Before reading the article, click here to take the pretest.
Long-acting reversible contraceptives, or LARC, are growing in popularity because they are highly effective, safe, and well tolerated. In addition, LARC methods require virtually no effort on the part of users besides seeing their healthcare provider (HCP) for insertion and removal. The authors describe their experience in “getting to yes”—that is, in encouraging HCPs to offer LARC methods in a patient-friendly environment and patients to consider using them—so that teens and women have access to all methods, autonomy over their method decision, and decreased risk of unintended pregnancy.
Key words: long-acting reversible contraceptives, LARC, intrauterine contraceptive, IUC, IUD, LNG-IUS
Of the 6.1 million pregnancies in the United States each year, 45% are unintended—either mistimed (27%) or unwanted (18%).1,2 Ninety-five percent of unintended pregnancies occur in females who do not use contraceptives (54%) or who use them inconsistently (41%).1 These unintended pregnancies may end in abortion (42%) or birth (58%),2 both of which have socioeconomic, fiscal, and health-related consequences. Births resulting from unintended or closely spaced pregnancies can have a variety of adverse maternal and child health outcomes.1 Furthermore, females who have children before they are ready are less likely to reach their educational, career, financial, and/or family-related goals.
Unintended pregnancies can be avoided by correct and consistent use of a birth control method. Among all reversible methods, those that require the least amount of effort by the user have been demonstrated to be the most effective at pregnancy prevention.
Background information on LARC
Long-acting reversible contraceptives, or LARC, include the subdermal implant and intrauterine contraceptives (IUCs).3 Both implants and IUCs are highly effective in preventing pregnancy and are FDA-approved for 3-10 years of use. In addition, these methods are reversible and do not impair fertility once they are removed; users who wish to become pregnant can have them removed at any time. LARC methods are the most effective forms of reversible birth control available: During the first year, fewer than 1% of implant or IUC users will become pregnant.4 Failure rates associated with the use of other contraceptives are considerably higher.
Devices
The implant is a single, matchstick-sized, etonogestrel-containing rod that is placed in the subdermal tissue of the inside aspect of the upper non-dominant arm.5 The implant, which is marketed as Nexplanon®, contains barium, allowing localization with radiography. The implant is FDA-approved for 3 years of use.
Intrauterine contraceptives, either an intrauterine device (IUD) or an intrauterine system (IUS), are T-shaped devices containing copper or levonorgestrel (LNG).6 Four IUCs are available, the Copper T 380A (ParaGard®) and three LNG-IUS products: Mirena®, Skyla®, and Liletta®. The copper IUD is effective immediately following placement7 and is FDA approved for 10 years of use.6 Mirena is FDA approved for 5 years of use, and Skyla and Liletta for 3 years of use.6 Data collection for Liletta is ongoing; it is expected that the manufacturer will ultimately seek approval for up to 7 years of use. If an LNG-IUS product is placed during the first 7 days of the menstrual cycle or immediately following birth, a miscarriage, or a first-trimester abortion, then back-up contraception is not needed.6,8 Otherwise, a backup method is recommended for the first 7 days.
Of note, LARC methods do not protect users against sexually transmitted infections (STIs). Condoms are needed for protection against STIs.
Medical eligibility criteria
All teenagers and women should be considered candidates for LARC use until proven otherwise.9-11 Readers can access the CDC’s Summary Chart of U.S. Medical Eligibility Criteria for Contraceptive Use. Information from the CDC is also available as a free iPhone or iPad app at the iTunes store or as an eBook available on an eReader app.
Trends in LARC use
LARC methods are gaining in popularity for many reasons, but mainly because of their high efficacy.12 According to an analysis of National Survey for Family Growth (NSFG) data, the proportion of female U.S. contraceptors using the IUD or implant increased from 2.4% in 2002 to 3.7% in 2007 and to 8.5% in 2009.13 According to a more recent analysis of the NSFG data, the prevalence of LARC use among contraceptors rose from 8.5% in 2009 to 11.6% in 2012, a significant increase.14,15 Much of this trend was driven by IUC use, which increased from 7.7% to 10.3%; implant use remained low (1.3%) and did not change significantly between these two time periods.
