
Faculty:
Susan Hoffstetter, PhD, WHNP-BC, FAANP, is a professor at Saint Louis University School of Medicine, Department of Obstetrics, Gynecology & Women’s Health, Division of Uro-Gynecology, in St. Louis, Missouri.
Intended audience: This continuing education (CE) activity has been designed to meet the educational needs of nurse practitioners who provide care for menopausal and postmenopausal women.
CE approval period: Now through June 30, 2019 Estimated time to complete this activity: 1 hour CE approval hours: 1.0 contact hour of CE credit and 1.0 con-tact hour of Pharmacology credit
 Goal statement: To initiate the conversation with patients about genitourinary syndrome of menopause (GSM) and postmenopausal dyspareunia so that the problem can be identified and treated according to each woman’s needs, desires, and preferences—with the goal of improving her quality of life.
Goal statement: To initiate the conversation with patients about genitourinary syndrome of menopause (GSM) and postmenopausal dyspareunia so that the problem can be identified and treated according to each woman’s needs, desires, and preferences—with the goal of improving her quality of life.
Needs assessment: This activity for Women’s Healthcare is based on a CE presentation developed by the NPWH Education Committee and presented at the NPWH annual conference held in Seattle, Washington, in October 2017. In this article on managing postmenopausal dyspareunia, the author guides women’s healthcare providers in starting the conversation to identify the problem, performing an evaluation to confirm the presence of an underlying cause—most likely GSM—and implementing an individually tailored approach to diminish both the GSM symptoms and the resulting dyspareunia.
Educational objectives: At the conclusion of this educational activity, participants should be able to:
- Query and counsel patients who may experience GSM or vulvovaginal atrophy and moderate-to-severe dyspareunia.
- Describe currently available options, including nondrug therapies and hormonal therapies, for management of moderate to severe dyspareunia.
- Select the most appropriate treatment option for each individual woman based on her health history, needs, desires, and preferences.
Accreditation statement: This activity has been evalu-ated and approved by the Continuing Education Approval Program of the National Association of Nurse Practitioners in Women’s Health (NPWH), and has been approved for 1.0 contact hour of CE credit and 1.0 contact hour of Pharmacology credit.
Faculty disclosures: NPWH policy requires all faculty to disclose any affiliation or relationship with a commercial interest that may cause a potential, real, or apparent conflict of interest with the content of a CE program. NPWH does not imply that the affiliation or relationship will affect the content of the CE program. Disclosure provides participants with information that may be important to their evaluation of an activity. Faculty are also asked to identify any unlabeled/unapproved uses of drugs or devices made in their presentation. Susan Hoffstetter, PhD, WHNP-BC, FAANP, has no actual or potential conflicts of interest in relation to this presentation.
Disclosure of unlabeled use: NPWH policy requires authors to disclose to participants when they are presenting information about unlabeled use of a commercial product or device or an investigational use of a drug or device not yet approved for any use.
Disclaimer: Participating faculty members determine the editorial content of the CE activity; this content does not necessarily represent the views of NPWH. This content has undergone a blinded peer review process for validation of clinical content. Although every effort has been made to ensure that the information is accurate, clinicians are responsible for evaluating this information in relation to generally accepted standards in their own communities and integrating the information in this activity with that of established recommendations of other authorities, national guidelines, FDA-approved package inserts, and individual patient characteristics.
Successful completion of the activity: Successful com-pletion of this activity, J-18-02, requires participants to:
- Log on to npwh.org/courses/home/details/1062 and “Sign In” at the top right-hand corner of the page if you have an NPWH account. You must be signed in to receive credit for this course. If you do not remember your username or password, please follow the “Forgot Password” link and instructions on the sign-in page. If you do not have an account, please click on “Create an Account.”*
- Read the learning objectives, disclosures, and disclaimers on the previous page.
- Study the material in the learning activity during the approval period (now through June 30, 2019).
