
Routine assessment for perinatal anxiety disorders, using established diagnostic criteria and standardized tools, can facilitate early diagnosis, guide management, and optimize outcomes for pregnant women and their offspring.
An anxiety disorder can disrupt a woman’s abilities to enjoy life and to self-care. When an anxiety disorder is present during the perinatal period—that is, during pregnancy and/or the first year postpartum—it can change how a woman experiences her pregnancy and how she interacts with and cares for her child.1 Limited data suggest a possible association between severe perinatal anxiety disorders and adverse pregnancy outcomes such as preterm birth, low birth weight, and postpartum depression.2,3 In addition, maternal anxiety disorders have been linked to developmental and mental health problems in offspring.2,4 Healthcare providers (HCPs) who see women during pregnancy and postpartum need to know the risk factors and signs and symptoms associated with perinatal anxiety disorders so that these disorders can be identified early and treated as needed. This article focuses primarily on the assessment and management of perinatal anxiety.
Perinatal anxiety disorder
Perinatal anxiety refers to anxiety experienced during pregnancy and/or the first 12 months after the birth of a baby.
Prevalence
Estimating the incidence of perinatal anxiety disorders (PAD) is difficult due to lack of consistent terminology regarding definition and symptoms, treatment protocol, and research methodology. Anxiety disorders across the perinatal period have been estimated at 1 in 5 women (20.7%) meeting the diagnostic criteria for at least one of the eight categories of anxiety disorders, with a range of 7.5% to 38.8%.5 More than two types of anxiety disorders have been experienced by 1 in 20 women (5.5%).5 Additional studies report anxiety disorders affect 4% to 39% of women during pregnancy and up to 18% during the postpartum period.6,7 A population-based survey given to 4,451 mothers following delivery of a live newborn found 18% of the participants reported anxiety symptoms and 35% also reported symptoms of depression.8 The reported global prevalence of perinatal anxiety ranges from 10% to 24% compared to perinatal depression from 10% to 20%. In perinatal women, there is a 40% comorbidity of mood and anxiety disorders.9
Risk factors
Perceived lack of partner and/or social support, a history of intimate partner violence or other abuse, a personal history of mental illness, having an unplanned or unwanted pregnancy, past or present pregnancy complications, and past pregnancy loss are risk factors for perinatal anxiety.10 Women experiencing a high-risk pregnancy are also at greater risk for developing anxiety.11 Other risk factors for perinatal anxiety include failure to complete high school, unemployment, and nicotine use.12,13
Symptoms
Some degree of anxiety is common during pregnancy and postpartum, so HCPs should aim to differentiate between “normal” anxiety and perinatal anxiety. Persons in the general population with anxiety may report trembling, twitching, shakiness, muscle aches, sweating, nausea, diarrhea, and an exaggerated startle response.14 During the perinatal period, anxiety may manifest as excessive and persistent nervousness, worry, or even panic about pregnancy and childbirth, the infant’s health, and parenting. Physical features—in addition to those listed for anxiety in general—may include stomach pain, headaches, dizziness, palpitations, and shortness of breath. Anxiety can exacerbate sleep disturbances and fatigue in women during the perinatal period.14
Screening for perinatal anxiety
Routine screening is essential for early recognition of anxiety, which may otherwise go undetected and untreated in pregnant and postpartum women. Some of the most common clinical features of anxiety may be attributed to normal physiologic changes of pregnancy or expected psychosocial adjustments to pregnancy and childcare. A woman may be reluctant to report signs/symptoms of anxiety for fear of bias and ridicule.15
The American College of Obstetricians and Gynecologists (ACOG) advises screening women at least once during the perinatal period for anxiety and depression using a standardized, validated tool.16 ACOG also advises HCPs to closely monitor women who have a history of, or risk factors for, anxiety or depressive disorders.17
Ongoing research is needed to develop an assessment tool with sound theoretical and psychometric properties to identify women who are at risk for perinatal anxiety disorders and women who are currently demonstrating symptoms. The assessment tool needs to distinguish the different types of anxiety disorders and the levels of anxiety. Ideally, the tool will provide information related to the severity of symptoms.18
Anxiety screening instruments used in both pregnant and postpartum women are the Generalized Anxiety Disorder-7 (GAD-7), the Perinatal Anxiety Screening Scale (PASS), and the Anxiety Disorder-13 (AD-13). The GAD-7 is a seven-item self-report questionnaire created to identify essential areas of anxiety (worry, restlessness, irritability, fear and its severity in the previous 2 weeks).19,20 The reported internal consistency of the GAD-7 is excellent (Cronbach’s alpha, .92), and its test/retest reliability is good (intraclass correlation coefficient [ICC], .83). The PASS is useful throughout the perinatal period to assess for a range of anxiety symptoms. Principal component analyses suggested a four-factor structure addressing symptoms of acute anxiety and adjustment; general worry and specific fears; perfectionism, control, and trauma; and social anxiety. The PASS is validated for use in hospital, mental health, and community samples and has excellent reliability (Cronbach’s alpha, .96) and test/retest reliability (ICC, .74). The PASS identified 68% of women with a diagnosed anxiety disorder compared to the Edinburgh Postnatal Depression Scale (EPDS) anxiety subscale that detected 36% of anxiety disorders.21,22 The AD-13 is a self-report questionnaire that identifies core symptoms of anxiety disorders: generalized anxiety disorder, panic disorder, obsessive compulsive disorder, posttraumatic stress disorder (PTSD), and social anxiety disorder. The tool meets the standard of a clinically useful screening measure, with an AUC [area under the curve] above 0.8 based on use of related disorders and without.23 The Box lists various anxiety screens and provides links to them for easy access.