The Contraceptive CHOICE Project
Although increased use of LARC methods has been encouraging, uptake is still relatively low—especially considering the high rate of unintended pregnancy in this country, the superior efficacy of these methods, and the many non-contraceptive benefits they offer. The next logical question is, What can be done to increase education about and access to LARC methods for reproductive-aged females who wish to prevent pregnancy?
Purpose and methods
The Contraceptive CHOICE Project was undertaken to remove educational, financial, and access barriers to contraception; to promote the most effective methods of birth control; and to reduce unintended pregnancy in the St. Louis, Missouri, area.16 Objectives of the project were to increase uptake of LARC; to measure/analyze method choice, satisfaction, side effects, and continuation across all reversible contraceptive methods; and to provide enough no-cost contraception to exert a population impact on unintended pregnancies particularly with respect to teen pregnancy and repeat abortion.
Enrollment began in August 2007 and ended in September 2011. Prospective enrollees ranged in age from 14-45 years, wanted to avoid pregnancy for ≥1 year, and were willing to initiate a new form of reversible contraception.17,18 Recruitment was done via word of mouth, referral from private and community healthcare providers (HCPs), and from the two abortion facilities in the St. Louis region. Participants underwent standardized evidencebased contraceptive counseling by trained non-clinicians. The counseling was structured on effectiveness tiers, and included the risk and benefits of each method. Tier 1 contraceptives—the most effective methods, which include LARC (IUCs and the implant)— were described first. Next, the counselor described tier 2 methods or refillables: depot medroxy-progesterone acetate (DMPA), and the pill/patch/ring (PPR). Tier 3 methods, including the diaphragm, the condom, the sponge, spermicide, withdrawal, and fertility awareness-based methods, were described last. Participants received their chosen contraceptive free of charge, and they could switch methods as frequently as they wanted for the duration of their study participation (2-3 years).
Results
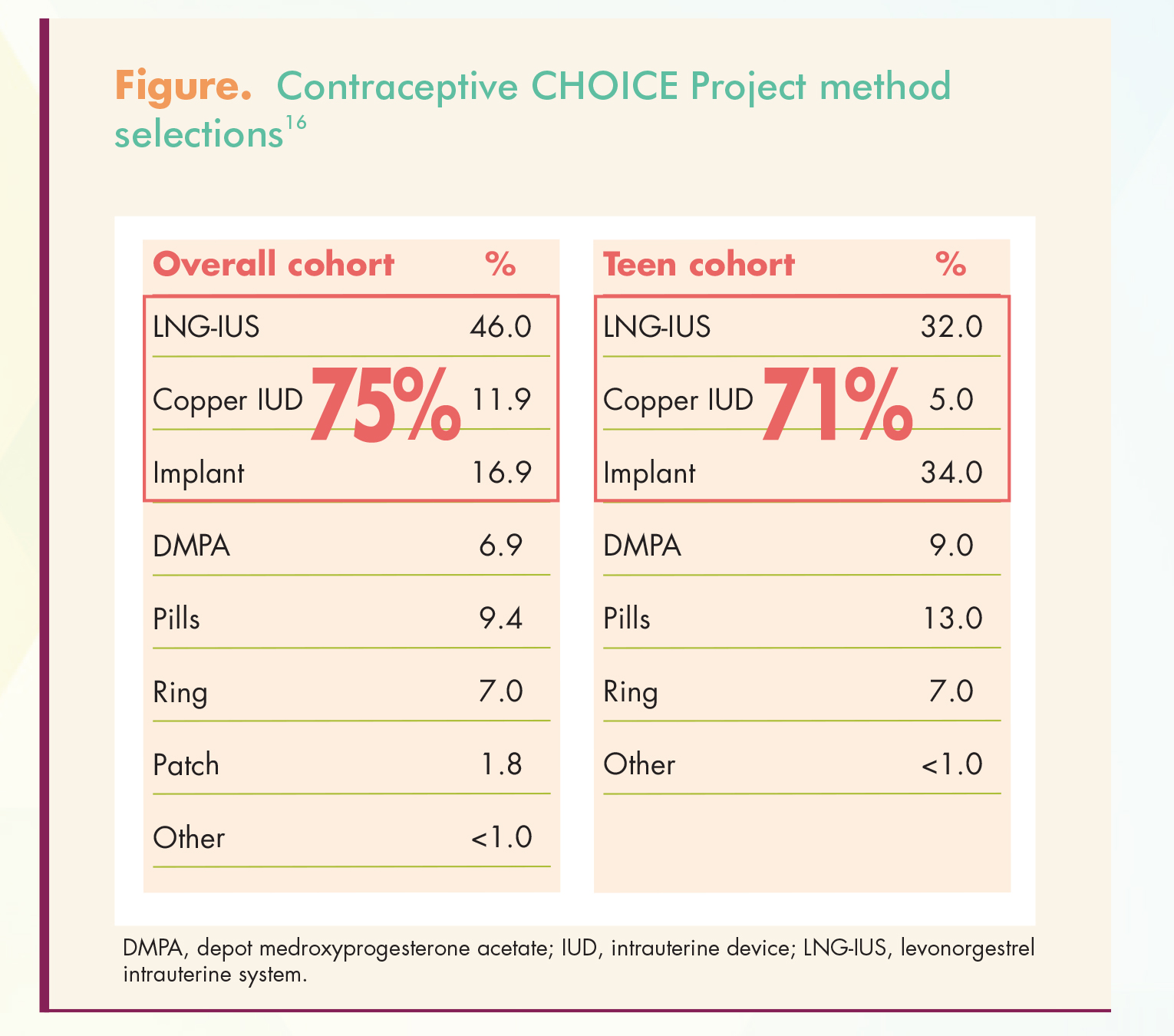
Contraceptive choices of the entire cohort and of the teen cohort alone are shown in the Figure. Among 9,256 adult and teen participants, 75% chose a LARC method; among teens alone, 71% chose a LARC method.
{kind=link}
Continuation rates