- Complete the post-test and evaluation. You must earn a score of 70% or better on the post-test to receive CE credit.
- Print out the CE certificate if successfully completed.
*If you are an NPWH member, were once a member, or have taken CE activities with NPWH in the past, you have a username and password in our system. Please do not create a new account. Creation of multiple accounts could result in loss of CE credits as well as other NPWH services. If you do not remember your username or password, please either click on the “Forgot Username” or “Forgot Password” link or call the NPWH office at (202) 543-9693, ext. 1.
Commercial support:The content for this article was supported by an educational grant from AMAG Pharmaceuticals.
Many women experiencing postmenopausal dyspareunia do not mention it at routine office visits. In this article, the author guides women’s healthcare providers in starting the conversation to identify the problem, performing an evaluation to confirm the presence of an underlying causemost likely genitourinary syndrome of menopause (GSM)—and implementing an individually tailored approach to diminish both GSM symptoms and the resulting dyspareunia.
As women reach menopause and beyond, declining levels of estrogen lead many of them to experience genitourinary syndrome of menopause (GSM). GSM is manifested in part by vulvovaginal atrophy (VVA) symptoms that can result in painful sexual intercourse, or dyspareunia. This article provides an overview of GSM, covers the impact of GSM on quality of life (QOL), guides women’s healthcare providers (HCPs) in starting the conversation about GSM and its effects with patients, reviews the patient evaluation process, and helps HCPs select the most appropriate option(s) for women seeking treatment for postmenopausal dyspareunia. Many options for improving GSM symptoms and dyspareunia exist—options that can be individu-ally tailored to each woman’s goals, needs, and desires and even take into account her budget and comfort zone.
Overview of GSM
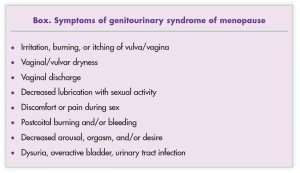
About 50% of postmenopausal women report experiencing GSM,1,2 defined as a collection of signs and symptoms associated with a decrease in estrogen and other sex-steroid hormones that leads to changes in the lower reproductive tract (i.e., labia majora/minora, clitoris, vestibule, introitus, and vagina) and the lower urinary tract (i.e., urethra, bladder).1 GSM symptoms, listed in the Box, progress with increasing age and time from menopause and are unlikely to resolve without intervention.
In terms of the vulvovaginal region in particular, estrogen loss leads to thinning and drying of vulvar tissue; graying and gradual loss of pubic hair; atrophy of the prepuce of the clitoris, exposing the glans clitoris; diminution of the labia minora; narrowing and loss of elasticity of the vaginal walls, making them more friable, with petechiae sometimes noted; shortening and constriction of the vaginal canal; a reduction of glandular secretions; and an increase in vaginal pH, which affects the microbiome of the vagina.
In addition to estrogen loss, other factors can play a role in precipitating or exacerbating GSM. Such factors include smoking, nulliparity, lack of sexual activity, poor overall health, certain physical diseases (e.g., diabetes, cancer), certain mental illnesses (e.g., anxiety, depression), use of certain medications/ substances (e.g., opioids, alcohol, selective serotonin reuptake inhibitors), and loss/absence of a sex partner.
Symptoms of GSM, specifically those related to VVA, are associated with a diminution in QOL, including the quality of a woman’s sexual activities and relationships.