Validated anxiety screening instruments with a postpartum focus include the Postpartum Worry Scale-R (PWS-R) and the Penn State Worry Questionnaire-10 (PSWQ-10). The PWS-R was developed to identify the degree of uncontrollable worry, a major symptom of GAD in postpartum women.24 This revised format of the original PWS includes items related to the mother’s perception of the infant’s well-being in terms of health and development and the mother’s relationship with her child.25,26 The PSWQ-10 measures worry, often described as the cardinal feature of GAD.27 Although the PSWQ-10 cannot distinguish GAD from major depressive disorder, it can track worry, which may affect both treatment and recovery. The EPDS has an anxiety subscale (EPDS-3A) and can reliably differentiate between depression and anxiety.28 Research continues with another screening tool, the Postpartum Specific Anxiety Scale (PSAS). Women who currently experience anxiety and/or depression are easily identified with PSAS, but not with case findings based on preliminary ROC [receiver operating characteristic] analysis.29
Making the diagnosis
Establishing rapport with patients facilitates a discussion of the clinical features of anxiety, screening test results, and treatment options. HCPs need to determine the extent to which anxiety, worry, and/or the physical manifestations of anxiety are causing impairment in social, occupational, or other areas of functioning.
Once perinatal anxiety is identified and diagnosed, the next step is to determine whether an underlying condition might be causing the signs/symptoms or exacerbating their severity (eg, substance misuse/abuse, a physical health condition), as well as whether coexisting psychiatric conditions such as depression, substance abuse, bipolar disorder, psychosis, schizophrenia, or PTSD might be complicating the picture. Referral to a mental health specialist is imperative when a pregnant woman has suicidal ideation, a coexisting psychiatric condition, or need for a complex medication regimen. HCPs providing perinatal care should have resources available for initiating an interprofessional team approach in treating perinatal anxiety.30,31
Management
If perinatal anxiety is determined to be the primary problem, cognitive behavioral therapy (CBT), the first-line treatment for anxiety in the general population, is a reasonable first approach.32 Although less studied in women with perinatal anxiety, CBT has been shown to be effective in treating postpartum depression.33,34 Additional nonpharmacologic options include mindfulness-based cognitive therapy, interpersonal therapy, psychodynamic therapy, acupuncture, and massage.35,36
When nondrug therapies are ineffective or only partially effective, medication may be indicated. In these cases, HCPs and patients should weigh the risks of not fully treating the anxiety disorder, the potential risks to a fetus exposed to the medications chosen, and the potential benefits of easing the anxiety disorder.
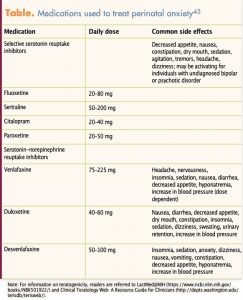
Selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) are first-line drugs for the treatment of moderate or severe anxiety disorders. The Table lists commonly prescribed SSRIs and SNRIs, as well as their recommended dosages and side effects. Research data are not consistent regarding risks associated with use of SSRIs and SNRIs during pregnancy. The research process is often faced with lack of significant statistical difference, resulting in varied results. Experts recommend use of SSRIs and SNRIs during pregnancy when indicated but urge consideration of risk/benefit ratio when selecting appropriate medication.37,38 More information is available on SSRIs than SNRIs because SSRIs have a longer history of use and there has been more research on SSRIs to identify risks and benefits. Risks associated with SSRI use during pregnancy include cardiac defects such as ventricular/atrial/septal defects, persistent pulmonary hypertension, and preterm birth.39–43
Traces of SSRIs and SNRIs will likely be in the woman’s breast milk and in the baby. The baby should be assessed for behavioral changes such as irritability and sedation. If these occur, the medication or breastfeeding will need to be discontinued. Assessment of the mother is imperative, because the postpartum period is high risk for anxiety and depression, an important part of the risk/benefit discussion between the woman and provider. If assessment of the baby indicates no behavioral changes, the woman may continue to breastfeed, based on outcome of the risk/benefit discussion.44 Effective treatment of perinatal anxiety is beneficial to both women and their children.
