
The authors discuss how to determine who is a candidate for bone densitometry, interpret the results, ascertain when treatment is indicated, and choose among various treatment options.
CASE PRESENTATIONS
You see a 70-year-old mother and her 50-year-old daughter in your practice. You order bone density scans for each of them. Although the scans show that each woman has a T-score of –2.3 at the femoral neck, you will be treating only the older woman with medication.
The daughter underwent a total abdominal hysterectomy 6 months previously and was started on estrogen therapy. She has no history of fracture and reports no use of corticosteroids, no smoking, and minimal intake of alcohol. Pertinent physical examination and laboratory findings are:
• Height, 62 inches; weight, 110 lb;
• Hyperextensible joints;
• Small bone structure;
• Tandem gait excellent; and
• Complete blood count (CBC), complete metabolic panel (CMP), vitamin D, parathyroid hormone (PTH), and 24-hour urinary calcium values all within normal limits.
Based on her FRAX® results (more about this tool later), her 10-year fracture risk is 7.3% for a fragility fracture and 0.5% for a hip fracture. You make sure that she has adequate calcium and vitamin D intake through diet and supplements, and you recommend that she engage in activities that maintain her good balance, engage in weight-bearing exercise, and work out with light weights.
The mother fractured her hip 2 years previously after tripping on a dog toy. She reached menopause at age 45 but chose to forgo hormone therapy. She does not take steroids, smoke, or drink alcohol. Her own mother sustained a hip fracture at age 85. Pertinent physical exam and lab findings are:
• Height, 62 inches; weight, 120 lb;
• Flexibility normal;
• Small bone structure;
• Slight limp from hip fracture;
• Tandem gait done with some difficulty; and
• CBC, CMP, vitamin D, PTH, and 24-hour urinary calcium values all within normal limits.
Based on her FRAX results, her 10-year fracture risk is 35% for a fragility fracture and 14% for a hip fracture. History of a hip fracture alone merits osteoporosis treatment. You recommend adequate calcium and vitamin D intake through diet and supplements, balance training and weight-bearing exercises, and pharmacotherapy with an oral bisphosphonate.
Why did both women undergo bone density scans? And, given the fact that mother and daughter got the same T-score, why is the mother, but not the daughter, a candidate for pharmacotherapy? Some background information is needed to answer these questions.
Osteoporosis is a skeletal disease characterized by low bone mass and microarchitectural deterioration of the bone tissue, with a consequent increase in bone fragility that increases the risk for fracture.1 Approximately 10 million persons in the United States have osteoporosis and another 44 million have osteopenia (low bone mass that is less severe than osteoporosis), placing them at increased risk for fracture.2 Fifty percent of women experience an osteoporosis-related fracture in their lifetime, an incidence greater than that of myocardial infarction, stroke, and breast cancer combined.2 Of note, especially for healthcare providers (HCPs) who see young female patients, osteoporosis is not just a disease of bone loss, which commonly occurs as people age. Osteoporosis can also develop in people who do not reach peak bone mass during childhood and adolescence—without the accelerated bone loss that can accompany aging.1
Instead of testing bone strength, which is inappropriate in humans, HCPs can check their patients’ bone mineral density (BMD), which accounts for about 70% of bone strength and serves as a proxy measure for it.1 BMD is ascertained most commonly by dual-energy x-ray absorptiometry (DXA) of the hip and spine—or in rare cases, the forearm. DXA is used to establish or confirm a diagnosis of osteoporosis, to help predict future fracture risk, and to monitor patients over time, particularly those undergoing osteoporosis treatment.3, 4