- A cross-sectional Internet survey of more than 7,000 women from the United States or Western Europe showed that VVA symptoms were associated with clinically meaningful decrements in QOL that were similar to those experienced by women with arthritis, chronic obstructive pulmonary disease, asthma, or irritable bowel syndrome.3
- In Women’s Voices in the Menopause, a slightly smaller survey (N = 4,246) that also included Canadian women and that was conducted by interview, 52% of participants reported that VVA symptoms had at least some degree of adverse impact on their sex life, self-esteem, marriage/relationship, and/or social life; 38% reported that their discomfort had not affected them much; and 32% reported that vaginal discomfort made them feel old and diminished their QOL.4
- A survey of British women who took a sexual health survey on a menopause website (N = 1,002) showed that 53% reported vaginal discomfort.5 Despite this discomfort, only 20% discussed it with an HCP. In terms of managing symptoms, 12% were using a prescribed treatment, 24% were using an over-the-counter (OTC) treatment, and 64% were doing nothing. In addition, 61% of the women hid their vaginal dryness/ discomfort from their partner, 42% made excuses to avoid intercourse, and 60% reported losing confidence in themselves because of their symptoms.
- The CLOSER (CLarifying Vaginal Atrophy’s Impact On SEx and Relationships) survey of 4,100 women and 4,100 men from the United States, Canada, and Western Europe evaluated the impact of VVA on physical and emotional aspects of sexual relationships between postmenopausal women and their male partners.6 Among the women, 28% did not tell their partners when they first encountered vaginal discomfort, mainly because they thought it was just a natural part of growing older or because they were embarrassed. Main adverse consequences of VVA were having sex less often, having less satisfying sex, and putting off having sex.
- A U.S. study of an ethnically diverse group of women (N = 745) who completed the DIVA (Day-to-Day Impact of Vaginal Aging) questionnaire showed that among those who reported vaginal dryness (76%), itching (43%), irritation (29%), or soreness (14%) and/or dyspareunia (30%), 64%81% were a little bit bothered or moderately bothered by these symptoms.7
- The REVIVE (REal Women’s Views of Treatment Options for Menopausal Vaginal ChangEs) survey, completed by more than 3,000 postmenopausal U.S. women, revealed that VVA symptoms reduced their enjoyment of sex (59%) and interfered with their sleep (24%), enjoyment of life (23%), and/or mood (23%).8 Most women did not know that VVA symptoms could be caused by menopause or hormonal changes. Almost half had never discussed their symptoms with an HCP. Although 40% of the women with VVA symptoms said they expected their HCP to ask them about their symptoms, the HCP initiated the conversation only 13% of the time. Likewise, only 19% of the women reported being asked about sexual health during a routine office visit. The most common reasons for not mentioning VVA symptoms to HCPs were the assumption that they were a natural part of aging or that they were not bothersome enough at the time. Other reasons for failure to mention the problem included embarrassment, a belief that menopause-related changes were irreversible, and lack of awareness about available treatments.
Starting the conversation
Results of these surveys and questionnaires suggest that women need much more information about GSM, VVA, and dyspareunia, and that HCPs need to be the ones providing this information. HCPs can start by saying Menopause can bring unexpected changes for many women with regard to their sex life, bladder function, or comfort of the vaginal and vulvar skin, and then asking questions such as the following:
- Do you feel dry in the vulvovaginal area?
- Do you experience pain when you’re having sex?
- Are you satisfied with your sexual functioning?
- Do you have any urinary symptoms?
- Do you tend to get urinary tract infections associated with sex? Do you wear pads for urine leakage?
- Do you ever leak urine during sex?
- Do you have a health condition that might affect your quality of life, your sex life, or your vulvovaginal skin or sensations?
HCPs should phrase these questions in ways that take into account each woman’s level of understanding, language/cultural background, and comfort zone.
The PLISSIT model can be used to determine the different levels of intervention for each patient9
- Permission: Validate her concerns and encourage her to talk about her concerns.
- Limited Information: Once a concern has been identified, offer targeted information about it.
- Specific Suggestions: Focus treatment on her goals and/or most bothersome concern.
- Intensive Therapy: If indicated, refer her to a specialist (e.g., sex therapist, pelvic floor physical therapist).
