
Continuing education approval: This activity has been evaluated and approved by the Continuing Education Approval Program of the National Association of Nurse Practitioners in Women’s Health (NPWH) for 1.0 continuing education contact hour now through April 31, 2025.
Educational objectives: At the conclusion of this educational activity, participants should be able to:
1.
Discuss alcohol consumption patterns and alcohol consumption guidelines for women.
2.
Describe how to administer a validated alcohol use screening tool in primary care settings.
3.
Discuss the steps for a brief negotiated interview as part of screening, brief intervention, and referral for treatment (SBIRT) used in primary care settings.
The authors have no actual or potential conflicts of interest in relation to the contents of this article.
Disclaimer: Participating faculty members determine the editorial content of the CE activity; this content does not necessarily represent the views of NPWH. This content has undergone a blinded peer review process for validation of clinical content. Although every effort has been made to ensure that the information is accurate, clinicians are responsible for evaluating this information in relation to generally accepted standards of care and integrating the information in this activity with that of established recommendations of other authorities, national guidelines, and individual patient characteristics.
Commercial support: This activity did not receive any commercial support.
Successful completion of the activity:
Successful completion of this activity, J-23-02, requires participants to do the following:
1.
“Sign in” at the top right-hand corner of the page pathlms.com/npwh/courses/51970 if you have an NPWH account. You must be signed in to receive credit for this course. If you do not remember your username or password, please follow the “Forgot Password” link and instructions on the sign-in page. If you do not have an account, please click on the “Create an Account.”*
2.
Read the learning objectives, disclosures, and disclaimers.
3.
Study the material in the learning activity during the approval period (now through April 31, 2025).
4.
Complete the post-test and evaluation. You must earn a score of 70% or higher on the post-test to receive CE credit.
5.
Print out the CE certificate after you have successfully passed the post-test and completed the evaluation.
*
If you are an NPWH member, were once a member, or have completed CE activities with NPWH in the past, you have a username and password in our system. Please do not create a new account. Creation of multiple accounts could result in loss of CE credits as well as other NPWH services. If you do not remember your username or password, either click on the “Forgot Username” or “Forgot Password” link or call the NPWH office at (202) 543-9693, ext. 1.
In the United States, alcohol use by women is common and frequent.1 In 2020, 51.2% of women reported alcohol use in the past month.1 Further, 18% of reproductive-age women (18–44 years) report binge drinking (ie, consuming four or more standard drinks in a 2-hour period for assigned female at birth).2 From 2018 to 2020, nearly 14% of pregnant people reported current drinking and about 5% reported binge drinking.3 It is important to note that the research presented in this article is based on findings collected from cisgender populations of individuals assigned female at birth. As such, the comparisons made between the substance-use behaviors of men and women are most in line with the experiences of cisgender women.
For women, heavy alcohol use is associated with infertility and miscarriage, along with a risk for other adverse health effects.4–8 Any alcohol use during pregnancy is associated with fetal alcohol spectrum disorders.9–11 There also appears to be a “telescoping effect” to women’s alcohol use, tending to progress to alcohol dependence more quickly than men and experiencing alcohol-related health problems more quickly in comparison.12 There are differences in how women and men perceive or present their excessive alcohol consumption: women are more likely to identify health or mental health concerns while men often cite excessive alcohol or substance use.13–15 Although there are barriers for treatment and intervention, healthcare providers can utilize screening, brief intervention, and referral to treatment (SBIRT) to identify excessive alcohol or substance use in clients at risk for developing dependency issues or other alcohol-related harms. This article provides an overview of the components of SBIRT and includes a case study to illustrate its use in a primary care setting.
Alcohol consumption guidelines
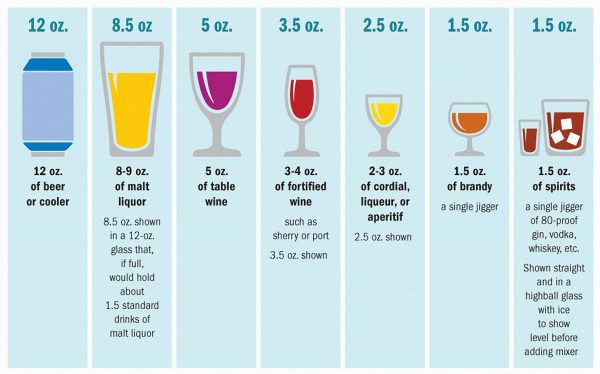
The alcohol consumption recommendation for women is no more than one standard drink per day and no more than seven standard drinks in a week (Figure 1). Exceeding these recommendations would classify someone as an at-risk drinker according to the National Institute on Alcohol Abuse and Alcoholism. People under the legal drinking age, who are currently pregnant or trying to become pregnant, or who are recovering from a substance use disorder are recommended to abstain from any alcohol consumption.16–18
Figure 1.
