
By Tara Fernandez Bertulfo, DNP, ARNP
Text message reminders were studied as an innovative, low cost method of improving adherence to monthly breast self examination/breast self-awareness among college-aged women. Results of this pilot study are presented and discussed in this article.
KEY WORDS: breast cancer, breast self-examination, breast self awareness, text message reminder, college-aged women
Each year in the United States, more than 200,000 women are diagnosed with breast cancer.1 Aside from nonmelanoma skin cancer, breast cancer is the most common form of cancer in women. Breast cancer is the No. 1 cause of cancer death in Hispanic women and the second most common cause of cancer death in women in all other ethnic groups in the U.S2
The major strategy to reduce breast cancer mortality is early detection. Breast cancers found during regular screening examinations, as opposed to those found because of symptoms, are more likely to be smaller and still confined to the breast; these two factors are the most important in determining prognosis.3 Early detection techniques include screening modalities such as mammography, clinical breast examination (CBE), breast self-examination (BSE), and breast self-awareness (BSA).
Breast self-examination
Breast self-examination, taught to women for years, consists of sequential steps (done in the shower, before a mirror, and lying down) and observations for changes or inconsistencies from one breast to the other.4 Premenopausal women are advised to perform BSE once a month—about 1 week following menses.
Breast self-awareness
More recently, there has been a movement toward teaching BSA, a less formal approach to breast cancer self-screening. This approach places less emphasis on technique and timing and more emphasis on a woman’s ability to be familiar with the look and feel of her breasts so that she can be alert to any changes that may occur and seek further evaluation by a healthcare provider (HCP).
With BSA, no formal method for examining the breasts is taught. Instead, women are encouraged to know their family history, understand risk reduction strategies, and be observant for any changes in their breasts by periodically viewing and feeling the entire area, including the breasts, collarbone, and underarms.5 To practice breast self-awareness, a woman is instructed to be alert to changes such as (a) a lump, hard knot, or thickening inside the breast or underarm area; (b) swelling, warmth, redness, or darkening of the breast; (c) change in the size or shape of the breast; (d) dimpling or puckering of the skin; (e) itchy, scaly sore or rash on the nipple; (f ) pulling in of the nipple or other parts of the breast; (g) nipple discharge that starts suddenly; or (h) pain in one spot that does not go away.6
Because BSE efficacy is controversial (related to inadequate evidence of lowered mortality as a result of its use), other than CBE, being breast aware is the only method that most women younger than 40 can use to screen
for breast cancer. Under ideal circumstances, HCPs should start educating and encouraging women to begin self-screening in early adulthood, before breast cancer risk begins to rise. The American Cancer Society,7 the National Comprehensive Cancer Network,8 the American Congress of Obstetricians and Gynecologists,9 and the Susan G. Komen Foundation6 now endorse BSA as an alternative to BSE.
Of note, women younger than 40 who have an increased risk for breast cancer (e.g., because of family history, a known genetic mutation, or a history of chest radiation) have different screening recommendations that include,
but are not limited to, CBE and BSA. Women who are older than 40, who may be having regular mammograms, should still be encouraged to remain breast aware.
Self-screening reminders
Multiple national and international studies have evaluated breast self-screening behavior.10-13 Commonly reported reasons for not performing the recommended self-screening are forgetting or being too busy.10,12,14 Many strategies to remind women to self-screen, including shower cards, oral contraceptive packaging, and, more recently, smartphone applications, have been used. However, among collegeaged women, one strategy that has not been widely tested is use of a text message reminder (TMR). With this strategy, a monthly text message reminds a woman to take a few minutes to focus on her breast health.
Several studies examining the use of text messaging in healthcare have shown that TMRs improve outpatient clinical attendance,15 improve adherence to asthma treatment,16 encourage weight loss,17 improve adherence to daily intake of vitamin C supplements,18 and support patients with diabetes.19 A study by Armstrong et al20 evaluated the effect of TMRs on adherence to sunscreen application among 70 participants from the general community. Throughout the 6-week study, half the participants received daily TMRs and half did not. TMR recipients, versus the controls, were nearly twice as likely to maintain a regimen of daily sunscreen use throughout the study period.