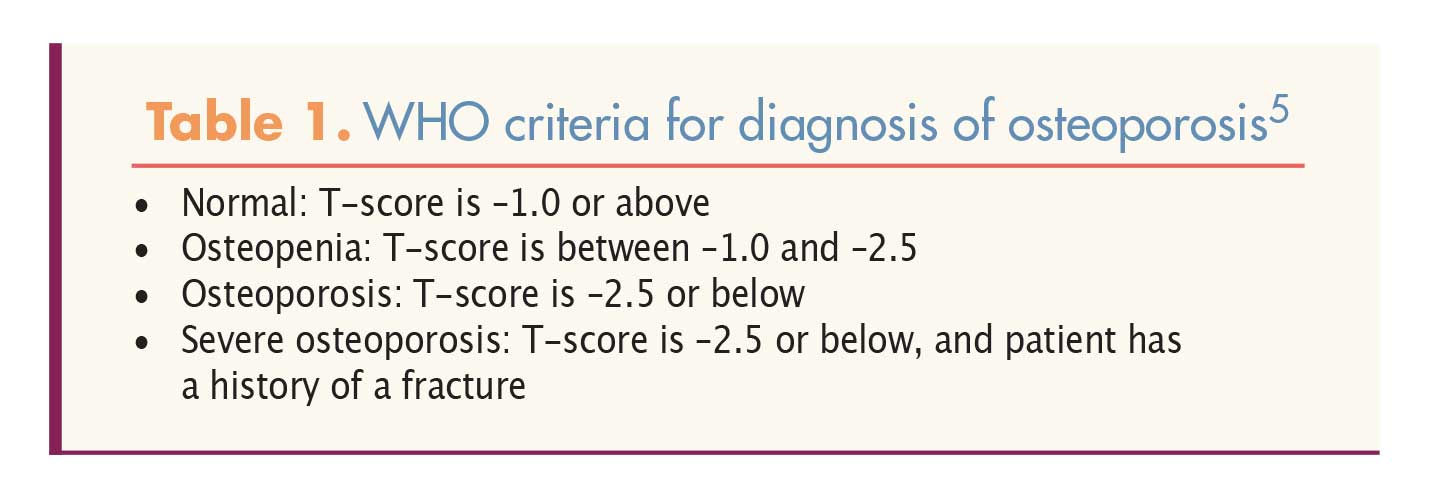
Areal BMD can be expressed in absolute terms of grams of mineral per square centimeter scanned (g/cm2) and as a relationship to two norms: the BMD of a young-adult reference population (T-score) and the BMD of an age-, sex-, and race- or ethnicity-matched reference population (Z-score). T-scores and Z-scores are calculated by determining the difference between a patient’s BMD and the mean BMD of the reference population, divided by the standard deviation (SD) of the reference population. Spine and hip BMD measurements in postmenopausal white women are interpreted using the World Health Organization’s T-score definitions of osteoporosis and osteopenia (Table 1).5
{kind=link}
Osteoporosis is defined clinically as a fragility fracture of the hip or spine in the absence of other metabolic bone disease, a BMD of –2.5 or lower at any location, or a FRAX score indicating a 10-year risk of a major fragility fracture equal to or greater than 20% or a 10-year risk of hip fracture equal to or greater than 3%.6 The Fracture Risk Assessment Tool,7 or FRAX, is a computer-based algorithm that calculates fracture probability from clinical risk factors—age, sex, body mass index, smoking, alcohol use, prior fracture, parental history of hip fracture, corticosteroid use, rheumatoid arthritis (RA), and secondary osteoporosis—and BMD at the femoral neck.8
Fracture
Bone mineral density and fracture risk are inversely related. Each 1 SD decrease in BMD is associated with a 1.6- to 2.6-fold increase in risk of fracture, depending on the skeletal site.9 Along with low BMD, non-skeletal factors—especially the tendency to fall—contribute to fragility fracture risk. About 90% of fragility fractures occur after falls.10 The pathogenesis of falls in older adults is complex and is related to factors such as age-related deficits in visual, proprioception, and vestibular systems; frailty and de-conditioning; health conditions such as neuropathy, or prior stroke; use of certain medications (e.g., hypnotics, antihypertensives) and polypharmacy; and environmental factors (e.g., poor lighting, loose rugs).11, 12
More than 2 million fragility fractures occur each year in the U.S., accounting for $17 billion in healthcare costs.13 Seventy percent of fragility fractures occur in women. Despite these numbers, fewer than 25% of women aged 67 or older with an osteoporosis-related fracture undergo BMD measurement or begin osteoporosis treatment.12
Vertebral fracture, the most common osteoporotic fracture, may occur in the absence of trauma or after minimal trauma (e.g., bending, lifting).14 Although most vertebral fractures are clinically silent at first, they can eventually cause pain, disability, deformity, and mortality.15 Hip fracture, the most serious consequence of osteoporosis,12 is associated with chronic pain and disability, loss of independence, decreased quality of life, and increased mortality—8% to 36%—within a year.4 More than half of hip fracture survivors cannot live independently; many require longterm nursing home care.16
Although for many years there was awareness of the morbidity and mortality associated with fragility fractures, real progress came only with the ability to diagnose osteoporosis before fractures occur and the development of effective treatments.3 Measurement of BMD with DXA, which entered routine clinical practice in the late 1980s, has played a vital role in both of these developments. Although BMD correlates with fracture risk, HCPs should keep in mind that most fractures occur in patients with osteopenia. Therefore, patients with osteoporosis or with osteopenia may need treatment.