Use of benzodiazepines should be reserved for acute anxiety on a short-term basis because of the multiple associated risks: worsening of depressive symptoms, possible dependence, and possible overdose. Some data show a small increased risk for preterm birth, low birth weight, and floppy infant syndrome (hypotonia) in infants whose mothers used benzodiazepines during pregnancy. Data are inconclusive in terms of any teratogenic effect. If benzodiazepines are considered for women who are breastfeeding, those with a shorter half-life such as lorazepam and oxazepam are preferred because they are reported to result in low levels in breast milk and because they do not cause adverse effects in breastfed infants. Alprazolam and diazepam, with longer half-lives than some of the other benzodiazepines, should be avoided because of reports of infant sedation.44,45
Psychosocial assessment completed at the initial prenatal visit and updated throughout pregnancy and postpartum provides a foundation for decision making. Clinical judgment is essential in determining the correct diagnosis and creating a plan of care supported by the best available evidence. Protocols require input of an interdisciplinary team of providers.46–48 Improved models of care that not only treat but also reduce risk need to be developed and implemented.
The Council on Patient Safety in Women’s Health Care convened an interdisciplinary work group and developed an evidence-based patient safety bundle to address maternal mental health. The Consensus Bundle on Maternal Mental Health describes four areas to be implemented in every clinical setting to identify maternal mental health issues and create effective treatment plans. The four areas include: readiness; recognition and prevention; response; reporting system and systems learning.49
The readiness area includes identification of mental health screening tools; a response protocol that includes a referral system of existing maternal mental healthcare providers and resources; education of clinicians and office staff; and identification of a key person who is responsible for initiating and maintaining the system. Recognition and prevention promotes a complete comprehensive prenatal intake, use of validated mental health screening on a scheduled sequence, and education to pregnant women and their support structures. Response consists of a stage-based management system that includes family, friends, and community; an emergency referral for women who experience suicide or homicide ideation or psychosis; creation of support for client and support systems; support for staff; and seamless transitions among providers. The reporting system and systems learning involves establishing a nonjudgmental culture of safety, an interdisciplinary review of adverse mental health outcomes, and establishment of local standards for recognition and response to measure compliance, understand individual performance, and track outcomes.49
Implications for practice
Perinatal anxiety is common, and, when severe, has been linked to adverse pregnancy outcomes and to developmental and mental health problems in offspring.50–52 Early identification of and intervention for perinatal anxiety can help alleviate signs and symptoms, improve the perinatal experience, and reduce the risk for adverse outcomes. HCPs need to screen women for anxiety both during pregnancy and postpartum. When anxiety is identified, HCPs should conduct further assessment to determine whether the patient has a coexisting psychiatric disorder that merits referral and collaboration with a mental health specialist. Nonpharmacologic treatments such as CBT should be considered as first-line treatment. Some women may require medication to manage symptoms adequately. Risks and benefits of using medications to treat anxiety during the perinatal period should be considered on an individualized and ongoing basis.
Marian L. Farrell is Professor of Nursing at the University of Scranton in Scranton, Pennsylvania. She is also in private practice as a psychiatric nurse practitioner and clinical nurse specialist. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
- Bauer A, Knapp M, Parsonage M. Lifetime costs of perinatal anxiety and depression. J Affect Disord. 2016;192:83-90.
- Bayrampour H, Ali E, McNeil DA, et al. Pregnancy-related anxiety: a concept analysis. Int J Nurs Stud. 2015;55:115-130.
- Ross LE, McLean LM. Anxiety disorders during pregnancy and the postpartum period: a systematic review. J Clin Psychiatry. 2006;67(8):1285-1298.
- Rubertsson C, Hellström J, Cross M, Sydsjö G. Anxiety in early pregnancy: prevalence and contributing factors. Arch Womens Ment Health. 2014;17(3):221-228.
- Fawcett EJ, Fairbrother N, Cox ML, et al. The prevalence of anxiety disorders during pregnancy and the postpartum period: a multivariate Bayesian meta-analysis. J Clin Psychiatry. 2019;80(4):18r12527.