Text message reminders are easy to implement and may be particularly appealing to younger people, an important target population for the development of positive health habits. With this in mind, and with the goal of promoting monthly breast cancer self-screening in early adulthood, the investigator recruited college-aged women for
this pilot study. Pre- and post-intervention questionnaires were used to assess participants’ baseline selfscreening frequency and beliefs regarding its importance; their perceptions of the usefulness and acceptability of the TMR; and whether they performed selfscreening following its receipt.
Pilot study
Methods
A pilot project using a descriptive, one-group, pre-test/post-test study design was conducted to explore the usefulness and acceptability of a TMR to perform BSE.* The study was approved by the Institutional Review Boards at the institution where the investigator was a student and at the site where the study was conducted.
Participants and setting
A convenience sample (N = 62) was recruited from first-year, second-semester, baccalaureate nursing students
enrolled in nursing classes at a southern university. These students were chosen because they were in the age group of interest and because they had been previously instructed in BSE. As such, the study questions did not need to focus on whether participants knew how to examine their breasts, whether they had been formally taught this technique, or whether they felt comfortable with their skills in this area.
Procedure
After providing written informed consent, participants completed a self-administered baseline questionnaire and demographic form. The questionnaire, developed by the investigator, was used to establish the frequency with which the participants performed BSE, as well as their beliefs about BSE. Along with written informed consent, participants provided a mobile phone number to receive a text message and authorized the investigator to send them a TMR. The investigator then manually entered the mobile phone numbers into the Google Voice website. One week later, the investigator sent a text message, Time for your monthly breast self-exam, to each participant simultaneously via Google Voice.
About 1 month after the TMR was sent, participants were asked to complete a follow-up questionnaire developed by the investigator. The questionnaire was used to ascertain whether participants performed BSE, as well as their perceptions of the effectiveness and acceptability of the TMR.
Results
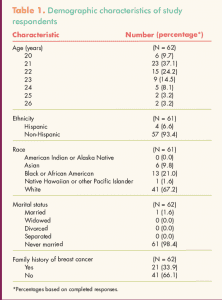
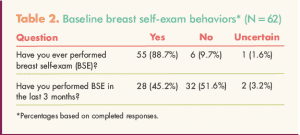
Demographic characteristics of the sample are shown in Table 1. Mean age of the participants was 22 years (SD, 1.44). Most participants were white, never-married women who did not have a family history of breast cancer. Data on BSE behaviors were collected from all participants at baseline (Table 2). Among the 34 participants who reported not having performed BSE in the past 3 months (n = 32) or who were uncertain about it (n = 2), reasons for not doing so included I forgot (n = 15), I don’t think about it (n = 15), I’m not sure what I’m feeling (n= 3), I’m too busy (n = 1), and I’m too young (n = 1).
![]()
![]()
![]()
![]()
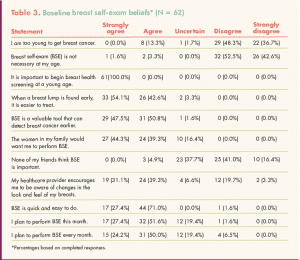
Table 3 shows participants’ beliefs about BSE at baseline. Among 11 beliefs examined, those with which participants agreed most strongly included the following: It is important to begin breast health screening at a young age; When a breast lump is found early, it is easier to treat; BSE is a valuable tool that can detect breast cancer earlier; BSE is quick and easy to do; and The women in my family would want me to perform BSE. Beliefs with which participants disagreed most strongly were as follows: I am too young to get breast cancer; and Breast self-exam is not necessary at my age.