Examination
Pelvic examination of a postmenopausal woman who reports pain during intercourse should start with inspection of the vulvovaginal and urethral areas, followed by a Q-tip test to localize and quantify the pain. The HCP should check for provoked pain in a systematic fashion, starting at the inner thigh. The cotton tip is pressed gently enough to dent the surface 1 mm; the patient’s pain level (0-10 on a Likert-type scale) and superficial muscle responses are noted. The HCP proceeds to test the labia majora, labia minora, clitoris and hood, perineum, and vestibule to delineate areas of tenderness.
 Next, the HCP should perform a speculum exam. Physical findings in a woman with GSM may include erythema and thinning of vulvovaginal tissues; urethral caruncle; labia minora resorption; loss of rugae and hymenal remnants; decreased moisture and elasticity; and tissue fragility, fissures, and petechiae. Wet mount findings will likely include vaginal pH >5.0, increased parabasal cells, and decreased superficial cells.
Next, the HCP should perform a speculum exam. Physical findings in a woman with GSM may include erythema and thinning of vulvovaginal tissues; urethral caruncle; labia minora resorption; loss of rugae and hymenal remnants; decreased moisture and elasticity; and tissue fragility, fissures, and petechiae. Wet mount findings will likely include vaginal pH >5.0, increased parabasal cells, and decreased superficial cells.
If signs of GSM-related changes are noted on the exam, the HCP can use these physical findings as the starting point for questions about GSM symptoms and dyspareunia, which the patient may have denied when her history was taken. The proactive HCP can say, During the pelvic exam, I noticed [fill in the blank]. So I am wondering whether you might be feeling some vaginal dryness or discomfort. And maybe, as a result, you might be experiencing pain during sex, upon entry and/or with deep penetration. Because of the trusting patient–HCP relationship that has been established, the woman may feel comfortable in confiding that, yes, she is having pain with intercourse. The HCP can use the Marinoff Scale to categorize the dyspareunia as follows: 0 = no pain with intercourse; 1 = pain with intercourse that does not preclude its completion; 2 = pain with intercourse that requires interruption or discontinuation; and 3 = pain with intercourse so intense that the act is not performed at all.10
Of note, dyspareunia may be caused or aggravated by the presence of other diagnoses. These entities, which must be ruled out or identified and treated, include vulvar dystrophies (e.g., lichen sclerosus, lichen planus), vulvodynia, vestibulodynia, vaginismus, pelvic floor muscle (PFM) dysfunction, pelvic organ prolapse, overactive bladder, and interstitial cystitis.
Management of postmenopausal dyspareunia
Goals of management are to relieve GSM symptoms, facilitate sexual activity according to the woman’s desires, and improve quality of life. In all cases, a woman’s specific preferences determine the goals.
Initial treatment
For some women, the source of dyspareunia may be as simple as irritation resulting from use of perfumed soaps. Therefore, the first step—for these women and, in fact, for nearly all women—is to implement a protective skin-care routine. Women should use fragrance-free, hypoallergenic products and avoid use of potential irritants, including feminine washes, perineal wipes, and even certain types of toilet paper.
If irritant avoidance is insufficient in resolving dyspareunia and a woman wants to continue or resume sexual activity—which itself has vulvovaginal health-promoting effects—she has several inexpensive options that are available on grocery store and drugstore shelves or on Internet websites. For example, she can try using a lubricant immediately before and/or during sex. Lubricants, the effects of which are temporary, reduce vaginal tissue irritation due to friction. OTC lubricants are available in oil-, water-, and silicone-based liquid or gel formulations. Although these products are generally safe, the woman should be advised that some of them contain ingredients that may themselves induce dermatologic reactions.
Moisturizers differ from lubricants in that they are applied internally at regular intervals and are longer acting. They are made of bioadhesive polymers and are designed to provide long-term relief of vaginal dryness11; they need not be reapplied before sexual intercourse. OTC oil-, water-, and silicone-based moisturizers are available. If a woman’s symptoms persist after using lubricants and moisturizers and she is still looking to avoid pain during sex, then HCPs should focus on reversing her VVA-related changes.