Among LARC users, adults and teens had high continuation rates—87% and 82%, respectively— at 12 months.19,20 Non- LARC users had much lower 12- month continuation rates: 59% for adults and 49% for teens. Among LARC users, continuation rates at 24 months were still high: 78% for adults and 67% for teens.20 Only 42% of adult non-LARC users and 37% of teen non-LARC users continued using the contraceptive method they chose at baseline for 24 months. At 3 years, continuation rates were 67.2% among LARC users and 31.0% among non-LARC users.21
Satisfaction levels
Twelve-month satisfaction levels mirrored continuation rates. A greater proportion of LARC users than non-LARC users reported being very satisfied or somewhat satisfied with their method (81.2% vs. 48.8%).19 This differential in satisfaction between LARC users and non-LARC users held true for adults (82% vs. 50%) and for teens (75% vs. 42%). Satisfaction was similarly high among users of the subdermal implant, copper IUD, or LNG-IUS (range, 72% for teen users of the copper IUD to 84% for adult users of the LNG-IUS) and similarly low among users of DMPA or PPR (range, 31% for teen users of the ring to 52% for adult users of DMPA or the ring).
Unintended pregnancy and abortion rates
Even more important, among 7,486 participants included in this analysis, 334 (4.5%) experienced unintended pregnancies.4 Failure rates among PPR users were 4.8%, 7.8%, and 9.4% in years 1, 2, and 3, respectively; corresponding rates among LARC users were 0.3%, 0.6%, and 0.9%
(P <.001). Failure rates among DMPA users were similar to those of the LARC users. LARC methods were highly effective in preventing pregnancy regardless of a user’s age, whereas teen PPR users were twice as likely as adult PPR users to become pregnant.
One of the primary outcomes of interest was the percentage of abortions that were repeat abortions.18 Using vital statistics data from Missouri’s state health department, the investigators found a significant difference in the proportion of repeat abortions between the St. Louis region and Kansas City in 2009 (respective rates, 46% vs. 49%; P = .02) and 2010 (respective rates, 44% vs. 51%; P <.01). In addition, they detected a significant decline in the proportion of repeat abortions over time in the St. Louis region (P = .002). Another analysis revealed that pregnancy, birth, and abortion rates among teens in the CHOICE Project were substantially lower than national rates among sexually experienced teens.22 Respective annual rates of pregnancy, birth, and abortion were 34.0, 19.4, and 9.7 per 1,000 teen CHOICE Project participants, as compared with 158.5, 94.0, and 41.5 per 1,000 sexually experienced U.S. teens in 2008.