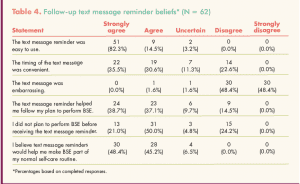
Overall performance of BSE increased significantly following the TMR (Table 4). When the 62 participants were asked whether the TMR helped them follow their plan to perform BSE, 47 (75.8%) agreed or strongly agreed with the statement, 9 (14.5%) disagreed, and 6 (9.7%) were uncertain. When asked whether they felt that the TMRs would help them make BSE part of their usual self-care routine, 58 participants (93.6%) agreed or strongly agreed.
Of note, participants with a family history of breast cancer were no more likely than those without such a history to perform BSE after receiving the TMR. In addition, no association was found between whether or not participants
reported My healthcare provider encourages me to be aware of changes in the look and feel of my breasts and whether they performed BSE following the TMR.
Discussion
The baseline data showed that participants believed BSE was important for women in their age group. Nevertheless, 50% of participants had not performed BSE in the previous 3 months, with most reporting that they did not do so because they forgot or did not think about it. This study confirms findings from previously mentioned studies about the use of TMRs to improve adherence to health-promoting behaviors.
Although most participants found the TMR acceptable, helpful, and easy to use, the timing of the TMR was found to be an important factor in terms of both the decision to perform BSE (or not) and the amount of time between receiving the TMR and performing BSE. In consideration of this important finding, methods for allowing patients to choose the timing of a TMR should be considered for use in practice. This approach may help decrease the number of women who forget to perform BSE following the TMR, who have another priority at the time that the TMR is received, or who report the timing of the TMR as inconvenient.
Now that this trial is complete, women who were satisfied with the TMR were asked to inform their friends about it so that they, too, could register for the service. A plan is in place to promote this idea through student health services by advertising the availability of the TMR to young women who attend the clinic. This approach can help create initial knowledge of the innovation, which can then be reinforced by peer encouragement.
Limitations
This pilot study used a TMR to target forgetfulness; however, many other factors could contribute to non-adherence to BSE. Use of a control group would have strengthened the rigor of the study and will be considered for future research based on this pilot work. In addition, the sample for this study comprised nursing students from one southern university BSN program. Applicability of the findings to the general population of college-aged women is
unknown.
Implications for practice
In addition to promoting breast self-screening, TMRs could be used to help promote other aspects of health in young women. Text messages can remind young women of a return appointment for a DMPA injection, for chlamydia re-screening in 3 months following treatment, for annual checkups, and the like. These reminders can be implemented by college health centers, private offices, public health clinics, or any clinical setting that serves young women. Because TMR recipients would be providing their mobile phone numbers and granting permission for TMRs to be sent, and because no personal health information would be provided in these simple reminders, this system would not compromise HIPAA standards, particularly with regard to a reminder to self-screen for breast cancer. If a woman decides to receive multiple TMRs, and a particular reminder concerns a potentially sensitive situation such as a DMPA injection or chlamydia rescreening, the wording of the text message could be coded rather than explicit.
At the first clinic visit, the use and benefits of TMRs could be explained to the patient. The patient could then be asked (1) for permission to receive TMRs, (2) to provide a mobile phone number for this purpose, and (3) whether she prefers a specific day of the week or time of day to receive a TMR. At each subsequent visit, the patient could be asked to verify her mobile phone number and her preferences for the timing of TMRs.
Ease of implementation is a key factor for HCPs in a college health setting or other outpatient setting. Through use of Google Voice, one can send a large number of text messages at once free of charge. Text messages can be sent via Google Voice directly using a Google account; sent and received via email or IM interface by reading
and writing text messages in Gmail; or by adding contacts’ phone numbers in Google Talk (PC-to-phone texting). In addition, automated text message services send group text messages for a set fee, which decreases the amount of time required to send the TMRs and allows HCPs the opportunity to choose when the message will be sent.
Conclusion
Text message reminders are an innovative, easily implemented strategy that may increase adherence to breast cancer self-screening recommendations, as well as other self-care practices among college-aged women. Through use of current technology such as text messaging, HCPs can play a key role in endorsing positive health habits that may promote wellness in young women for a lifetime.