Hormonal treatments
Formulations in this category include vaginal estrogen therapy (ET) and two non-estrogen therapies, oral ospemifene and intravaginal dehydroepiandrosterone (DHEA), also known as prasterone. Of note, black cohosh has no estrogenic effects on the vagina and is not recommended as a treatment for GSM-related dyspareunia.
Vaginal estrogen therapy
Vaginal ET is FDA approved and preferred over systemic ET as first-line therapy for GSM symptoms.12Vaginal ET preparations, which are quite expensive, include creams, tablets, and rings containing estradiol or conjugated equine estrogens. Creams and tablets are used twice weekly; the ring is changed every 3 months. Vaginal ET restores the genitourinary tract anatomy, increases superficial vaginal cells, reduces vaginal pH, and treats symptoms of VVA. According to The North American Menopause Society (NAMS), vaginal ET decreases sexual dysfunction, including dyspareunia, by increasing lubrication, blood flow, and sensation in vaginal tissues.12
In addition to their efficacy, lowdose vaginal ET products are generally safe; users’ blood estrogen levels remain in the postmenopausal range. At the same time, the prescribing information for these products carries the standard black-box warnings for estrogen-alone and estrogen-progestogen treatment risks. HCPs should prescribe the lowest vaginal ET dose for the shortest duration, consistent with a woman’s treatment goals and risk profile. Although progestogen therapy is not necessarily needed with low-dose vaginal ET to protect the uterus, randomized clinical trial data are lacking beyond 1 year; postmenopausal bleeding in women using low-dose vaginal ET must be thoroughly evaluated.12
Because of a potential risk for small increases in circulating estrogens, the decision to use low-dose vaginal ET in a woman with breast cancer is made in conjunction with her oncologist.12 This recommendation is particularly important for a woman using an aromatase inhibitor (AI) with suppressed plasma levels of estradiol, although no increased risk was seen in an observational trial of breast cancer survivors using tamoxifen or an AI with low-dose vaginal ET over a mean follow-up of 3.5 years.13
Ospemifene
Ospemifene is a selective estrogen receptor modulator approved for the treatment of dyspareunia associated with GSM.14This estrogen agonist/antagonist has tissue-selective effects, including a nearly full estrogen agonist effect on the vaginal epithelium, while having neutral to slight estrogenic effects on the endometrium.14 Ospemifene should not be taken with any form of ET or other estrogen agonist/antagonist because the safety of concomitant use of ospemifene with either of these agents has not been studied.15Because ospemifene has mild estrogenic effects on the endometrium, concurrent use of a progestogen to protect the uterus should be considered in nonhysterectomized women to reduce the risk for endometrial cancer.15 Of note, the use of progestogens with ospemifene therapy was not evaluated in clinical trials conducted prior to its approval.
Ospemifene, taken orally at a dosage of 60 mg/day, has been shown to improve sexual function significantly, specifically in the domains of sexual pain, arousal, and desire, in symptomatic women.16 This medication should be taken with food, which increases its bioavailability by 2- to 3-fold. The most common side effects of ospemifene are hot flushes, vaginal discharge, muscle spasms, and increased sweating.17 Ospemifene’s prescribing information includes a black-box warning about increased risk for endometrial cancer and cardiovascular adverse events (stroke and deep venous thrombosis).
Prasterone
Intravaginal DHEA, or prasterone, is an inactive endogenous steroid converted locally inside the vaginal cells into active androgens and estrogens. This once-daily vaginal suppository containing prasterone 6.5 mg is approved to treat moderate to severe dyspareunia related to GSM.18 The prescribing information for this product has no black-box warnings.19 The main side effect is vaginal discharge related to melting of the suppository.