Osteoporosis workup
According to guidelines published by the American Association of Clinical Endocrinologists and the American College of Endocrinology (AACE/ACE) in 2016, all postmenopausal women aged 50 years or older should undergo clinical assessment for osteoporosis and fracture risk, starting with a detailed history and physical examination.12 HCPs should check for prior non-traumatic fractures, low body weight (<127 lb), height loss or kyphosis, a family history of osteoporosis and/or fractures, smoking, early-onset menopause, and excessive alcohol intake (3 drinks/day). HCPs should also assess each woman’s risk factors for falling.
The AACE/ACE recommends lateral spine imaging with standard radiography or vertebral fracture assessment (VFA).12 VFA is a method for imaging the thoracic and lumbar spine by DXA for the purpose of detecting vertebral fracture deformities in patients with unexplained height loss, self-reported but undocumented prior spine fractures, or steroid therapy equivalent to 5 mg/day prednisone for 3 months or longer.
The AACE/ACE recommends BMD measurement in women at increased risk for osteoporosis and fractures who are willing to consider pharmacologic treatment if osteopenia or osteoporosis is documented.12 Candidates for BMD measurement include all women aged 65 years or older, as well as younger postmenopausal women who (1) have a history of fracture without major trauma, (2) are on long-term systemic steroids, (3) have radiographic osteopenia, or (4) have clinical risk factors for osteoporosis.12 Three major health organizations—the U.S. Preventive Services Task Force, the National Osteoporosis Foundation (NOF), and the American Congress of Obstetricians and Gynecologists—offer similar screening recommendations.17-19
The AACE/ACE advises that treatment decisions for osteoporosis or osteopenia include consideration of fracture probability.12 Therefore, BMD results should be combined with other clinical risk factors for accurate fracture risk assessment. The FRAX tool can be used to calculate patients’ probability of fracture over 10 years.
In terms of the first question posed at the beginning of this article—Why did both women undergo bone density scans?—the answer is that both the mother and the daughter met criteria for BMD testing: The mother is 70 years old, and the daughter is a 50-year-old postmenopausal woman with low body weight and a mother who sustained a hip fracture.
Management
If postmenopausal osteoporosis is documented based on clinical and imaging fi ndings, HCPs should first ascertain whether it might be secondary to another cause. Certain health conditions that cause or exacerbate bone loss may be asymptomatic and require laboratory testing for detection. Lab tests include a CBC, a CMP, 25-hydroxyvitamin D, PTH, bone-specifi c alkaline phosphatase, and a 24-hour urine collection for calcium and creatinine.12 When indicated, HCPs should address causes of secondary osteoporosis and correct any calcium and/or vitamin D deficiencies. The general approach to management of osteoporosis and osteopenia is as follows:
Nutritional and nonpharmacologic interventions
All women, not just those with low bone mass—should aim for an adequate intake of vitamin D and calcium, participation in weight-bearing and muscle-strengthening exercises, smoking cessation as applicable, minimization of alcohol intake as applicable, and treatment of risk factors for falling. Many scientific organizations recommend an intake of 1,000 IU/day of vitamin D for adults aged 50 or older.12 Serum 25-hydroxyvitamin D levels should be measured in those at risk for vitamin D defi ciency, and vitamin D supplements should be prescribed as needed.4 Adults aged 50 or older are advised to consume 1,200 mg/ day of calcium through diet and a supplement, if needed.20
Measures to reduce falls include individual risk assessment; Tai Chi, yoga for seniors, and other exercise programs; home safety assessment, especially when done by an occupational therapist, and modification as needed; withdrawal of psychotropic medications if possible; and appropriate correction of visual impairment.4 Measures to be taken inside the home include anchoring rugs, minimizing clutter, removing loose wires, using nonskid mats, installing handrails where needed, adding lighting to stairwells and hallways, wearing sturdy shoes, and avoiding potentially dangerous activities.12
Pharmacotherapy
The AACE and NOF strongly recommend pharmacotherapy for persons with:
• Osteopenia and a history of a fragility fracture of the spine or hip;
• A T-score of –2.5 or lower in the spine, femoral neck, total hip, or distal one-third radius; or
• A T-score between –1.0 and –2.5 in the spine, femoral neck, total hip, or distal one-third radius and a 10-year risk of hip fracture equal to or greater than 3% or a 10-year risk of a major osteoporosis-related fracture equal to or greater than 20%.4,12
In terms of the second question posed at the beginning of this article—Why is the mother, but not the daughter, a candidate for pharmacotherapy?—the answer is that the 50-year-old daughter does not meet criteria for pharmacologic intervention; her BMD is in the osteopenia range, but she has no history of fracture and her FRAX scores do not show a high enough 10-year fracture risk to merit treatment. By contrast, the 70-year-old mother has osteopenia, a personal history of fracture, a maternal history of fracture, and FRAX scores that are high enough to warrant treatment.
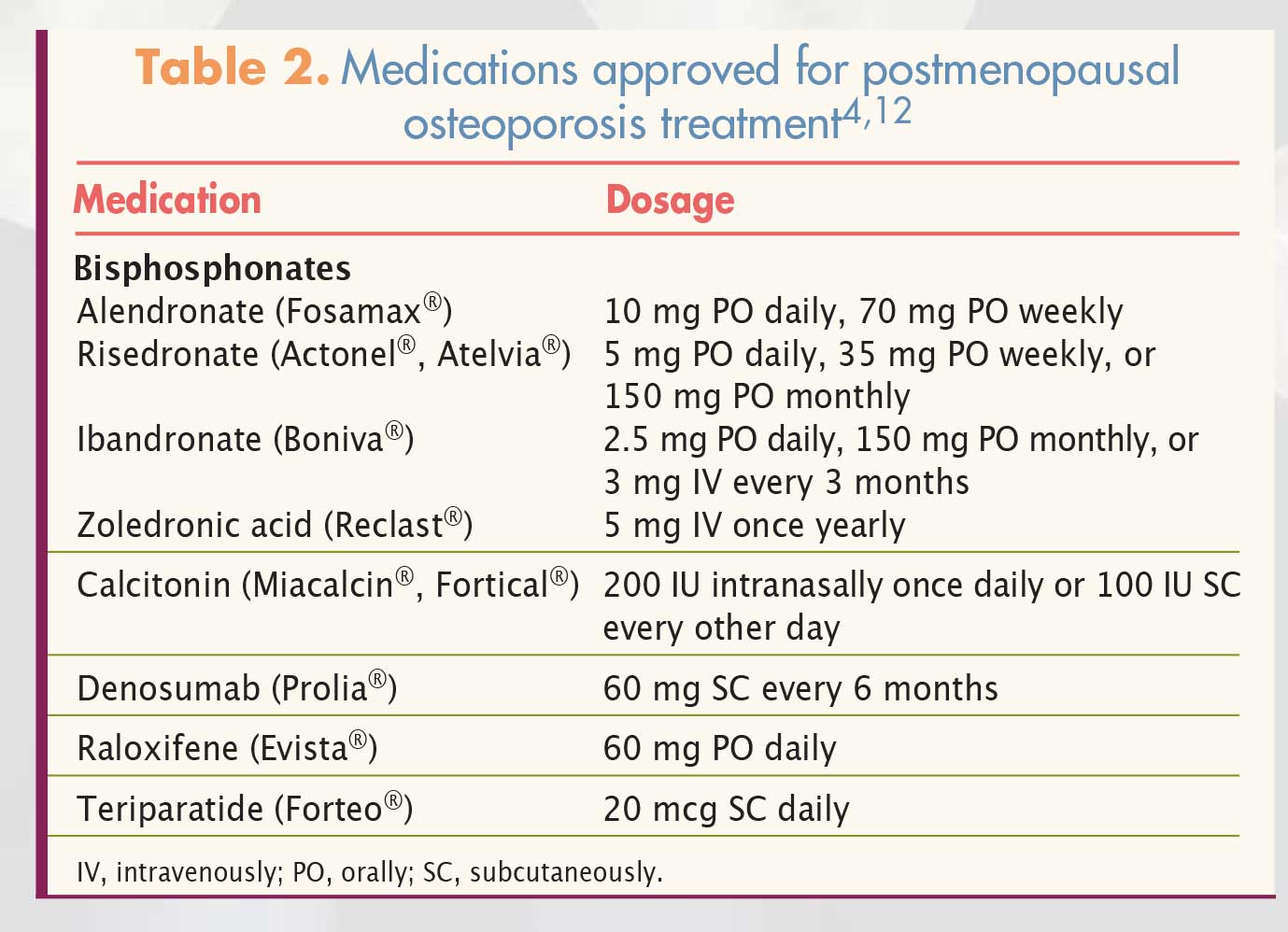
Healthcare providers can choose among a variety of medications (Table 2), depending on patients’ health status and fracture risk.4,12 Four agents—alendronate, risedronate, zoledronic acid, and denosumab—have evidence for “broad spectrum” anti-fracture efficacy and are considered initial options in most cases.
{kind=link}
