
Alcohol use is common in the United States. In 2020, 54.2% of adults age 18 and older reported drinking in the last month.1 Among female adults age 18 and older, 66.9% reported consuming alcohol in the last year and 51.2% reported any alcohol use in the past month.1 An estimated 9% of women have an alcohol use disorder.1 Approximately 18% of reproductive-age women (18–44 years) binge drink (defined as consuming four or more standard drinks in about 2 hours for women).2,3 Concerningly, analysis of data from the Behavioral Risk Factor Surveillance System (BRFSS) collected between 2011 and 2018 suggests that alcohol consumption during pregnancy is increasing.4 Recent analysis of 2018–2020 BRFSS data indicates that 13.5% of pregnant adults reported current drinking and 5.2% reported binge drinking, and these numbers are likely an underestimation.4,5
Fetal alcohol spectrum disorders (FASDs) are a range of life-long developmental conditions associated with exposure to alcohol during pregnancy.6 These conditions include fetal alcohol syndrome, partial fetal alcohol syndrome, alcohol-related neurodevelopmental disorder, alcohol-related birth defects, and neurobehavioral disorder associated with prenatal alcohol exposure.7,8 According to recent estimates, up to 1 in 20 schoolchildren in the US may have FASDs.9 The impact of such alcohol exposure can result in changes in brain development, manifesting as impaired neurocognitive function, poor executive functioning, attention deficits, and memory impairment, among other outcomes.7,9 Additionally, prenatal alcohol exposure can result in adverse birth outcomes such as premature birth and low birth weight.10
In an effort to reduce the number of alcohol-exposed pregnancies, 43 states have implemented legislation targeting alcohol use among pregnant people. This brief report summarizes the current status of these policies.
Policy categories
Policies created to address alcohol use during pregnancy fall under two categories: punitive or supportive. A 2019 study found that 25 states utilize a mixture of supportive and punitive policies, 14 utilize only supportive policies, four states use only punitive policies, and eight states utilize no policies.11 The Table provides information on which states are implementing supportive and/or punitive policies.
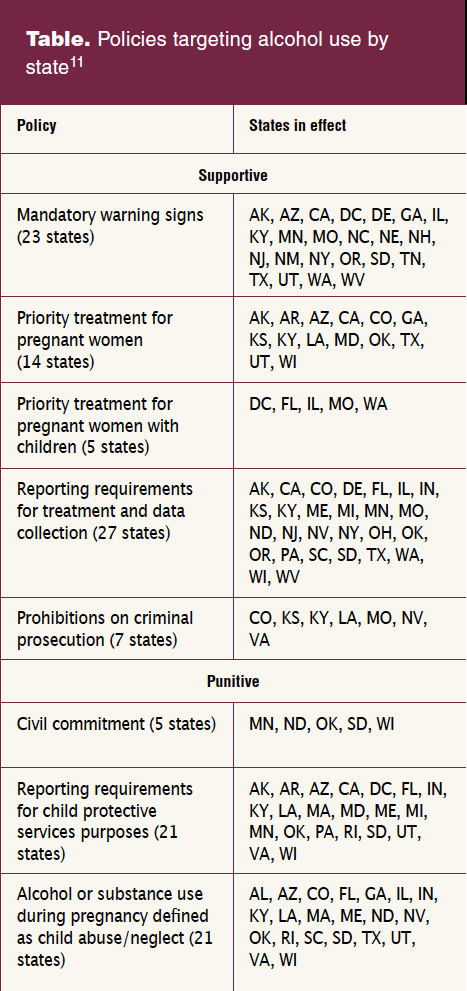
Supportive policies
Mandatory warning signs: Businesses that sell alcohol for consumption either on site or off site are required to have signs describing the negative impacts of alcohol use during pregnancy.
Priority substance abuse treatment: Pregnant persons (without children) and pregnant persons (with children) are given priority when seeking to enter treatment.
Prohibitions on criminal prosecutions: Medical records and prenatal test results are not admissible as evidence in criminal proceedings that are attempting to prove the pregnant person may have hurt their unborn child.
Reporting requirements for data and treatment purposes: These requirements are divided into two subcategories: reporting for child protective services in the instances of a child being at risk of danger and reporting for data collection or determining a need for treatment.11
Punitive policies
Civil commitment: This consists of placing a pregnant person in protective custody to protect the fetus from prenatal alcohol exposure. This is mandatory involuntary commitment, meaning the pregnant person does not have to consent to being committed.
Child protective services (CPS) reporting: These requirements allow the use of screening or toxicology tests of pregnant persons or of babies after birth and using those tests to report abuse or neglect to CPS or a health authority.