Summary of main findings
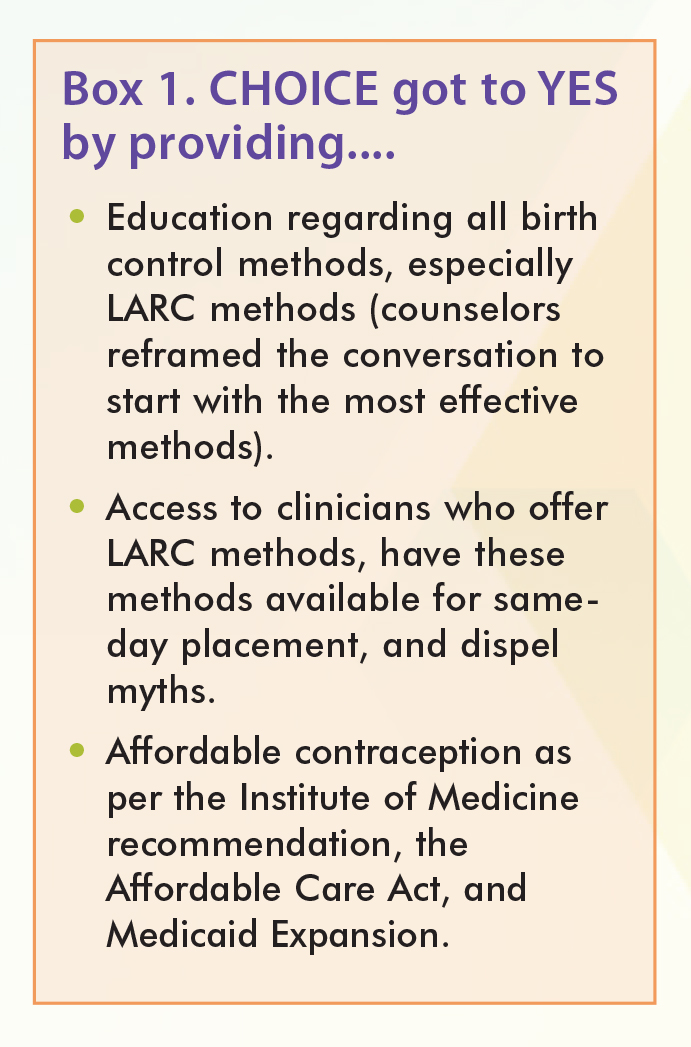
LARC methods, as compared with shorter-acting methods, were associated with higher continuation rates and user satisfaction levels, regardless of age. In addition, LARC methods were associated with lower rates of unintended pregnancy and, as a consequence, lower rates of birth and abortion. An informative video about the Contraceptive CHOICE Project is available at Pathway to Choice. Box 1 shows how CHOICE got to yes.
{kind=link}
Barriers to IUC use, and how to overcome them
In order for the encouraging results of the CHOICE Project to translate to other populations throughout the country, barriers must be overcome. From this point onward, this article focuses on IUCs.
The National Committee for Quality Assurance has issued a White Paper, Women’s Health: Approaches to Improving Unintended Pregnancy Rates in the United States, that describes numerous barriers that impede our nation’s ability to reduce the rate of unintended pregnancy. To read a summary of these barriers, click here. To read the entire White Paper, click here.
Provider barriers
Many HCPs have concerns about prescribing and placing IUCs. Many of these concerns are easily addressed.
Lack of training
If an HCP’s training occurred prior to 2001, she or he may not have received instruction in IUC placement. To acquire such training, HCPs can seek out instructors provided by product manufacturers or academic institutions, or they can attend conferences where such training is provided. HCPs need not be certified by the manufacturer to place IUCs; any HCP who feels comfortable with the instructions and the procedure may place them.