Patients with moderate fracture risk, but no fragility fractures, can be started on an oral agent—that is, alendronate or risedronate. Patients with the highest fracture risk are usually started on an injectable such as teriparatide, denosumab, or zoledronic acid. The injectables are also appropriate for patients with upper gastrointestinal (GI) problems who might not tolerate oral medications, those with lower GI problems who might not absorb oral medications, and those with difficulty remembering to take oral medications on a regular basis or coordinating an oral bisphosphonate (BP) with other oral medications or their daily routine.
Bisphosphonates
Three of the aforementioned firstline agents, alendronate, risedronate, and zoledronic acid, are BPs; another member of this class is ibandronate. These agents, which are approved for both prevention and treatment of osteoporosis, have proven anti-fracture efficacy as well; on average, they reduce the incidence of vertebral and hip fractures by 50% over 3 years and they may increase BMD. The major downside is that nearly all oral BP products must be taken on an empty stomach and swallowed with a full glass of water, with at least a half hour intervening before anything other than water is ingested. Many BP users report painful swallowing, nausea, heartburn, or esophageal irritation. Other side effects include hypocalemia; bone, joint, or muscle pain; rash/allergy; and renal dysfunction. Presence of hypocalcemia is a contraindication to BP use. BPs should be used with caution, if at all, in patients with reduced renal function.
Two serious, but rare, adverse effects of long-term BP treatment are osteonecrosis of the jaw (ONJ) and atypical fracture of the femur (AFF). Pain in the thigh or groin area, which can be bilateral, often precedes an AFF. To put the risks of ONJ and AFF in perspective, out of 100,000 postmenopausal women, 50,000 will experience an osteoporosis-related fracture. By contrast, out of 100,000 persons on osteoporosis medication for 5 years, 1 may develop ONJ and 16, AFF.21
Calcitonin
Salmon calcitonin is approved for the treatment of osteoporosis in women who are at least 5 years postmenopausal when alternative treatments are not suitable. Calcitonin reduces vertebral fracture occurrence by about 30% in persons with prior vertebral fractures, but it has not been shown to reduce the risk of nonvertebral fractures and it has only a weak effect on BMD. The most common side effects of nasally administered calcitonin are nasal discomfort, rhinitis, and epistaxis.
Raloxifene
Raloxifene, an estrogen agonist/antagonist, is approved for prevention and treatment of postmenopausal osteoporosis, as well as for the reduction of breast cancer risk. Raloxifene is contraindicated in women of childbearing potential and in those with a history of venous thromboembolism (VTE). Raloxifene has been shown to reduce the risk of vertebral fracture (by 30%-55%), but not nonvertebral fracture or hip fracture. Adverse effects of this agent include VTE (a 3-fold increased risk, but the absolute risk is low), menopausal symptoms, and leg cramps.