Alcohol screening
In order to avoid the adverse health effects related to alcohol use, the US Preventive Services Task Force recommends all individuals age 18 and older be screened in primary care settings for excessive alcohol use to help prevent long-term adverse health outcomes.19 The Alcohol Use Disorders Identification Test-Concise (AUDIT-C) is a simple three-question screener that can identify hazardous or harmful drinking. The AUDIT-C can be administered alone or incorporated into general health history questionnaires. It takes no more than approximately 5 minutes for the client to complete and for the clinician or medical assistant to score. If a client scores positive (3 or higher), a full 10-item AUDIT should be administered to further assess consumption, drinking behaviors, and alcohol-related problems. A score of 8 or more on the full AUDIT indicates hazardous or harmful alcohol use, and these patients are likely good candidates for brief intervention, and potentially for follow-up. The AUDIT and the AUDIT-C have been validated in a wide range of racial and ethnic groups and are recommended for medical settings. Both instruments are in the public domain.
SBIRT
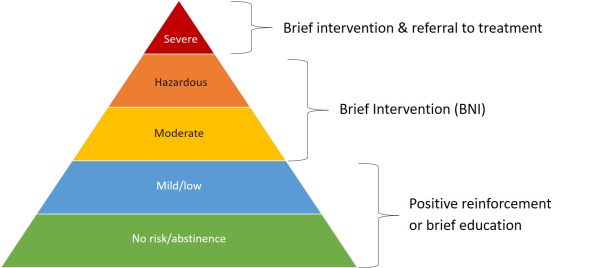
Sometimes referred to as SBI [screening and brief intervention], SBIRT combines the use of a standardized screening tool such as the AUDIT with a brief intervention. In SBIRT, using motivational interviewing strategies, the healthcare provider offers feedback based on the screener, offers advice, assesses the client’s readiness to change, and helps identify and foster the client’s own intrinsic motivations for change. The clinician assists the client with goal setting and follow-up as appropriate. SBIRT has been shown to be an effective strategy for helping people reduce their alcohol use, therefore reducing their risk for adverse health outcomes.20,21 A key feature of SBIRT is that it identifies clients whose current drinking patterns place them at risk for poor health outcomes, allowing the healthcare practitioner to provide timely advice or counseling around reducing their alcohol use. SBIRT can also identify clients whose alcohol use patterns indicate they may already meet the definition for an alcohol use disorder. For these clients, a referral by the healthcare provider for further assessment or treatment may be warranted. Most clients screened will require only positive reinforcement or brief education about lowering their risk for adverse outcomes (Figure 2).
Figure 2.
Brief counseling/intervention
However, some clients may benefit from the next step, the brief intervention. Also known as the brief negotiated interview (BNI), this is a focused discussion with the client about their drinking patterns and identifying their motivation to change these behaviors. The Table outlines the five steps of BNI including recommended scripts.
Case study
Frankie (she/her) is a 30-year-old female who presents for a pelvic exam, her first visit to your clinic. Frankie states that she is sexually active and has multiple male sex partners. She reports she is not on birth control but is using condoms “most of the time.” Frankie has no history of prior pregnancies or sexually transmitted infections (STIs). She has no current symptoms or reported problems. She usually consumes alcohol socially when out with friends. Frankie scored a 7 on the AUDIT-C: she consumes a drink containing alcohol 2 to 3 times per week, consumes 3 standard drinks on a typical day she drinks, but at least weekly she has more than 4 standard drinks on one occasion. When asked the remaining AUDIT questions, Frankie shared that a few times in the last year she has been unable to do what was expected of her because of her drinking (eg, she has been unable to go to work). Her full AUDIT score was 10.
Build rapport
Begin by asking permission to ask about the topic of alcohol use, using the prompts in the Table as a guide. Consider providing feedback that interprets Frankie’s screening score with sexual health behaviors, such as the risk of developing a chronic STI. Additionally, her alcohol use combined with inconsistent contraception increases risk for an unintended and/or alcohol-exposed pregnancy. Follow up by asking what she thinks about the information you provided. This sets up the opportunity to listen to her concerns and discuss options she may wish to consider.