Too few patients to gain competency
An HCP such as a primary care provider or a rural health provider may not see enough patients to maintain a comfortable competency in IUC placement. This barrier may or may not be surmountable; each HCP has her or his own threshold for a feeling of competency. One approach is to form a collaborative relationship with a high-volume provider who can offer ongoing support and training. In addition, if HCPs view each patient encounter with a reproductive-aged female as an opportunity to address her goals with respect to pregnancy and/or pregnancy prevention, then they will likely be providing many more contraceptive services than they think.
Fear of litigation
Some HCPs may fear litigation if complications arise; some of the items in the bulleted list in the next section can help dispel this fear. Concerns based on myths Each of these myths surrounding IUCs is debunked.
• Teenagers and nulliparous women are not appropriate candidates for IUCs. Evidence shows that these females are excellent candidates for IUCs, which are highly effective regardless of age or parity.10
• Young women won’t like IUCs because placement is too painful. Placement comfort varies from patient to patient. Many young women tolerate the placement procedure very well.23
• Most patients cannot afford IUCs. Many women have coverage for IUCs.24 More will be able to get them as the Affordable Care Act (ACA) continues to implement the 2011 Institute of Medicine recommendations.
• Women should have IUC counseling at one visit and return for IUC placement at the next visit. Two-thirds of women prefer to have the IUC placed on the same day it is prescribed.25 Adding a second visit places an extra barrier between the patient and her receiving the desired contraceptive, thereby increasing her risk for unintended pregnancy.
• Patients won’t keep their IUCs. IUCs had the highest continuation rates of any method offered in the CHOICE Project.26
• Patients already know what they want. When CHOICE Project participants were advised of all their birth control options and allowed to choose what they wanted, 58% chose an IUC. In the real world, only 10% of U.S. females choose an IUC.14,15 Many females are unfamiliar with LARC methods or harbor misconceptions about them. They cannot know what they want unless they are fully informed about the options.
• HCPs don’t have time to tell patients about every method. Trained staff members can inform patients of their options, starting with the most effective methods.27 In addition, HCPs can provide decision aids that patients can use in the waiting room before their visits.
High upfront cost
The high cost to stock IUCs, with a delay in reimbursement, may keep some HCPs from offering them. The ACA has helped in that the cost of a contraceptive and its placement should be fully covered, with no cost share to the patient. However, barriers do remain: Some health insurance plans exclude contraceptive coverage for religious reasons, small companies need not comply, and some state plans do not cover at 100% or have restrictions on use.
Concern about a prospective IUC user being pregnant
According to the U.S. Selected Practice Recommendations for Contraceptive Use, an HCP can be reasonably certain that a patient is not pregnant if she has no signs or symptoms (S/S) of pregnancy, has a negative urine pregnancy test result, and meets any one of these criteria8:
• ≤7 days after the start of her normal menses;
• abstinence since the start of her last normal menses;
• correct and consistent use of contraception;
• ≤7 days after spontaneous or induced abortion;
• within 4 weeks postpartum; or
• fully or nearly fully breastfeeding, amenorrheic, and <6 months postpartum.
Concern about a prospective IUC user having an STI
At-risk patients can be tested for gonorrhea and chlamydia at IUC placement.10 If a positive result is noted, the device can still remain in place. The HCP can treat the infection, offer expedited partner therapy as per CDC guidelines, inform patients about the warning S/S of pelvic inflammatory disease (PID; e.g., new-onset abdominal or pelvic pain, foul-smelling vaginal discharge, pain during or shortly after sex, fever, abnormal uterine bleeding), and retest in 3 months. However, if an HCP suspects active infection at the time, the device should not be placed. Instead, the patient is tested and treated as needed. No evidence suggests that IUCs increase the risk for developing an STI.
Patient barriers
These barriers include lack of knowledge about IUCs, negative influence of friends or the media, lack of access to HCPs who can provide IUCs, and cost concerns. The CHOICE Project overcame these barriers by having non-clinicians educate participants about all birth control methods. HCPs provided same-day LARC placement as per the U.S. Selected Practice Recommendations for Contraceptive Use guidelines.8 The birth control methods were provided free of charge. In Open the Dialogue, CHOICE Project participants describe how they felt when education, access, and cost barriers were removed and they could choose any birth control method they wanted.
