
The rate of obesity in the United States continues to rise annually, and over one million pregnant individuals live with obesity. Obesity in pregnancy is associated with increased complications for both the pregnant person and the fetus. In addition to a higher risk of complications, pregnant patients with obesity are at risk for bias and discrimination from their community and healthcare providers. This article addresses the incidence and impact of obesity on the pregnant person and fetus, while also addressing ways to reduce bias in caring for this patient population.
Womens Healthcare. 2022;10(3):35-40. doi: 10.51256/WHC062235
Obesity in pregnancy is common in the United States, with over one million pregnant individuals living with obesity and the rates continuing to rise.1–3 The incidence of obesity in pregnancy in the US is estimated to be as high as 1 in 2 pregnancies, with the definition of obesity (a body mass index [BMI] > 30 kg/m2) being the same for both nonpregnant and pregnant individuals.4 The most noticeable recent increase in obesity has been in the most severe class, defined as a BMI greater than 40 kg/m2.4,5 This increase in obesity is important for providers to grasp because of the increased rate of specific poor outcomes during pregnancy (Table 1).

On top of these medical risks, pregnant patients with obesity are subject to stigma and bias from society and healthcare providers, which also can be damaging to maternal health and wellbeing.6,7
According to the Pregnancy Risk Assessment Monitoring System, 25.3% of US females have obesity prior to conception.8Differences are seen across racial groups in the rate of obesity both before and during pregnancy, and populations of color have a higher incidence of obesity than their White counterparts.4 For example, pregnant persons of Latinx/Hispanic heritage have the highest rate of obesity in pregnancy and Black women are more likely to have severe obesity in pregnancy.3,4 Other factors that affect the risk of a pregnant person having obesity are a rural living location and working at sedentary jobs.3,4
Pregnancy complicated by obesity has been seen as inherently high risk and therefore necessitating high-risk physician care. A growing body of research, however, supports nurse practitioners and certified nurse-midwives caring for this population independently or in partnership with physicians.9,10 Whereas traditional obstetric care centers around treating pregnancy as an illness and using medical tests to discover potential complications, research indicates that care under this model is often not evidence driven and does not necessarily improve outcomes.11 For example, past recommendations for fetal surveillance were to monitor those with obesity in pregnancy with regular fetal nonstress tests and ultrasounds in the third trimester.
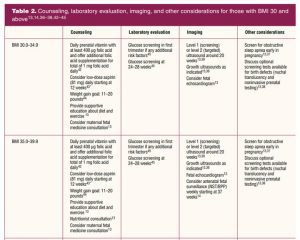
The recommended gestational age to begin this surveillance varied greatly, and in their 2015 Practice Bulletin on obesity in pregnancy, the American College of Obstetricians and Gynecologists (ACOG) acknowledged that antenatal surveillance does not necessarily lead to better outcomes. The bulletin notes that “there is no evidence showing a clear improvement in pregnancy outcomes with antepartum surveillance, and a recommendation cannot be made for or against routine antenatal fetal surveillance in obese pregnant women.”12 In 2021 ACOG replaced these guidelines, offering slightly more concrete suggestions for antenatal testing (Table 2).

Clinicians, however, still struggle with conflicting recommendations and information for this patient population.13,14 Currently, no consistent recommendations exist as to when to begin this fetal testing, and a common practice is to begin any time between 28 and 37 weeks, which can lead to confusion with the plan of care for both clinician and patient.15 This conflict can be resolved by following evidence-based practice and involving the patient in shared decision making with an unbiased approach.
Reducing size bias and providing evidence-based care
Ideally, anyone planning pregnancy should have a preconception discussion with a provider well before pregnancy. Although this visit does not always occur as a formal preconception visit, if the provider can counsel the patient on healthy choices before pregnancy is achieved, complications could potentially be minimized or avoided. Given that a formal preconception visit is uncommon, the initial prenatal visit provides an opportunity for the provider to establish rapport and convey important information on healthy lifestyle choices, nutrition, and exercise. For individuals with obesity, this can include compassionate counseling on healthy choices.
By providing specific advice on healthy food choices and exercise in an inclusive manner, the provider and patient can focus on health promotion and shared decision making—which has been shown to improve outcomes.16 Table 1 discusses potential complications for those with a BMI of 30 kg/m2 and above, and Table 2 provides appropriate counseling, laboratory evaluation, and imaging for these individuals. The recommendations in the tables are categorized by BMI ranges and can serve as an easy reference point for counseling patients.