Daily intravaginal prasterone treatment has been shown to exert clinically and statistically significant beneficial effects on the four co-primary objectives of VVA treatment: a decrease in the percentage of vaginal parabasal cells, an increase in the percentage of vaginal superficial cells, a decrease in vaginal pH, and a reduction in the severity of dyspareunia.20 In a study by Archer et al,20 gynecologic evaluation showed that prasterone users experienced improvements in vaginal secretions, epithelial integrity, epithelial surface thickness, and color. Serum steroid concentrations remain within postmenopausal levels. Consistent with the strictly local action of treatment, no major prasterone-related adverse effects have been reported.
Other treatment options
Therapies that can be used in addition to or instead of hormone treatment include vaginal dilators, pelvic floor physical therapy (PT), and laser treatment (experimental for this indication).
According to NAMS, gentle stretching of the vagina with the use of lubricated vaginal dilators of graduated sizes can help restore and maintain vaginal function.21 Re-initiating regular sexual activity once vaginal penetration is comfortable will help maintain vaginal health.21 Similarly, a vibrator can be used therapeutically to stimulate blood flow and maintain vaginal function in women with or without a partner.22
Pelvic floor PT, ideally provided by a physical therapist with specialized training in pelvic floor disorders, may be useful in women with non-relaxing or high-tone PFM dysfunction triggered by painful sexual activity related to GSM.22This treatment entails PFM awareness/training and the use of biofeedback. Efficacy of this approach was shown in an Italian study of 206 postmenopausal women with GSM who received intravaginal estriol, alone or with pelvic floor PT.23 In an individual case study, a 77-year-old woman with GSM-related dyspareunia showed improvement in symptoms and the quality of her sex life following the addition of a 12-week course of pelvic floor PT to her vaginal ET regimen.24
The FDA has approved fractional laser treatment for “incision, excision, ablation, vaporization, and coagulation of body soft tissues in medical specialties, including aesthetics, dermatology, plastic surgery, podiatry, ENT, gynecology, neurosurgery, dental oral surgery and genitourinary surgery,” but not as a treatment for VVA.25 Laser therapy stimulates production of collagen to create healthier skin. Preliminary observational data have shown some potential benefits with the use of this technology in treating patients with VVA, but additional data are needed to further assess the efficacy and safety of this procedure for this indication. The series of laser treatments that are needed are expensive and are not covered by health insurance.
Conclusion
Postmenopausal women who are experiencing GSM-related dyspareunia and who want to resume sexual intercourse have a variety of therapeutic options. If initial conservative measures such as the use of lubricants and/or moisturizers are insufficient, they can try a hormonal treatment such as vaginal ET, oral ospemifene, or intravaginal prasterone. They can consider adjunctive therapies such as graduated dilators and pelvic floor PT. Women’s HCPs can initiate the conversation about postmenopausal dyspareunia with their patients, who may not feel comfortable broaching the topic, and they can educate them about the problem, evaluate them, and offer them a treatment that is individually tailored to their goals, needs, desires, cultural background, and comfort zone.
References
- Portman DJ, Gass ML; Vulvovaginal Atrophy Terminology Consensus Conference Panel. Genitourinary syndrome of menopause: new terminology for vulvovaginal atrophy from the International Society for the Study of Women’s Sexual Health and The North American Menopause Society. Menopause. 2014;21(10):1063-1068.
- Parish SJ, Nappi RE, Krychman ML, et al. Impact of vulvovaginal health on postmenopausal women: a review of surveys on symptoms of vulvovaginal atrophy. Int J Womens Health. 2013;5:437-447.
- DeBonaventura M, Luo X, Moffatt M, et al. The association between vulvovaginal atrophy symptoms and quality of life among postmenopausal women in the United States and Western Europe. J Womens Health (Larchmt).2015;24(9):713-722.
- Nappi RE, Kokot-Kierepa M. Women’s voices in the menopause: results from an international survey on vaginal atrophy. Maturitas. 2010;67(3):233-238.
- Cumming GP, Herald J, Moncur R, et al. Women’s attitudes to hormone replacement therapy, alternative therapy and sexual health: a web-based survey. Menopause Int. 2007;13(2):79-83.
