBGTQ adolescents, as affirming care is associated with improved outcomes in general, and consistently lower rates of suicide attempts, especially among transgender and nonbinary adolescents.11 Using adolescents’ chosen pronouns, strategically including icons such as a rainbow or pink triangle in clinical settings, demonstrating a culturally competent, nonjudgmental posture and using appropriate terminology throughout patient interviews, and having community and national support resources readily available to LBGTQ adolescents and their caregivers are important in creating an open, inclusive, and respectful environment. These resources can include the Trevor Project, the Gay and Lesbian Support Network, the American Academy of Pediatrics, the CDC, and the Parent, Families and Friends of Lesbians and Gays organization. Considering that 46% of LGBTQ adolescents desire professional assistance with their mental health concerns but are unable to obtain it, and 40% report concerns of parental permission as a barrier to receiving care, it is even more important to provide affirming care in the primary care setting.11
HEEADSSS remains a valuable strategy in primary care for all adolescents to identify social contributors of health (eg, home, education/employment, eating, activities, drugs, sexuality, suicide, safety) that may also place them at risk for mental health issues. Providing assistance as needed through referral to available resources is important in both prevention and treatment of mental health conditions.
Covid-19 and adolescent mental health
Adolescents have needs for social interaction and peer relationships that have been significantly challenged with the Covid-19 pandemic.43,44 The prolonged quarantine and shift from in-person to virtual learning made it difficult for adolescents to maintain their peer support networks and meaningful interpersonal relationships. Although many tried to stay connected via social media and other virtual technologies, this work-around was not equivalent to in-person interaction and led to common feelings of social isolation and resulting mental health consequences.43 The continued uncertainty of when a true return to normal will occur creates a lingering atmosphere of stress and anxiety. Additionally, the pandemic has impacted access to care for adolescents with pre-existing mental illness. It is important, and will continue to be important for some time to come, to inquire about, support, and address these issues in the primary care setting. Providing screening for anxiety, depression, and suicidality at every visit with an adolescent is a necessity in the post-Covid landscape. Although we understand this situation and its impact on the immediate mental health of adolescents, we will not have a true and thorough comprehension of the long-term consequences until well into the future.44
Conclusion
Women’s health nurse practitioners and other clinicians who provide primary care for adolescents can improve screening, identification, and treatment of anxiety and depression. Incorporating an adolescent-centered comprehensive history approach, standardized screening tools, and interventions that promote and support resiliency, providers can impact substance use, high-risk behaviors, adolescent safety, and mental health outcomes. With the significant prevalence of mental health concerns in adolescents, this evidence-based approach can have a marked impact on the health of each young patient. It is essential that primary care providers screen for and address concerns at every visit to best support the success of adolescent patients in this vulnerable time of growth and development.
Malinda S. Teague is a pediatric nurse practitioner and Assistant Professor and Lead Faculty in the primary care PNP program at Duke University School of Nursing in Durham, North Carolina. Anne L. Derouin is a pediatric nurse practitioner and Professor and Assistant Dean for the MSN program at Duke University School of Nursing. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
References
- Tang MH, Pinsky EG. Mood and affect disorders. Pediatr Rev. 2015;36(2):52-61.
- Jones PB. Adult mental health disorders and their age at onset. Br J Psychiatry. 2013;202(s54):s5-s10.
- Kessler R, Berglund P, Demler O, et al. Lifetime prevalence and age-of-onset distributions of DSM-IV disorders in the National Comorbidity Survey Replication. Arch Gen Psychiatry. 2005;62(6):593-602.
- Whitney DG, Peterson MD. US national and state-level prevalence of mental health disorders and disparities of mental health care use in children. JAMA Pediatr. 2019;173(4):389-391.
- American College of Obstetricians and Gynecologists. Mental health disorders in adolescents. Committee Opinion Number 705. Obstet Gynecol. 2017;130:e32-41.