Clinicians must also recognize that in addition to having a higher risk of some physical complications, pregnant patients with obesity are at risk for bias and discrimination.17 Indeed, negative bias toward pregnant individuals with obesity may contribute to the poor outcomes that are increased in this patient population.17 The stigma surrounding the diagnosis of obesity can be seen in past recommendations in which pregnancy care was heavily focused on intervention for patients with a BMI over 30 kg/m2.12,18 The current recommendations focus on collaboration between low-and high-risk providers, and the result of this trend toward collaborative practices has improved patient outcomes.9,19
In support of this, a growing body of research shows improved outcomes when the pregnant person has access to the Midwifery Model of Care—a model very familiar to women’s health nurse practitioners.1,9,20 The midwifery model emphasizes relationship-focused and nonjudgmental care.21 It offers an alternative to traditional obstetric care that is patient led, and in which translation and discussion of evidence is highly valued. Because of the relationship-based care provided in the midwifery model, a trusting relationship is formed with the patient, which promotes wellness and positive birth outcomes across patient populations.20,21 This improvement in birth outcomes can have a significant impact on the overall health of the pregnant person, the fetus, and the family. It is crucial for clinicians to grasp patient-centered prenatal care, have a concrete understanding of the evidence-based recommendations, and to actively employ strategies to reduce the bias and discrimination often aimed at these patients.
Effective bias interventions must increase awareness about implicit biases, build motivation to reduce that bias, and give providers evidence-based strategies for countering their own biases.22 Additionally, beliefs and stereotypes about obesity are most likely to change when individuals can change their attributions about the causes and controllability of weight.23 One key tactic here is decoupling weight and health in healthcare education.24 As one author argues, better training for clinicians must “confront the framing of fat bodies as dreaded and despised,” which requires a shift toward humanizing and embracing obesity.25 A weight-inclusive approach emphasizes viewing health and wellbeing as multifaceted and not linking weight and weight loss in defining health and wellbeing (a weight-normative approach).26 In contrast to a weight-normative approach, which stigmatizes weight and is not effective for sustainable improved health, a weight-inclusive framework has been demonstrated to improve physical, behavioral, and psychological indicators of health. A paradigm shift from weight-normative to weight-inclusive will centralize health across the weight continuum and redress weight bias in providers.26
A health-based approach will focus on health promotion through shared decision making and patient education without centering weight.27 Healthcare providers must “learn and adopt less stigmatizing ways of interacting with the fat body and with fat people.”7 Providers can start by being aware of the biases that exist and actively work to care for pregnant persons in ways that are not rooted in shame and blame.28 A critical step in reducing stigmatizing communication and weight bias in pregnancy is to center the voices of women who are overweight or obese. This includes the importance of sensitive communication, individualized care regarding weight, and reduced focus on body weight by focusing on comorbidities and other health indicators.6 For example, gestational weight gain is a key topic of conversation. Because weight bias is so pervasive, patients are likely to enter clinical encounters expecting their providers to be biased, making these patients particularly sensitive to the words and actions of their care providers.29
Thus, in discussing weight gain during pregnancy, providers can emphasize vital health information, communicate understanding and respect, and be particularly sensitive in conversations about weighing the patient, bringing up the subject of body weight, providing weight-related advice, and managing patients’ emotions.29 Messages regarding nutrition and exercise during pregnancy should be consistent, unambiguous, and avoid misconceptions and myths.30
Finally, to truly address the damaging effects of weight bias on women’s experiences, we must think intersectionally, understanding the merging identities and social structures that affect women’s lived experiences during prenatal care. We must acknowledge that weight bias does not exist independently of sexism, racism, ableism, homophobia, classism, etc., and will certainly affect pregnant individual’s clinical encounters and physical/emotional outcomes during and after pregnancy.31,32
Conclusion and implications for practice
The potential risks of pregnancy complicated by obesity are well documented, but management of these pregnancies has changed significantly in recent years. Historically, a diagnosis of obesity would have meant a pregnant person risked out of prenatal care by nurse practitioners. This is not always the case presently, and the choice of care model is often patient driven. Additionally, there has been a significant rise in the number of nurse practitioners in the US who will encounter pregnant patients with obesity within their practices, so it is vital for these clinicians to know the latest recommendations for pregnant patients with obesity. It is important that all prenatal providers acknowledge biases held toward this patient population both by society and healthcare professionals and to be ready to employ strategies to reduce bias toward patients with obesity. This helps to build trust and establishes a positive relationship with a patient, which in turn can enhance the pregnant person’s ability to make healthy choices throughout pregnancy.