Of note, estrogen therapy is FDA approved only for osteoporosis prevention, not treatment. Likewise, a medication that combines conjugated estrogens with the estrogen agonist/antagonist bazedoxifene is approved to prevent, not treat, osteoporosis after menopause, as well as to treat moderate to severe vasomotor symptoms.
Denosumab
Denosumab, a fully human monoclonal antibody, is approved for treatment of osteoporosis in postmenopausal women at high risk of fracture. This agent decreases bone resorption, increases BMD, and reduces fracture risk by 20%-70% over 3 years, depending on the site. Given subcutaneously (SC) every 6 months, denosumab must be administered by an HCP. Denosumab may be considered for use in certain patients with renal insuffi ciency; impaired renal function does not signifi cantly alter the metabolism or excretion of the drug.22 Denosumab may cause hypocalcemia, which must be corrected before treatment is started. Potential side eff ects include back pain, musculoskeletal pain, cystitis, and hypercholesterolemia. Denosumab has been associated with cellulitis and skin rash, as well as ONJ and AFF in rare cases.
Teriparatide
Recombinant human PTH, or teriparatide, builds bone—as opposed to reducing bone resorption. It is approved for initial treatment of women with postmenopausal osteoporosis who are at high risk of fracture or have failed or been intolerant of previous osteoporosis therapy. Administered SC by patients themselves, teriparatide reduces fracture risk by 50%-65%, depending on the site, after 18 months of therapy. Use of this agent is limited to 2 years. It is contraindicated in patients with pre-existing hypercalcemia, severe renal impairment, or a history of bone metastases or skeletal malignancies, and in those who are at an increased baseline risk for osteosarcoma.23 Potential side effects include orthostatic hypotension, dizziness, myalgias, arthalgias, leg cramps, transient hypercalcemia, increased serum uric acid, hypercalciuria, headache, and nausea.
Monitoring treatment response
After initiating treatment, patients are seen 1-3 months later to check their adherence to the medication regimen and for lab testing. Patients are seen at least yearly to assess their response. Stable or increasing BMD at the spine and hip, as well as no fractures, indicates a satisfactory response.12 Therefore, serial central DXA, performed 1-2 years after initiating therapy and every 2 years thereafter, is a vital component of osteoporosis management. The decision to test BMD every 2 years is based on the time it takes for treatment-related improvement in BMD to occur and on Medicare and health insurance company reimbursement.
Yearly height measurement is also a crucial determinant of osteoporosis treatment efficacy. Patients who lose 2 cm (0.8 in) of height either acutely or cumulatively should undergo repeat vertebral imaging to determine whether new or additional vertebral fractures have occurred since the previous test.4
Duration of pharmacologic treatment
In 2016, the American Society for Bone and Mineral Research issued guidelines for long-term BP treatment.24 The society recommends that, after 5 years of oral therapy or 3 years of IV therapy, HCPs reassess patients’ fracture risk. For women at high risk, HCPs should consider continuing treatment for up to 10 years (oral) or 6 years (IV), with periodic evaluation. Although the risk of AFF, but not ONJ, increases with BP treatment duration, it is outweighed by the benefit of vertebral fracture risk reduction. For women not at high fracture risk, a drug holiday of 2-3 years can be considered after 3-5 years of treatment. By contrast, a drug holiday is not recommended for denosumab users because BMD benefits are rapidly lost with drug discontinuation. Treatment with teriparatide, which is taken for no longer than 2 years, is followed by treatment with an antiresorptive agent to prevent BMD decline and loss of fracture efficacy.
All non-BP osteoporosis medications produce temporary beneficial effects that wane upon discontinuation. By contrast, BPs may allow residual protection against fracture even after treatment cessation. Therapy should be resumed if a fracture occurs, if BMD declines beyond the least significant change (a value computed by each testing facility for relevant measurement sites to determine the magnitude of diff erence that represents a real change), or patients meet initial treatment criteria.
Conclusion
Healthcare providers can decrease postmenopausal patients’ risk of developing osteoporosis and/or experiencing a fragility fracture by clinically assessing them for these risks, ordering radiographic imaging and BMD measurement via DXA as indicated, and prescribing nondrug interventions and pharmacotherapy as needed. Patients who adhere to and tolerate their drug regimens can reduce their fracture risk, depending on the medication and the site, by about half. Patients on osteoporosis medication should be monitored at least once yearly to assess response to treatment, which is gauged by height measurement (every year), BMD via DXA (every 1-2 years), and absence of new fractures.