Tara Fernandez Bertulfo is a women’s health nurse practitioner and Clinical Assistant Professor at Georgia Baptist College of Nursing, Mercer University, in Atlanta, Georgia. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
1. U.S. Department of Health and Human Services, National Institutes of Health, National Cancer Institute.
What You Need to Know About Breast Cancer (NIH Publication No. 09-1556). 2012. cancer.gov/cancertopics/
insides-wyntk-breast.pdf
2. Centers for Disease Control and Prevention. Breast Cancer Statistics. 2014. cdc.gov/cancer/breast/statistics/
3. American Cancer Society. Breast Cancer: Early Detection. 2014. cancer. org/acs/groups/cid/documents/
webcontent/003165-pdf.pdf
4. National Breast Cancer Foundation. Breast Self-Exam. 2012. nationalbreastcancer. org/breast-self-exam
5. M.D. Anderson Cancer Center. Breast Self Awareness. 2012.
6. Susan G. Komen Foundation. Breast Self-Awareness. 2015. komen.org/BreastCancer/Breast-SelfAwareness.html
7. American Cancer Society. Breast Cancer Prevention and Early Detection. Breast awareness and self-exam.
2014. cancer.org/cancer/breastcancer/moreinformation/breastcancerearlydetection/breast-cancerearly-detection-acs-recs-bse
8. National Comprehensive Cancer Network. Stage 0 Breast Cancer. NCCN Guidelines for Patients. 2014. nccn.org/patients/guidelines/stage_0_breast/files/assets/common/downloads/files/stage_0_breast.pdf
9. American Congress of Obstetricians and Gynecologists. Breast Screening: Mammography and Breast Self-Awareness. 2012. acog.org/Patients/FAQs/Breast-Screening-Mammography-and-Breast-Self-Awareness
10. Budden L. Registered nurses’ breast self-examination practice and teaching to female clients. J Community
Health Nurs. 1998;15(2):101-112.
11. Friedman LC, Nelson DV, Webb JA, et al. Dispositional optimism, self efficacy and health beliefs as predictors of breast self-examination. Am J Prev Med. 1994;10(3):130-135.
12. Mason TE, White KM. The role of behavioral, normative and control beliefs in breast self-examination.
Women Health. 2008;47(3):39-56.
13. Tavafian SS, Hasani L, Aghamolaei T, et al. Prediction of breast selfexamination in a sample of Iranian
women: an application of the Health Belief Model. BMC Womens Health. 2009;9(37):1-7.
14. Ahuja S, Chakrabarti N. To determine the level of knowledge regarding breast cancer and to increase
awareness about breast cancer screening practices among a group of women in a tertiary care hospital in
Mumbai, India. Internet J Public Health. 2009;1(1).
15. Koshy E, Car J, Majeed A. Effectiveness of mobile-phone short message service (SMS) reminders for ophthalmology outpatient appointments: observational study. BMC Ophthalmol. 2008;8:9.
16. Strandbygaard U, Thomsen SF, Backer V. A daily SMS reminder increases adherence to asthma treatment:
a three-month follow-up study. Respir Med. 2010;104(2):166-171.
17. Patrick K, Raab F, Adams MA, et al. A text message based intervention for weight loss: randomized controlled
trial. J Med Internet Res. 2009;11(1):e1.
18. Cocosila M, Archer N, Haynes RB, Yuan Y. Can text messaging improve adherence to preventive activities?
Results of a randomized controlled trial. Int J Med Inform. 2009; 78(4):230-238.
19. Waller A, Franklin V. Pagilari C, Greene S. Participatory design of a text message scheduling system to
support young people with diabetes. J Health Inform. 2006;12(4):304-318.
20. Armstrong AW, Watson AJ, Makredes M, et al. Text-message reminders to improve sunscreen use. Arch Dermatol. 2009;145(11):1230-1236.