IUC risks and side effects
One of the main concerns about IUC placement is uterine perforation, which occurs in about 1 in 1,000 placements.3 Red flags indicating acute uterine perforation include the uterus sounding to a depth greater than that appreciated on bimanual examination, sudden loss of resistance, and patient pain disproportionate to that expected. Vaginal bleeding is unlikely.
Another concern is PID, which develops in fewer than 1% of IUC users, usually during the first 20 days post-placement. Appropriate precaution—screening highrisk women at the time of placement and delaying placement in those with active cervicitis—is the best way to minimize this risk. In very rare cases, pregnancy may occur with the IUC in place; if so, there is a higher chance that it will be an ectopic pregnancy. IUC users with a positive pregnancy test result need to be promptly evaluated to rule out ectopic pregnancy and undergo pregnancy options counseling.
With the copper IUD, menstrual pain and bleeding may increase at first.3 Intermenstrual bleeding may occur as well. These side effects are common in the first few months of use and tend to subside within a year. The LNG-IUS may be associated with spotting, irregular bleeding, and menstrual cramping in the first few months of use. Again, these side effects tend to diminish over time. Some users may experience LNG-related effects such as headache, nausea, depression, and breast tenderness.
Creating a LARC-friendly practice
Healthcare providers who wish to create a LARC-friendly practice know that LARC methods are the most effective reversible methods. They know that every patient is a LARC candidate until proven otherwise. They have ensured that all office staffers are knowledgeable about LARC, can follow an effectiveness tier-based counseling approach as per the CDC guidelines, and promote LARC use. After all, support staff members’ perceptions can greatly affect patients’ decisions. Other tenets of a LARC-friendly practice include the following:
• Every effort is made to help patients obtain the method of their choice.
• Same-day LARC placement is the standard.
• All HCPs have received proper LARC training.
• LARC methods are stocked if possible.
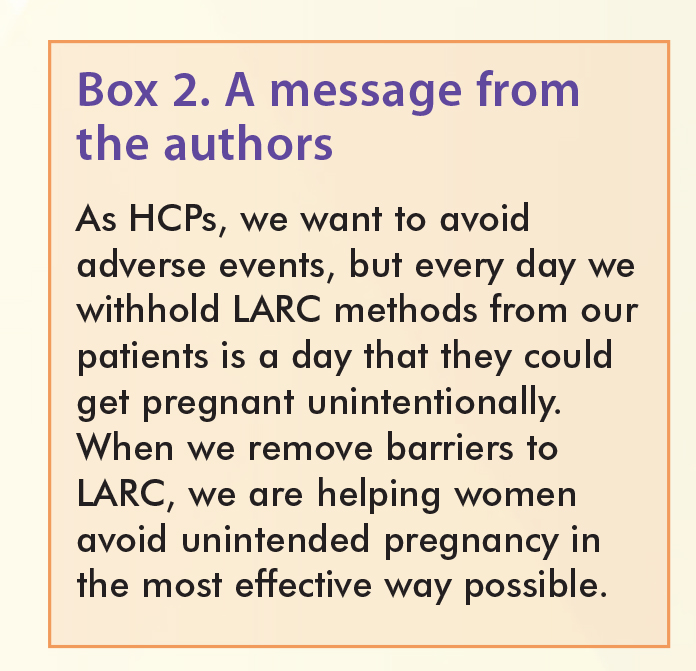
More information about setting up a LARC-friendly practice, including an introductory video, is available at the LARC First website. A message from the authors appears in Box 2.
{kind=link}
Conclusion
Long-acting reversible contraceptives are the most effective birth control methods on the market. As shown in the CHOICE Project, IUCs and implants are superior to other methods in terms of continuation rates and satisfaction levels. As such, LARC methods should be considered first-line options for all females, including adolescents and nul liparous women. LARC method efficacy does not depend on user compliance. HCPs should provide counseling and reassurance so that patients know what to expect at the time of placement, as well as possible side effects. Same-day IUC placement should be the standard. As providers of healthcare to teenage girls and women, HCPs are privileged to be able to have a dramatic impact on patients’ lives with such a simple intervention.