- Substance Abuse and Mental Health Services Administration. Key substance use and mental health indicators in the United States: Results from the 2019 National Survey on Drug Use and Health. Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration; 2020. HHS Publication No. PEP20-07-01-001, NSDUH Series H-55. September 2020.
- Johns MM, Lowry R, Haderxhanaj LT, et al. Trends in violence victimization and suicide risk by sexual identity among high school students—Youth Risk Behavior Survey, United States, 2015–2019. MMWR Suppl. 2020;69(1):19-27.
- Jones CM, Clayton HB, Deputy NP, et al. Prescription opioid misuse and use of alcohol and other substances among high school students—Youth Risk Behavior Survey, United States, 2019. MMWR Suppl. 2020;69(1):38-46.
- Ivey-Stephenson AZ, Demissie Z, Crosby AE, et al. Suicidal ideation and behaviors among high school students—Youth Risk Behavior Survey, United States, 2019. MMWR Suppl. 2020;69(1):47-55.
- Centers for Disease Control and Prevention. FastStats – Adolescent health. April 14, 2021.
- The Trevor Project. 2020 National Survey on LGBTQ Youth Mental Health. New York, New York: The Trevor Project. 2020
- Children and teens: Statistics. Rape, Abuse, and Incest National Network.
- Centers for Disease Control and Prevention. Preventing Child Sexual Abuse. March 20, 2020.
- Hughes K, Bellis MA, Hardcastle KA, et al. The effect of multiple adverse childhood experiences on health: a systematic review and meta-analysis. Lancet Public Health. 2017;2(8):e356-e366.
- Goldenring JM, Rosen DS. Getting into adolescents’ heads: an essential update. Contemp Pediatr. 2004;21(1):64-90.
- HEEADSSS 3.0: The psychosocial interview for adolescents updated for a new century fueled by media. HEEADSSS Resource Center. Contemp Pediatr. January 1, 2014.
- Ford C, English A, Sigman G. Confidential health care for adolescents: position paper of the Society for Adolescent Medicine. J Adolesc Health. 2004;35(1):1-8.
- Recommendations for preventative pediatric health care. American Academy of Pediatrics.
- Hagan JF, Shaw JS, Duncan PM, eds. Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. 4th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2017.
- US Preventive Services Task Force. Screening for depression in children and adolescents: US Preventive Services Task Force recommendation statement. Ann Intern Med. 2016;164:360-366.
- Phipps MG, Son S, Zahn C, et al. Women’s Preventive Services Initiative’s well-woman chart: a summary of preventive health recommendations for women. Obstet Gynecol. 2019;134(3):465-469.
- Richardson LP, McCauley E, Grossman DC, et al. Evaluation of the Patient Health Questionnaire (PHQ-9) for detecting major depression among adolescents. Pediatrics. 2010;126(6):1117.
- Levis B, Sun Y, He C, et al. Depression Screening Data (DEPRESSD) PHQ Collaboration. Accuracy of the PHQ-2 alone and in combination with the PHQ-9 for screening to detect major depression: systematic review and meta-analysis. JAMA. 2020;323(22):2290-2300.
- Manea L, Gilbody S, Hewitt C, et al. Identifying depression with the PHQ-2: a diagnostic meta-analysis. J Affect Disord. 2016;203:382-395.
- Richardson LP, Rockhill C, Russo JE, et al. Evaluation of the PHQ-2 as a brief screen for detecting major depression among adolescents. Pediatrics. 2010;125(5):e1097-e1103.
- Mossman SA, Luft MJ, Schroeder HK, et al. The Generalized Anxiety Disorder 7-item scale in adolescents with generalized anxiety disorder: signal detection and validation. Ann Clin Psychiatry. 2017;29(4):227-234A.
- Tiirikainen K, Haravuori H, Ranta K, et al. Psychometric properties of the 7-item Generalized Anxiety Disorder Scale (GAD-7) in a large representative sample of Finnish adolescents. Psychiatry Res. 2019;272:30-35.