Ellen C. Solis is on staff of Carle Midwifery Services in Urbana, Illinois, and at the University of Illinois, Chicago School of Nursing. Elizabeth G. Muñoz is on staff of Carle Midwifery Services in Urbana, Illinois, and at the University of Illinois, Chicago School of Nursing. Amy L. Delaney is Director of Diversity, Equity, and Inclusion at Carle Health at the University of Illinois at Urbana-Champaign. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
References:
- Centers for Disease Control and Prevention. Pregnancy complications. 2018.
- Hales CM, Carroll MD, Fryar CD, Ogden CL. Prevalence of obesity among adults and youth: United States, 2015–2016. NCHS Data Brief No. 288; October 2017. Centers for Disease Control and Prevention. National Center for Health Statistics (NCHS).
- Chen C, Xu X, Yan Y. Estimated global overweight and obesity burden in pregnant women based on panel data model. PLoS One. 2018;13(8):e0202183.
- National Center for Health Statistics, 2020. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017-2018.
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion: Ethical considerations for the care of patients with obesity. 2019.
- Nagpal TS, da Silva DF, Liu RH, et al. Women’s suggestions for how to reduce weight stigma in prenatal clinical settings. Nurs Womens Health. 2021;25(2):112-121.
- Ward P, McPhail D. Fat shame and blame in reproductive care: implications for ethical health care interactions. Womens Reproductive Health. 2019;6(4):225-241.
- PRAMS. Prevalence of selected maternal and child health indicators for all PRAMS sites. 2017.
- Carlson NS, Breman R, Neal JL, Phillippi JC. Preventing cesarean birth in women with obesity: influence of unit-level midwifery presence on use of cesarean among women in the Consortium on Safe Labor data set. J Midwifery Womens Health. 2019;65(1):22-32.
- Centers for Disease Control and Prevention. Cesarean delivery rate by state. 2020.
- Our Bodies, Ourselves. Models of maternity care. 2014.
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin no. 156. Obesity in pregnancy. Obstet Gynecol. 2015;126(6):e112-e126.
- American College of Obstetricians and Gynecologists. ACOG Practice Bulletin no. 230. Obesity in pregnancy. Interim update. Obstet Gynecol. 2021;137(6):e128-e144.
- American College of Obstetricians and Gynecologists. ACOG Committee Opinion no. 828. Indications for outpatient antenatal fetal surveillance. Obstet Gynecol. 2021;137(6):e177-e197.
- Vitner D, Harris K, Maxwell C, Farine D. Obesity in pregnancy: a comparison of four national guidelines. J Matern Fetal Neonatal Med. 2019;32(15):2580-2590.16.
- Healthit.gov. What is shared decision making? Shared decision making.
- DeJoy SB, Bittner K. Obesity stigma as a determinant of poor birth outcomes in women with high BMI: a conceptual framework. Matern Child Health J. 2015;19(4):693-699.
- Hanneman N, Sarker M, Caughey AB, Valent AM. Influence of obesity on maternal and neonatal outcomes in advanced maternal age women [22D]. Obstet Gynecol. 2020;135:44S.
- Reither M, Germano E, DeGrazia M. Midwifery management of pregnant women who are obese. J Midwifery Womens Health. 2018;63(3):273-282.
- American College of Nurse-Midwives. 2020.
- American College of Nurse-Midwives. Core competencies for basic midwifery practice. 2020.
- Hagiwara N, Kron FW, Scerbo MW, Watson GS. A call for grounding implicit bias training in clinical and translational frameworks. Lancet. 2020;395(10234):1457.
- Poustchi Y, Saks NS, Piasecki AK, et al. Brief intervention effective in reducing weight bias in medical students. Family Med. 2013;45(5):345.