References
1. Guttmacher Institute. Unintended Pregnancy in the United States. Fact Sheet. March 2016.
2. Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374(9):843-852.
3. American Congress of Obstetricians and Gynecologists. Long-Acting Reversible Contraception (LARC): IUD and Implant. May 2016.
4. Winner B, Peipert JF, Zhao Q, et al. Effectiveness of long-acting reversible contraception. N Engl J Med. 2012;366(21):1998-2007.
5. Association of Reproductive Health Professionals. Choosing a Birth Control Method. Implant. Updated June 2014.
6. Association of Reproductive Health Professionals. Choosing a Birth Control Method. Intrauterine Contraception. Updated June 2014.
7. Trussell J. Contraceptive failure in the United States. Contraception. 2011;83(5):397-404.
8. Centers for Disease Control and Prevention. U.S. Selected Practice Recommendations for Contraceptive Use, 2016. July 29, 2016.
9. ACOG Practice Bulletin. Long-Acting Reversible Contraception. #121, July 2011.
10. CDC. U.S. Medical Eligibility Criteria for Contraceptive Use, 2016. July 29, 2016.
11. MacGregor KE, Khadr SN. Contraception for adolescents (American Academy of Pediatrics). Arch Dis Child Educ Pract Ed. 2016;101(2):61-64.
12. Branum AM, Jones J, for the Centers for Disease Control and Prevention. Trends in Long-acting Reversible Contraception Use Among U.S. Women Aged 15–44. NCHS Data Brief No. 188, February 2015.
13. Finer LB, Jerman J, Kavanaugh MLO. Changes in use of long-acting contraceptive methods in the United States, 2007-2009. Fertil Steril. 2012;98(4):893-897.
14. Kavanaugh ML, Jerman J, Finer LB. Changes in use of long-acting reversible contraceptive methods among U.S. women, 2009-2012. Obstet Gynecol. 2015;126(5):917-927.
15. Guttmacher Institute. Use of Long-Acting Reversible Contraceptive Methods Continues to Increase in the United States. Press release. October 8, 2015.
16. Contraceptive CHOICE Project.
17. Secura GM, Allsworth JE, Madden T, et al. The Contraceptive CHOICE Project: reducing barriers to long-acting reversible contraception. Am J Obstet Gynecol. 2010;203(2):115.e1-7.
18. Peipert JF, Madden T, Allsworth JE, Secura GM. Preventing unintended pregnancies by providing no-cost contraception. Obstet Gynecol. 2012;120(6):1291-1297.
19. Rosenstock JR, Peipert JF, Madden T, et al. Continuation of reversible contraception in teenagers and young women. Obstet Gynecol. 2012;120(6):1298-1305.
20. O’Neil-Callahan M, Piepert JF, Zhao Q, et al. Twenty-four-month continuation of reversible contraception. Obstet Gynecol. 2013;122(5): 1083-1091.
21. Diedrich JT, Zhao Q, Madden T, et al. Three-year continuation of reversible contraception. Am J Obstet Gynecol. 2015;213(5):662.e1-8.
22. Birgisson NE, Zhao Q, Secura GM, et al. Preventing unintended pregnancy: the Contraceptive CHOICE Project in review. J Womens Health (Larchmt). 2015;24(5):349-353.
23. McNicholas CP, Madden T, Zhao Q, et al. Cervical lidocaine for IUD insertional pain: a randomized controlled trial. Am J Obstet Gynecol. 2012;207(5):384.e1-6.
24. Clinical Preventive Services for Women: Closing the Gaps. Washington, DC: The National Academies Press; 2011.
25. Stanek AM, Bednarek PH, Nichols MD, et al. Barriers associated with the failure to return for intrauterine device insertion following firsttrimester abortion. Contraception. 2009;79(3):216-220.
26. Peipert JF, Madden T, Allsworth JE, et al. Continuation and satisfaction of reversible contraception. Obstet Gynecol. 2011;117(5):1105-1113.
27. Madden T, Mullersman JL, Omvig KJ, et al. Structured contraceptive counseling provided by the Contraceptive CHOICE Project. Contraception. 2013;88(2):243-249.