- Marchesi C, Ossola P, Amerio A, et al. Clinical management of perinatal anxiety disorders: a systematic review. J Affect Disord. 2016;190:543-550.
- Leach LS, Poyser C, Fairweather-Schmidt K. Maternal perinatal anxiety: a review of prevalence and correlates. Clin Psychologist. 2017;21(1):4-19.
- Farr SL, Dietz PM, O’Hara MW, et al. Postpartum anxiety and comorbid depression in a population-based sample of women. J Womens Health. 2014;23(2):120-128.
- Cena L, Palumbo G, Mirabella F, et al. Perspectives on early screening and prompt intervention to identify and treat maternal perinatal mental health. Protocol for a prospective multicenter study in Italy. Front Psychol. 2020;11:365.
- Biaggi A, Conroy S, Pawlby S, Pariante CM. Identifying the women at risk of antenatal anxiety and depression: a systematic review. J Affect Disord. 2016;191:62-77.
- Zadeh MA, Khajehei M, Sharif F, Hadzic M. High-risk pregnancy: effects on postpartum depression and anxiety. Br J Midwifery. 2012;20(2):104-113.
- Rados SN, Tadinac M, Herman R. Anxiety during pregnancy and postpartum: course, predictors and comorbidity with postpartum depression. Acta Clin Croat. 2018;57(1):39-51.
- Fairbrother N, Janssen P, Antony MM, et al. Perinatal anxiety disorder prevalence and incidence. J Affect Disord. 2016;200:148-155.
- American Psychiatric Association. Anxiety disorders. In: Diagnostic and Statistical Manual of Mental Disorders, 5th ed. Arlington, VA: American Psychiatric Association; 2013:222-226.
- Hoang S. Pregnancy and anxiety. Int J Childbirth Educ. 2014;29(1):67-70.
- American College of Obstetricians and Gynecologists Committee Opinion No. 630. Screening for perinatal depression. Obstet Gynecol. 2015;125(5):1268-1271.
- Accortt EE, Wong MS. It is time for routine screening for perinatal mood and anxiety disorders in obstetrics and gynecology settings. Obstet Gynecol Surv. 2017;72(9):553-568.
- Brunton RJ, Dryer R, Saliba A, Kohlhoff J. Pregnancy anxiety: a systematic review of current scales. J Affect Disord. 2015;176:24-34.
- Spitzer RL, Kroenke K, Williams JBW, Löwe B. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092-1097.
- Simpson W, Glazer M, Michalski N, et al. Comparative efficacy of the generalized anxiety disorder 7-item scale and the Edinburgh Postnatal Depression Scale as screening tools for generalized anxiety disorder in pregnancy and the postpartum period. Can J Psychiatry. 2014;59(8):434-440.
- Somerville S, Dedman K, Hagan R, et al. The perinatal anxiety screening scale: development and preliminary validation. Arch Womens Ment Health. 2014;17(5):443-454.
- Somerville S, Byrne SL, Dedman K, et al. Detecting the severity of perinatal anxiety with the Perinatal Anxiety Screening Scale (PASS). J Affect Disord. 2015;186:18-25.
- Fairbrother N, Corbyn B, Thordarson DS, et al. Screening for perinatal anxiety disorders: room to grow. J Affect Disord. 2019;250:363-370.
- Wenzel A, Haugen EN, Jackson LC, Robinson K. Prevalence of generalized anxiety at eight weeks postpartum. Arch Womens Ment Health. 2002;6(1):43-49.
- Moran TE, Polanin JR, Wenzel A. The Postpartum Worry Scale-Revised: an initial validation of a measure of postpartum worry. Arch Womens Ment Health. 2014;17(1):41-48.
- Moran TE, Polanin JR, Segre L, Wenzel A. The Postpartum Worry Scale-Revised: continuing validation with a sample of NICU mothers. Arch Womens Ment Health. 2015;18(2):221-228.
- Yao B, Sripada RK, Klumpp H, et al. Penn State Worry Questionnaire-10: a new tool for measurement-based care. Psychiatry Res. 2016;239:62-67.
- Matthey S, Fisher J, Rowe H. Using the Edinburgh Postnatal Depression Scale to screen for anxiety disorders: conceptual and methodological considerations. J Affect Disord. 2013;146(2):224-230.
- Fallon V, Halford JCG, Bennett KM, Harrold JA. The Postpartum Specific Anxiety Scale: development and preliminary validation. Arch Womens Ment Health. 2016;19(6):1079-1090.