- Ramos Salas X, Alberga AS, Cameron E, et al. Addressing weight bias and discrimination: moving beyond raising awareness to creating change. Obesity Rev. 2017;18(11):1323-1335.
- Fahs B. Fat and furious: interrogating fat phobia and nurturing resistance in medical framings of fat bodies. Womens Reproductive Health. 2019;6(4):245-251.
- Tylka TL, Annunziato RA, Burgard D, et al. The weight-inclusive versus weight-normative approach to health: evaluating the evidence for prioritizing well-being over weight loss. J Obesity. 2014;(983495).
- Zielinski RE. BMI and pregnancy/childbirth: risk reduction or fat shaming? Womens Reproductive Health. 2019;6(4):242-244.
- Christenson A, Johansson E, Reynisdottir S, et al. “… or else I close my ears” How women with obesity want to be approached and treated regarding gestational weight management: a qualitative interview study. PloS One. 2019;14(9):e0222543.
- Furness PJ, McSeveny K, Arden MA, et al.Maternal obesity support services: a qualitative study of the perspectives of women and midwives. BMC Pregnancy Childbirth. 2011;11(1):1-11.
- Green TL, Zapata JY, Brown HW, Hagiwara N. Rethinking bias to achieve maternal health equity: changing organizations, not just individuals. Obstet Gynecol. 2021;37(5):935.
- Kinavey H, Cool C. The broken lens: how anti-fat bias in psychotherapy is harming our clients and what to do about it. Women Ther. 2019;42(1-2):116-130.
- Molyneaux E, Poston L, Ashurst-Williams S,Howard LM. Obesity and mental disorders during pregnancy and postpartum: a systematic review and meta-analysis. Obstet Gynecol. 2014;123(4):857-867.
- Kongubol A, Phupong V. Prepregnancy obesity and the risk of gestational diabetes mellitus. BMC Pregnancy Childbirth. 2011;11:59.
- Schummers L, Hutcheon JA, Bodnar LM, et al. Risk of adverse pregnancy outcomes by prepregnancy body mass index: a population-based study to inform prepregnancy weight loss counseling. Obstet Gynecol. 2015;125(1):133-143.
- Sohlberg S, Stephansson O, Cnattingius S, Wikstrom AK. Maternal body mass index, height, and risks of preeclampsia. Am J Hypertens. 2012;25:120-125.
- McDonald SD, Han Z, Mulla S, Beyene J; Knowledge Synthesis Group. Overweight and obesity in mothers and risk of preterm birth and low birth weight infants. Obstet Anesthesia Dig. 2011;31(3):158-159.
- Izci-Balserak B. Sleep-disordered breathing in pregnancy. Part 1. Am J Respir Crit Care Med. 2019;200(9):18-19.
- Stothard KJ, Tennant PW, Bell R, Rankin J. Maternal overweight and obesity and the risk of congenital anomalies: a systematic review and meta-analysis. JAMA. 2009;301:636-650.
- Salihu HM, Dunlop AL, Hedayatzadeh M, et al. Extreme obesity and risk of stillbirth among black and white gravidas. Obstet Gynecol. 2007;110:552-557.
- Blomberg M. Maternal obesity and risk of postpartum hemorrhage. Obstet Gynecol. 2011;118(3):561-568.
- Garner CD, McKenzie SA, Devine CM, et al. Obese women experience multiple challenges with breastfeeding that are either unique or exacerbated by their obesity: discoveries from a longitudinal, qualitative study. Matern Child Nutr. 2017;13(3):e12344.
- Chitayat D, Matsui D, Amitai Y, et al. Folic acid supplementation for pregnant women and those planning pregnancy: 2015 update. J Clin Pharmacol. 2016;56(2):170-175.
- American College of Obstetricians and Gynecologists. Committee Opinion no. 743. Low-dose aspirin use during pregnancy. Obstet Gynecol. 2018;132(1):e44-e52.
- Institute of Medicine. Weight Gain during Pregnancy: Reexamining the Guidelines. Washington, DC: National Academies Press; 2009.
- American College of Obstetricians and Gynecologists. Gestational diabetes mellitus. Practice Bulletin no. 190. Obstet Gynecol. 2018;131(2):e49-e64.
Key words: pregnancy, overweight, obesity, complications, intervention, bias, discrimination
Womens Healthcare. 2022;10(3):35-40. doi:10.51256/WHC062235