Table. Five steps of brief negotiated interview
Build rapport
Ask client’s permission to discuss their alcohol or other substance use.
“We are now talking to each client, no matter why they are here, about their alcohol and drug use. We know these things can have a significant impact on your health, and we want to help our clients make informed healthcare decisions that they think are best for them. Would it be okay if we took some time together to discuss your thoughts around your alcohol or substance use?”
If a client does not consent to discussing their alcohol or substance use, the clinician can express their concern about the potential adverse health impacts and leave the conversation open to resume at another visit.
Ask about how alcohol or other substances fit into the client’s routine.
“Tell me about…”
“Tell me about a typical day in your life. Where does your current use fit in?”
Discuss the pros and cons of the client’s substance use
Elicit the pros the client sees.
“Tell me through your eyes, the good things about using/drinking [substance of choice] are…”
“What else?”
Elicit the cons the client sees.
“What may be some of the not-so-good things about using/drinking [substance of choice]?”
“What else?”
Provide a summary of what the client said.
“On the one hand [what’s good about the behavior], and on the other hand [what’s not so good about the behavior].”
Provide information and feedback
Explore the client’s experiences with alcohol or other substance use further.
“When you completed the form you mentioned … Can you tell me more about that?”
Connect the client’s alcohol or other substance use back to health.
“While I hear that drinking is important to you because… but I’m concerned it may be [health concern/medical problem].”
“We know that as a woman, if you have more than four drinks in 2 hours or more than seven drinks in a week you put yourself at risk of social or legal problems, as well as illness or injury. It can also cause health problems like…”
Elicit the client’s thoughts.
“What do you think about this information?”
Introduce the readiness ruler
Support the client’s autonomy.
“You have thought a lot about what is best for you and it is absolutely your choice what you decide.”
Ask a scaling question.
“Thinking about where you are right now, on a scale from 1 to 10, with 1 being not ready at all, and 10 being completely ready, how ready are you to change your alcohol or substance use?”
Ask a follow-up question to elicit change talk.
“You marked… That means you are…% ready to make a change. Why did you choose that number and not a lower one like a 1 or a 2?”
Action plan
Summarize the discussion.
“What will help you reduce the things you don’t like about using alcohol?”
Ask a follow-up question.
“What support do you have for making this change?”
“Tell me about a challenge you overcame in the past.”
Offer appropriate resources.
“Is it okay for me to write down your plan, to keep with you as a reminder?
Will you summarize the steps you’ll take to change your alcohol or substance use?”
Thank the client.
Discuss pros and cons
Ask Frankie to tell you about the good things she associates with drinking alcohol, then follow up with a question about the not-so-good things. Summarize these pros and cons, for example: “So, on the one hand, you enjoy drinking when out with your friends, and on the other hand, you don’t like how it leaves you feeling the next day.”
Provide information and feedback
Based on what Frankie has told you, you can provide tailored feedback and information. It is important to connect her alcohol use back to any concerns you have for her health. For example: “While I hear drinking is important to you because it helps you connect with your friends, we know that if you have more than four drinks in 2 hours or more than seven drinks in a week you put yourself at risk of social or legal problems (eg, interpersonal relationship problems, DUI, loss of employment), as well as illness or injury. Given what you have told me about condom use, I also am concerned that you have an increased risk for an STI or an unintended pregnancy. What do you think about this information?”
Support the client’s autonomy
At this point in the BNI, introduce the readiness ruler. You could say, “Thinking about where you are right now, on a scale from 1 to 10, with 1 being not ready at all and 10 being completely ready, how ready are you to change your alcohol use?” This will help you elicit change talk, the words and phrases that indicate Frankie is contemplating making a change in her drinking. In this case study, Frankie selects 6. You can follow up that selection with: “You marked 6. That means you are 60% ready to make a change. Why did you choose that number and not a lower number, like 1 or 2?” Asking about the lower number will help you learn about and reinforce Frankie’s own reasons for change.
Action plan
Before developing an action plan, summarize the discussion and have Frankie identify the things she can do to make this change. Ask her what types of supports she has and about another time she successfully made a change. This is intended to bolster her confidence and identify her support network. It will help you provide appropriate additional resources should she need them. Finally, have Frankie summarize the action plan and ask her permission to write down the plan so she can keep it with her. Thank Frankie for talking with you about this topic.