- Birmaher B, Khetarpal S, Brent D, et al. The Screen for Child Anxiety Related Emotional Disorders (SCARED): scale construction and psychometric characteristics. J Am Acad Child Adolesc Psychiatry. 1997:36(4):545-553.
- Birmaher B, Brent D, Chiappetta L, et al. Psychometric properties of the Screen for Child Anxiety Related Emotional Disorders (SCARED): a replication study. J Am Acad Child Adolesc Psychiatry. 1999;38(10):1230-1236.
- Wehry AM, Beesdo-Baum K, Hennelly MM, et al. Assessment and treatment of anxiety disorders in children and adolescents. Curr Psychiatry Rep. 2015;17(7):52.
- Levy SJL, Williams JF, Committee on Substance Use and Prevention. Substance use screening, brief intervention, and referral to treatment. Pediatrics. 2016;138(1):e1-e15.
- Levy S, Weiss R, Sherritt L, et al. An electronic screen for triaging adolescent substance use by risk levels. JAMA Pediatr. 2014;168(9):822-828.
- Cullen KA, Ambrose BK, Gentzke AS, et al. Notes from the field: Use of electronic cigarettes and any tobacco product among middle and high school students – United States, 2011-2018. MMWR Morb Mortal Wkly Rep. 2018;67(45):1276-1277.
- Zuckerbrot RA, Cheung A, Jensen PS, et al; GLAD-PC STEERING GROUP. Guidelines for Adolescent Depression in Primary Care (GLAD-PC): part I. Practice preparation, identification, assessment, and initial management. Pediatrics. 2018;141(3):e20174081.
- Southammakosane C, Schmitz K. Pediatric psychopharmacology for treatment of ADHD, depression, and anxiety. Pediatrics. 2015;136(2):351-359.
- Adair KC, Kennedy LA, Sexton JB. Three good tools: positively reflecting backwards and forwards is associated with robust improvements in well-being across three distinct interventions. J Posit Psychol. 2020;15(5):613-622.
- Kondo MC, Oyekanmi KO, Gibson A, et al. Nature prescriptions for health: a review of evidence and research opportunities. Int J Environ Res Public Health. 2020;17(12):4213.
- Lee JA, Heberlein E, Pyle E, et al. Evaluation of a resiliency focused health coaching intervention for middle school students: building resilience for healthy kids program. Am J Health Promot. 2021;35(3):344-351.
- Douglas LJ, Jackson D, Woods C, Usher K. Rewriting stories of trauma through peer-to-peer mentoring for and by at-risk young people. Int J Ment Health Nurs. 2019;28(3):744-756.
- Keith DJ, Rinchuse DJ, Kennedy M, Zullo T. Effect of text message follow-up on patient’s self-reported level of pain and anxiety. Angle Orthod. 2013;83(4):605-610.
- Mheidly N, Fares MY, Fares J. Coping with stress and burnout associated with telecommunication and online learning. Front Public Health. 2020;8(574969).
- Ellis WE, Dumas TM, Forbes LM. Physically isolated but socially connected: psychological adjustment and stress among adolescents during the initial COVID-19 crisis. Can J Behav Sci. 2020;52(3);177-187.
- Loades ME, Chatburn E, Higson-Sweeney N, et al. Rapid systematic review: the impact of social isolation and loneliness on the mental health of children and adolescents in the context of COVID-19. J Am Acad Child Adolesc Psychiatry. 2020;59(11):1218-1239.e3.
- Nearchou F, Flinn C, Niland R, et al. Exploring the impact of COVID-19 on mental health outcomes in children and adolescents: a systematic review. Int J Environ Res Public Health. 2020;17(22):8479.
Key words: adolescent, mental health, screening, treatment, depression, anxiety
Womens Healthcare. 2022;10(2):36-42. doi:10.51256/WHC042236