Child abuse/neglect: These policies examine the pregnant person’s behaviors while the fetus is in utero and allows for alcohol use during pregnancy to be legally defined as child abuse or neglect.11
Impact and effectiveness
Researchers used data from BRFSS from 1985 to 2016 to assess the impact of these policies on the prevalence of alcohol use during pregnancy.11 During this period, 57,194 pregnant women answered questions about alcohol use in the past 30 days. The study authors found women in states with no alcohol policies had lower likelihood of alcohol use during pregnancy than did women in both punitive and supportive policy environments, yet states with a punitive and/or supportive policy approaches were associated with increased likelihood of alcohol consumption during pregnancy.11
Another study examined the associations between state-level policies and adverse birth outcomes and prenatal care utilization.12 Using birth certificate data of singleton births in the US between 1972 and 2013, they found that mandatory warning signs and requirements for reporting child abuse/neglect were associated with increased likelihood for low birth weight and premature birth. Policies establishing priority treatment for pregnant women and prohibitions against criminal prosecutions also were associated with these increased likelihoods. Further, mandatory warning signs and civil commitment policies were associated with an increased likelihood of late prenatal care. A follow-up study found that mandatory warning signs were associated with an excess of babies born with a low birth weight, while defining alcohol use during pregnancy as child abuse/neglect was linked to an excess of preterm births.13
Furthermore, the ethical implications of such policies must be questioned. Punitive policies feed into negative stereotypes and contribute to the stigma surrounding alcohol use and FASDs for parents and children.14 Supportive policies also contribute to the negative stereotypes and have a different impact across various racial and ethnic groups.15 Taking all of this into account, the data suggest that current policy efforts are not successful in reducing the number of alcohol-exposed pregnancies. Although 86% of states have implemented policies intended to reduce alcohol use, the prevalence of alcohol-exposed pregnancies remains unaffected.5
An opportunity that policy makers should consider is the development of policies that make it easier for healthcare organizations to adopt cost-effective, evidence-based interventions that promote alcohol-free pregnancies.15,16 For example, universal alcohol screening and brief intervention (ASBI) as a routine preventive practice has been demonstrated through clinical studies as effective at reducing excessive alcohol use for adults without an alcohol use disorder, including pregnant women.17–19 ASBI is recommended by the US Preventive Services Task Force for all persons age 18 years and older who are seen in primary care settings, including pregnant women.20 The vast majority of people who are screened using the ASBI framework require only positive reinforcement of low-risk behaviors or brief education about reducing their risk for adverse health outcomes.5,21,22 Policies that provide financial support to primary and reproductive healthcare organizations for modifying electronic health record systems in ways that facilitate screening, brief intervention, and referrals to treatment, documentation and billing, incentives and reimbursement for providing ASBI services, and increased availability of programmatic resources, such as training and patient education materials, will help to address barriers to adopting this evidence-based practice, particularly in under-resourced communities.23 It is clear that more research is needed to identify and implement effective policy approaches to reducing alcohol consumption during pregnancy.
Kathryn E. Davis is Research Professional, Alexandra E. Edwards is Senior Research Professional, and Diane K. King is Research Associate Professor/Director of the Center for Behavioral Health Research & Services, Institute of Social and Economic Research, at the University of Alaska Anchorage. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
This project is supported by the US Department of Health and Human Services, Centers for Disease Control and Prevention (CDC) Cooperative Agreement Number NU84DD000006. These contents are solely the responsibility of the authors and do not necessarily represent the official views of the CDC, the US Department of Health and Human Services, or the University of Alaska Anchorage Institute of Social and Economic Research.
Womens Healthcare. 2023;11(2):12-15. doi: 10.51256/WHC042312
References
1 Substance Abuse and Mental Health Services Administration. 2020 National Survey on Drug Use and Health: Detailed Tables. January 11, 2022. www.samhsa.gov/data/report/2020-nsduh-detailed-tables.
2 Centers for Disease Control and Prevention. Excessive alcohol use is a risk to women’s health. October 17, 2022. www.cdc.gov/alcohol/fact-sheets/womens-health.htm.
3 National Institute on Alcohol Abuse and Alcoholism. Women and alcohol. Updated September 2022. www.niaaa.nih.gov/publications/brochures-and-fact-sheets/women-and-alcohol.
4 Denny CH, Acero CS, Terplan M, Kim SY. Trends in alcohol use among pregnant women in the U.S., 2011–2018. Am J Prev Med. 2020;59(5);768-769.