References
1. National Institutes of Health. Osteoporosis Prevention, Diagnosis, and Therapy. NIH Consensus Statement; March 27-29, 2000.
2. National Osteoporosis Foundation. Osteoporosis Fast Facts. 2015.
3. Blake GM, Fogelman I. The role of DXA bone density scans in the diagnosis and treatment of osteoporosis. Postgrad Med J. 2007;83(982):509-517.
4. Cosman F, de Beur SJ, LeBoff MS, et al. Clinician’s guide to prevention and treatment of osteoporosis. Osteoporosis Int. 2014;25(10):2359-2381.
5. World Health Organization. Assessment of Fracture Risk and its Application to Screening for Postmenopausal Osteoporosis: Technical Report Series 843. Geneva, Switzerland: WHO; 1994.
6. Unnanuntana A, Gladnick BP, Donnelly E, Lane JM. The assessment of fracture risk. J Bone Joint Surg Am. 2010;92(3):743-753.
7. FRAX® Fracture Risk Assessment Tool. n.d.
8. Kanis JA, Hans D, Cooper C, et al; Task Force of the FRAX Initiative. Interpretation and use of FRAX in clinical practice. Osteoporos Int. 2011;22(9):2395-2411.
9. Marshall D, Johnell O, Wedel H. Meta-analysis of how well measures of bone mineral density predict occurrence of osteoporotic fractures. BMJ. 1996;312(7041):1254-1259.
10. Tinetti ME. Clinical practice. Preventing falls in elderly persons. N Engl J Med. 2003;348(1):42-49.
11. Berry SD, Kiel DP. Falls as risk factors for fracture. In: Marcus R, Feldman D, Nelson DA, Rosen CJ, eds. Osteoporosis. 3rd ed. San Diego, CA: Academic Press; 2008.
12. Camacho PM, Petak SM, Binkley N, et al. American Association of Clinical Endocrinologists and American College of Endocrinology Clinical Practice Guidelines for the Diagnosis and Treatment of Postmenopausal Osteoporosis – 2016. Endocr Pract. 2016;22(suppl 4):1-42.
13. Burge R, Dawson-Hughes B, Solomon DH, et al. Incidence and economic burden of osteoporosis-related fractures in the United States, 2005-2025. J Bone Miner Res. 2007;22(3):465-475.
14. International Osteoporosis Foundation. Vertebral Fracture Initiative. Part I: Overview of Osteoporosis: Epidemiology and Clinical Management.
15. Lewiecki EM, Laster AJ. Clinical review: Clinical applications of vertebral fracture assessment by dual-energy x-ray absorptiometry. J Clin Endocrinol Metab. 2006;91(11):4215 4222.
16. Orwig DL, Chan J, Magaziner J. Hip fracture and its consequences: differences between men and women. Orthop Clin North Am. 2006;37(4):611-622.
17. U.S. Preventive Services Task Force. Final Recommendation Statement: Osteoporosis: Screening. April 2016.
18. National Osteoporosis Foundation. Bone Density Exam/Testing. 2016.
19. American College of Obstetricians and Gynecologists. Osteoporosis Guidelines Issued. August 21, 2012.
20. Institute of Medicine Committee to review dietary reference intakes for vitamin D and calcium. In: Ross AC, Taylor CL, Yaktine AL et al, eds. Dietary Reference Intakes for Calcium and Vitamin D. Washington, DC: National Academies Press; 2011.
21. Kaiser Permanente. Southern California. Fracture Liaison Service. 2013.
22. Block GA, Bone HG, Fang L, et al. A single-dose study of denosumab in patients with various degrees of renal impairment. J Bone Miner Res. 2012;27(7):1471-1479.
23. Quattrocchi E, Kourlas H. Teriparatide: a review. Clin Ther. 2004;26(6):841-854.
24. Adler RA, El-Hajj Fuleihan G, Bauer DC, et al. Managing Osteoporosis in Patients on Long Term Bisphosphonate Treatment: Report of a Task Force of the American Society for Bone and Mineral Research. J Bone Miner Res. 2016;31(1):16-35.