Adapting SBIRT for your practice
SBIRT should be implemented at the clinic level to ensure that all clients are provided consistent care and services are reimbursed appropriately.22 There are several key parts to an SBIRT implementation plan.
Who will be screened?
SBIRT is meant to be universal, but the recommendations found here are specifically for cisgender women of reproductive age. The recommended screening tools, as well as the SBIRT process, may need to be modified to better serve the needs of individuals in special populations.
How often will clients be screened?
Best practice recommends that all clients be screened at least yearly.
Reimbursement
Services related to SBIRT are reimbursable through commercial insurance providers, Medicare, and Medicaid. CPT code 99408 and Medicare code G0396 can be used for structured services between 15 and 30 minutes. CPT code 99409 and Medicare code G0397 can be used for structured SBIRT services beyond 30 minutes. Medicaid code H0049 can be used for alcohol and/or drug screening. H0050 can be used for SBIRT services up to 15 minutes. The ability to bill Medicaid for SBIRT- related services may vary by state.23
Implementing SBIRT versus business as usual
There are several advantages to implementing SBIRT in daily clinical practice. Routine and universal screening using a validated screening tool normalizes conversations about alcohol use. It can help reduce inconsistent and selective screening practices that are based in personal biases or stereotypes, thereby reducing stigma and bias and improving clinician–client trust and rapport. Interventions are client driven and evidence-based with a focus on whole-person care.
Summary and recommendations
As trusted healthcare professionals, primary care providers are ideally placed to conduct SBIRT. The implementation of SBIRT by nurse practitioners in primary care settings is the most sustainable plan of integration because of the role these professionals already have within clinical settings. The addition of SBIRT into training curricula for nurse practitioners will ensure that they are able to continue providing person-centered, respectful care while effectively identifying individuals engaging in risky drinking. The Box provides examples of resources available for use in nurse practitioner programs and for nurse practitioner continuing education.
Box. Resources
- NPs, Midwives, and Nurses: Partnering to Prevent Fetal Alcohol Spectrum Disorders https://sites.google.com/view/nursesmidwivespreventfasds/home B
- Velasquez MM, Ingersoll K, Sobell M, Sobell LC. Women and Drinking: Preventing Alcohol-Exposed Pregnancies. Series: Advances in Psychotherapy–Evidence-Based Practices, vol. 34.
- Centers for Disease Control and Prevention. CHOICES: Preventing Alcohol Exposed Pregnancies. www.cdc.gov/ncbddd/fasd/choices-importance-preventing-alcohol-exposed-pregnancies.html C
- Implementing Care for Alcohol and Other Drug Use in Medical Settings. An extension of SBIRT. thenationalcouncil.org/wp-content/uploads/2021/04/Implementing_Care_for_Alcohol_and_Other_Drug_Use_In_Medical_Settings_-_An_Extension_of_SBIRT.pdf D
- Centers for Disease Control and Prevention. Fetal alcohol spectrum disorders (FASDs). Online training and resources. nccd.cdc.gov/FASD/ E
- Using SBIRT to talk to adolescents about substance use. Four-part on-demand webinar series. sbirt.webs.com/talking-2-adolescents-series F
- National Frontier and Rural Telehealth Education Center. Lions, Tigers, & Bears: Guiding listeners through using motivational interviewing. nfartec.org/mipodcast/ G
This work is supported by the US Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) Cooperative Agreement Number NU84DD000017 and NU84DD000009. These contents are solely the responsibility of the authors and do not necessarily represent the official views of the CDC, the US Department of Health and Human Services, the University of Alaska Anchorage Institute of Social and Economic Research, or the University of Texas at Austin Steve Hicks School of Social Work.
Womens Healthcare. 2023;11(2):4-10. doi: 10.51256/WHC042304
References
1 US Department of Health and Human Services. Substance Abuse and Mental Health Services Administration. 2020 National survey of drug use and health (NSDUH) releases. https://www.samhsa.gov/data/release/2020-national-survey-drug-use-and-health-nsduh-releases.
2 Centers for Disease Control and Prevention. Excessive alcohol use is a risk to women’s health. Updated October 17, 2022. https://www.cdc.gov/alcohol/fact-sheets/womens-health.htm.
3 Gosdin LK, Deputy NP, Kim SY, et al. Alcohol consumption and binge drinking during pregnancy among adults aged 18–49 years – United States, 2018–2020. MMWR Morb Mortal Wkly Rep. 2022;71(1):10-13.