- Ali NS, Azam IS, Ali BS, et al. Frequency and associated factors for anxiety and depression in pregnant women: a hospital-based cross-sectional study. Scientific World J. 2012;2012:653098.
- Dunkel Schetter C, Tanner L. Anxiety, depression and stress in pregnancy: implications for mothers, children, research, and practice. Curr Opin Psychiatry. 2012;25(2):141-148.
- Otte C. Cognitive behavior therapy in anxiety disorders: current state of the evidence. Dialogues Clin Neurosci. 2011;13(4):413-421.
- Sockol LE, Epperson CN, Barber JP. A meta-analysis of treatments for perinatal depression. Clin Psychol Rev. 2011;31(5):839-849.
- Stuart S, Koleva H. Psychological treatments for perinatal depression. Best Pract Res Clin Obstet Gynaecol. 2014;28(1):61-70.
- Kittel-Schneider S, Reif A. Treatment of mental disorders in pregnancy and lactation: psychotherapy and other non-drug therapies. Neurologist. 2016;87(9):967-973.
- Taylor BL, Cavanagh K, Strauss C. The effectiveness of mindfulness-based interventions in the perinatal period: a systematic review and meta-analysis. PLoS One. 2016;11(5):e0155720.
- Fischer Fumeaux CJ, Morisod Harari M, Weisskopf E, et al. Risk-benefit balance assessment of SSRI antidepressant use during pregnancy and lactation based on best available evidence – an update. Expert Opin Drug Saf. 2019;18(10):949-963.
- Weisskopf E, Fischer CJ, Bickle Graz M, et al. Risk-benefit balance assessment of SSRI antidepressant use during pregnancy and lactation based on best available evidence. Expert Opin Drug Saf. 2015:14(3);413-427.
- Bérard A, Sheehy O, Zhao JP, et al. SSRI and SNRI use during pregnancy and the risk of persistent pulmonary hypertension of the newborn. Br J Clin Pharmacol. 2017;83(5):1126‐1133.
- Bérard A, Zhao JP, Sheehy O. Antidepressant use during pregnancy and the risk of major congenital malformations in a cohort of depressed pregnant women: an updated analysis of the Quebec Pregnancy Cohort. BMJ Open. 2017;7(1):e013372.
- Gao SY, Wu QJ, Sun C, et al. Selective serotonin reuptake inhibitor use during early pregnancy and congenital malformations: a systematic review and meta-analysis of cohort studies of more than 9 million births. BMC Med. 2018;16(1):205.
- Ekc AC, Saccone G, Beghella V. Selective serotonin reuptake inhibitor (SSRI) use during pregnancy and risk of preterm birth: a systematic review and meta‐analysis. BJOG. 2016;123(12):1900-1907.
- Ng QX, Venkatanarayanan N, Ho CYX, et al. Selective serotonin reuptake inhibitors and persistent pulmonary hypertension of the newborn: an update meta-analysis. J Womens Health (Larchmt). 2019;28(3):331‐338.
- Stahl S. Prescriber’s Guide: Stahl’s Essential Psychopharmacology. 6th ed. New York, NY: Cambridge University Press; 2017.
- Drugs and Lactation Database (LactMed): Bethesda, MD: National Library of Medicine: 2006-. https://www.ncbi.nlm.nih.gov/books/NBK501922/?report=classic.
- Van Damme R, Van Parys A-S, Vogels C, et al. A mental health care protocol for the screening, detection and treatment of perinatal anxiety and depressive disorders in Flanders. J Psychosom Res. 2020;128:109865.
- Smith T, Gemmill AW, Milgrom J. Perinatal anxiety and depression: awareness and attitudes in Australia. Int J Soc Psychiatry. 2019;65(5):378-387.
- Lemmens GMD, Von Parys A-S, Vogels C, Roelens K. Early detection and treatment of perinatal mental health disorders: a perinatal health care protocol. J Psychosomatic Res. 2019;121:151.
- Kendig S, Keats JP, Hoffman MC, et al. Consensus bundle on maternal mental health: perinatal depression and anxiety. Obstet Gynecol. 2017:129(3):422-430.
- Gjerde LC, Eilertsen EM, Eley TC, et al. Maternal perinatal and concurrent anxiety and mental health problems in early childhood: a sibling-comparison study. Child Dev. 2020;91(2):456-470.
- Hoffman C, Dunn DM, Njoroge WFM. Impact of postpartum mental illness upon infant development. Curr Psychiatry Rep. 2017;19(12):100.
- Ravid E, Salzer L, Arnon L, et al. Is there an association between maternal anxiety propensity and pregnancy outcomes? BMC Pregnancy Childbirth. 2018;18(1):287.