- Nappi RE, Kingsberg S, Maamari R, Simon J. The CLOSER (CLarifying Vaginal Atrophy’s Impact On SEx and Relationships) survey: implications of vaginal discomfort in postmenopausal women and in male partners. J Sex Med. 2013;10(9):2232-2241.
- Huang AJ, Gregorich SE, Kuppermann M, et al. Day-to-Day Impact of Vaginal Aging questionnaire: a multidimensional measure of the impact of vaginal symptoms on functioning and well-being in postmenopausal women. Menopause. 2015;22(2):144-154.
- Kingsberg SA, Wysocki S, Magnus, L, Krychman ML. Vulvar and vaginal atrophy in postmenopausal women: findings from the REVIVE (REal Women’s VIews of Treatment Options for Menopausal Vaginal ChangEs) survey. J Sex Med. 2013;10(7):1790-1799.
- Palmisano B. PLISSIT Model: Introducing sexual health in clinical care. Psychiatry Advisor. January 4, 2017.
- Marinoff SC, Turner ML. Vulvar vestibulitis syndrome. Dermatol Clin. 1992;10(2):435-444.
- Faught BM, Kellogg-Spadt S. Sexual enhancers: lubricants, aids, and toys. Womens Healthcare. 2016;4(1):46-48.
- Pinkerton JV, Sánchez Aguirre F, Blake J, et al. The 2017 hormone therapy position statement of The North American Menopause Society. Menopause. 2017;24(7):728-753.
- Le Ray I, Dell Aniello S, Bonnetain F, et al. Local estrogen therapy and risk of breast cancer recurrence among hormone-treated patients: a nested case-control study. Breast Cancer Res Treat. 2012;135(2):603-609.
- DeGregorio MW, Zerbe RL, Wurz GT. Ospemifene: a first-in-class, non-hormonal selective estrogen receptor modulator approved for the treatment of dyspareunia associated with vulvar and vaginal atrophy. Steroids. 2014;90:82-93.
- Osphena prescribing information. Shionogi, Inc. Revised February 2015.
- Constantine G, Graham S, Portman DJ, et al. Female sexual function improved with ospemifene in postmenopausal women with vulvar and vaginal atrophy: results of a randomized, placebo-controlled trial. Climacteric. 2015;18(2):226-232.
- MedlinePlus. Ospemifene. February 15, 2017.
- Prasterone (Intrarosa) for dyspareunia. Med Lett Drugs Ther. 2017;11(1529):149-150.
- Prasterone prescribing information. AMAG Pharmaceuticals, Inc. April 2017.
- Archer DF, Labrie F, Bouchard C, et al; VVA Prasterone Group. Treatment of pain at sexual activity (dyspareunia) with intravaginal dehydroepiandrosterone (prasterone). Menopause. 2015;22(9):950-963.
- Management of symptomatic vulvovaginal atrophy: 2013 position statement of The North American Menopause Society. Menopause. 2013;20(9):888-902.
- Faubion SS, Sood R, Kapoor E.Genitourinary syndrome of menopause: management strategies for the clinician. Mayo Clin Proc. 2017;92(12):1842-1849.
- Capobianco G, Donolo E, Borghero G, et al. Effects of intravaginal estriol and pelvic floor rehabilitation on urogenital aging in postmenopausal women. Arch Gynecol Obstet. 2012;285(2):397- 403.
- Mercier J, Morin M, Lemieux MC, et al. Pelvic floor muscles training to reduce symptoms and signs of vulvovaginal atrophy: a case study. Menopause. 2016;23(7):816-820.
- American College of Obstetricians and Gynecologists and the American Congress of Obstetricians and Gynecologists. Position Statement. Fractional Laser Treatment of Vulvovaginal Atrophy and U.S. Food and Drug Administration Clearance. May 2016.