4 O’Keefe JH, Bhatti SK, Bajwa A, et al. Alcohol and cardiovascular health: the dose makes the poison…or the remedy. Mayo Clin Proc. 2014;89(3):382-393.
5 Roerecke M, Vafaei A, Hasan OSM, et al. Alcohol consumption and risk of liver cirrhosis: a systematic review and meta-analysis. Am J Gastroenterol. 2019;114(10):1574-1586.
6 Erol A, Karpyak VM. Sex and gender-related differences in alcohol use and its consequences: Contemporary knowledge and future research considerations. Drug Alcohol Depend 2015;156:1–13
7 Rehm J, Shield KD, Weiderpass E. Alcohol consumption: a leading risk factor for cancer. In: Wild CP, Weiderpass E, Stewart BW, eds. World Cancer Report. Lyon, France: International Agency for Research on Cancer; 2020:68-76.
8 Bailey BA, Sokol RJ. Prenatal alcohol exposure and miscarriage, stillbirth, preterm delivery, and sudden infant death syndrome. Alcohol Res Health 2011;34:86-91.
9 Mattson SN, Bernes GA, Doyle LR. Fetal alcohol spectrum disorders: a review of the neurobehavioral deficits associated with prenatal alcohol exposure. Alcohol Clin Exp Res. 2019;43(6):1046-1062.
10 Hagan JF Jr, Balachova T, Bertrand J, et al. Neurobehavioral disorder associated with prenatal alcohol exposure. Pediatrics. 2016;138(4):e20151553.
11 Bertrand J. Fetal alcohol spectrum disorders are clearly brain-based. Dev Med Child Neurol. 2016;58(8):794-795.
12 Keyes KM, Martins SS, Blanco C, Hasin DS. Telescoping and gender differences in alcohol dependence: new evidence from two national surveys. Am J Psychiatry. 2010;167(8):969-976.
13 Velasquez MM. Women and alcohol: screening and brief intervention and referral to treatment (SBIRT) in medical settings. 25th Annual Nurse Practitioners in Women’s Health (NPWH) Women’s Healthcare Conference, Houston, Texas, 2022.
14 Washburn V. The 2021 annual meeting goes fully virtual. ACNM 68th Annual Meeting & Exhibition. February 3, 2021. https://annualmeeting.midwife.org/the-2021-annual-meeting-goes-fully-virtual/.
15 HealthManagement.org. ACNM 2022 – 67th Annual Meeting & Exhibition. January 24, 2023. https://healthmanagement.org/c/hospital/event/acnm-2022-67th-annual-meeting-exhibition.
16 Centers for Disease Control and Prevention. Dietary guidelines for alcohol. April 19, 2022. https://www.cdc.gov/alcohol/fact-sheets/moderate-drinking.htm.
17 National Institutes on Alcohol Abuse and Alcoholism. Drinking levels defined. February 6, 2023. https://www.niaaa.nih.gov/alcohol-health/overview-alcohol-consumption/moderate-binge-drinking.
18 US Department of Agriculture; US Department of Health and Human Services. Dietary Guidelines for Americans, 2020-2025, 9th ed. December 2020. DietaryGuidelines.gov.
19 US Preventive Services Task Force, Curry SJ, Krist AH, Owens DK, et al. Screening and behavioral counseling interventions to reduce unhealthy alcohol use in adolescents and adults: US Preventive Services Task Force recommendation statement. JAMA 2018;320(18):1899-1909.
20 Doi L, Jepson R, Cheyne H. A realist evaluation of an antenatal programme to change drinking behaviour of pregnant women. Midwifery. 2015;31(10):965-972.
21 Higgins-Biddle JC, Babor TF. A review of the alcohol use disorders identification test (AUDIT), AUDIT-C, and USAUDIT for screening in the United States: past issues and future directions. Am J Drug Alcohol Abuse. 2018;44(6):578-586.
22 Centers for Disease Control and Prevention. Planning and Implementing Screening and Brief Intervention for Risky Alcohol Use: A Step-by-Step Guide for Primary Care Practices. Atlanta, Georgia: Centers for Disease Control and Prevention, National Center on Birth Defects and Developmental Disabilities.
23 US Department of Health and Human Services. Substance Abuse and Mental Health Services Administration. Coding for screening and brief intervention reimbursement. Updated April 14, 2022. https://www.samhsa.gov/sbirt/coding-reimbursement.
Key words: alcohol use, SBIRT, AUDIT