5 Gosdin LK, Deputy NP, Kim SY, et al. Alcohol consumption and binge drinking during pregnancy among adults aged 18–49 years – United States, 2018–2020. MMWR Morb Mortal Wkly Rep. 2022;71(1):10-13.
6 Mattson SN, Bernes GA, Doyle LR. Fetal alcohol spectrum disorders: a review of the neurobehavioral deficits associated with prenatal alcohol exposure. Alcohol Clin Exp Res. 2019;43(6):1046-1062.
7 Hagan JF Jr, Balachova T, Bertrand J, et al, on behalf of Neurobehavioral Disorder Associated with Prenatal Alcohol Exposure Workgroup; American Academy of Pediatrics. Neurobehavioral disorder associated with prenatal alcohol exposure. Pediatrics. 2016;138(4):e20151553.
8 May PA, Chambers CD, Kalberg WO, et al. Prevalence of fetal alcohol spectrum disorders in 4 US communities. JAMA. 2018;319(5):474-482.
9 Bertrand J. Fetal alcohol spectrum disorders are clearly brain based. Dev Med Child Neurol. 2016;58(8):794-795.
10 Subbaraman MS, Thomas S, Treffers R, et al. Associations between state-level policies regarding alcohol use among pregnant women, adverse birth outcomes, and prenatal care utilization: results from 1972 to 2013 vital statistics. Alcohol Clin Exp Res. 2018;42:1511-1517.
11 Roberts SCM, Mericle AA, Subbaraman MS, et al. State policies targeting alcohol use during pregnancy and alcohol use among pregnant women 1985–2016: evidence from the Behavioral Risk Factor Surveillance System. Womens Health Issues. 2019;29(3):213-221.
12 Subbaraman MS, Roberts SCM. Costs associated with policies regarding alcohol use during pregnancy: results from 1972-2015 vital statistics. PLoS One. 2019;14(5):e0215670.
13 Bell E, Andrew G, Di Pietro N, et al. It’s a shame! Stigma against fetal alcohol spectrum disorder: examining the ethical implications for public health practices and policies. Public Health Ethics. 2016;9(1):65-77.
14 Roberts SCM, Berglas NF, Subbaraman MS, et al. Racial differences in the relationship between alcohol/pregnancy policies and birth outcomes and prenatal care utilization: a legal epidemiology study. Drug Alcohol Depend. 2019;201:244-252.
15 Olmstead TA, Yonkers KA, Ondersma SJ, et al. Cost-effectiveness of electronic- and clinician-delivered screening, brief intervention and referral to treatment for women in reproductive health centers. Addiction. 2019;114(9):1659-1669.
16 Chang G, McNamara TK, Orav EJ, et al. Brief intervention for prenatal alcohol use: a randomized trial. Obstet Gynecol. 2005;105(5 Pt 1):991-998.
17 Shogren MD, Harsell C, Heitkamp T. Screening women for at-risk alcohol use: an introduction to screening, brief intervention, and referral to treatment (SBIRT) in women’s health. J Midwifery Womens Health. 2017;62(6):746-754.
18 Chiodo LM, Cosmian C, Pereira K, et al. Prenatal alcohol screening during pregnancy by midwives and nurses. Alcohol Clin Exp Res. 2019;43(8):1747-1758.
19 O’Connor MJ, Whaley SE. Brief intervention for alcohol use by pregnant women. Am J Public Health. 2007;97(2):252-258.
20 US Preventive Services Task Force. Final recommendation statement. Unhealthy alcohol use in adolescents and adults: screening and behavioral counseling interventions. November 13, 2018. https://www.uspreventiveservicestaskforce.org/uspstf/recommendation/unhealthy-alcohol-use-in-adolescents-and-adults-screening-and-behavioral-counseling-interventions
21 Bohm MK, Liu Y, Esser MB, et al. Binge drinking among adults, by select characteristics and state – United States, 2018. MMWR Morb Mort Wkly Rep. 2021;70(41):1441-1446.
22 Centers for Disease Control and Prevention. Planning and Implementing Screening and Brief Intervention for Risky Alcohol Use: A Step-By-Step Guide for Primary Care Practices. Atlanta, GA: Centers for Disease Control and Prevention, National Center for Birth Defects and Developmental Disabilities; 2014. www.cdc.gov/ncbddd/fasd/documents/alcoholsbiimplementationguide.pdf.
23 Harris B. The role of public policy in advancing SBIRT implementation and dissemination. In: Cimini MD, Martin JL, eds. Screening, Brief Intervention, and Referral to Treatment for Substance Use: A Practitioner’s Guide. American Psychological Association; 2020:267-283.