The National Association of Nurse Practitioners in Women’s Health (NPWH) advocates for the use of evidence-based strategies by women’s health nurse practitioners (WHNPs) and other advanced practice registered nurses (APRNs) who provide healthcare for reproductive-age women to prevent alcohol-exposed pregnancies (AEPs). Foremost is the strategy of universal screening for alcohol use in primary care settings for all adult patients age 18 years or older, including pregnant women.1,2 Strategies also extend to offering a brief behavioral intervention to individuals who screen positive for excessive alcohol use and referrals to specialty services as needed with appropriate follow-up. See Box 1 for parameters of excessive alcohol use.
The prevention of AEPs requires the provision of fact-based information about the risks of alcohol use during pregnancy. All sexually active women of reproductive age who could become pregnant and who drink alcohol need to be counseled about the potentially harmful effects of alcohol on a developing fetus. It is important also to advise them to use effective contraception to prevent pregnancy or to stop drinking alcohol. Women who are pregnant or trying to get pregnant need to be advised to abstain from drinking alcohol. Public awareness campaigns have the potential to reach a wider audience with this information, including women’s partners and families.
NPWH recognizes that early and regular prenatal care for women with alcohol dependence is essential to encourage healthy behaviors and provide support and early treatment referrals to reduce risks of harm. State laws and policies that require reporting of alcohol/substance abuse during pregnancy as potential child abuse or neglect may deter women with alcohol dependence from seeking prenatal care.2,3 Therefore, NPWH opposes laws and policies that threaten civil or criminal sanctions and/or that require reporting alcohol/substance abuse during pregnancy.
NPWH provides leadership and collaborates with other organizations and agencies to deliver education and skills training for WHNPs and other APRNs who provide healthcare for reproductive-age individuals, promote public awareness campaigns, advocate repeal of laws and policies that deter women with alcohol dependence from seeking prenatal care, and support research in a concerted effort to prevent AEPs.
BACKGROUND
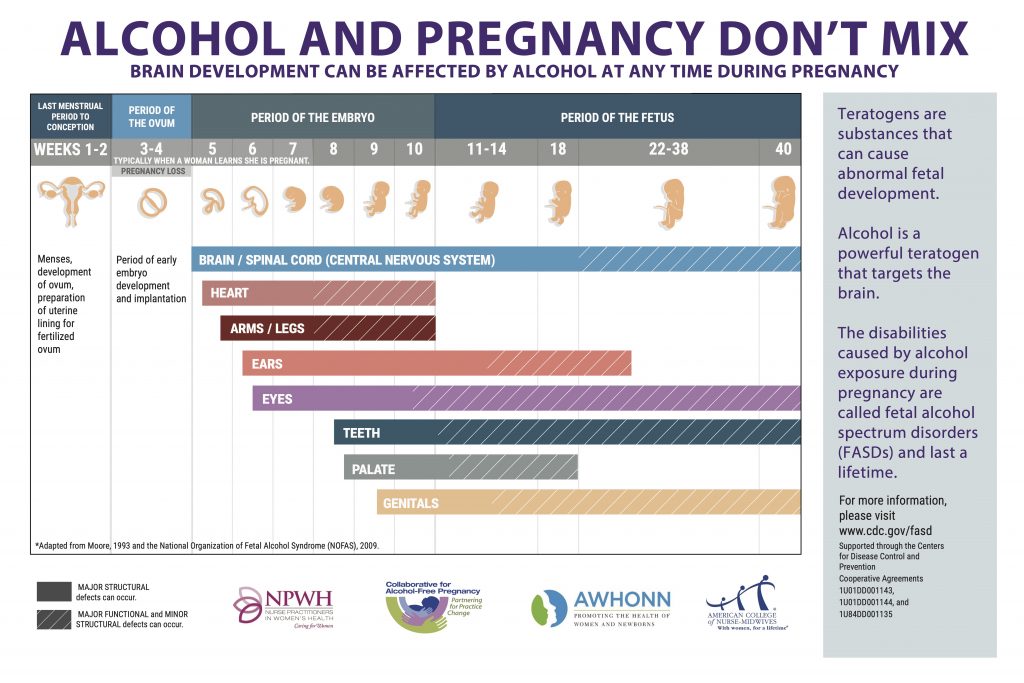
Prenatal alcohol exposure is a major preventable cause of birth defects and intellectual and developmental disabilities. Alcohol, a known teratogen, readily crosses the placenta and accumulates in amniotic fluid. A slower elimination rate (3%–4% of maternal rate) results in a prolonged effect on the fetus.4 Toxicity is dose related, with the greatest risk to the fetus in the first trimester.5 The developing fetal brain, however, is vulnerable to the influence of any alcohol throughout pregnancy.5 The umbrella term fetal alcohol spectrum disorders (FASDs) describes a range of possible effects that include physical, intellectual, behavioral, and learning disabilities and language delays, with lifelong implications for individuals prenatally exposed to alcohol.6 Based on community studies funded by the National Institutes of Health, experts estimate the prevalence of FASDs as high as 1 to 5 per 100 school children.7 In addition to FASDs, alcohol use during pregnancy is associated with increased risks for spontaneous abortion, intrauterine growth restriction, stillbirth, preterm birth, and sudden infant death syndrome.8 With regard to preventing FASDs and other adverse pregnancy and birth outcomes associated with prenatal alcohol exposure, there is no known safe amount of alcohol use at any time during pregnancy. FASDs are completely preventable if alcohol is not consumed during pregnancy.
In 2005, the Surgeon General advised pregnant women to not drink any alcohol, pregnant women who have already consumed alcohol to stop doing so, and women considering becoming pregnant to abstain from drinking alcohol.9 Despite this recommendation, the number of women who drink alcohol while pregnant remains at significant levels. Approximately 1 in 9 (11.5%) pregnant women report drinking some amount of alcohol in the past month and, of those, about one-third (3.9%) report binge drinking.10 Women who binge drink before pregnancy are more likely to drink and binge drink during pregnancy than are women who do not binge drink before pregnancy.10 The high blood alcohol concentrations associated with binge drinking may be particularly harmful to fetal brain development, especially in the cognitive domain.11
The fact that about one-half of all pregnancies are unplanned poses a particular challenge to the prevention of AEPs. Approximately 3.3 million reproductive-age women report drinking alcohol in the past month and having sex without using contraception.12 The stigma related to drinking alcohol during pregnancy can create a barrier to being forthright about alcohol use or seeking help, especially when the individual fears discrimination or legal consequences. As well, healthcare providers report concerns about stigmatizing patients as a barrier to screening.13,14
Strong evidence suggests that alcohol screening and brief intervention (SBI) is effective in reducing excessive alcohol use among women of childbearing age, including pregnant women.15–17 Leading healthcare organizations and agencies in the United States, including NPWH, US Preventive Services Task Force, American College of Obstetricians and Gynecologists, and the Centers for Disease Control and Prevention (CDC), recommend that alcohol SBI be implemented for all adults in primary care settings.1,2,18 All pregnant women need to be screened at the first prenatal visit.1,2,18 An expert panel convened by the CDC recommends screening to be repeated at least every trimester for individuals identified as at risk (eg, high use in past including recent treatment, stopped late in pregnancy, continued low level of use).16
Alcohol SBI uses a validated screening tool to identify a woman’s drinking patterns, whether her alcohol consumption is creating a health risk for herself or others, and whether she has symptoms of dependency. If excessive drinking is identified, the provider engages the woman in a brief motivation-enhancing intervention to reduce drinking. The main goal of alcohol SBI is to motivate patients to be aware of their alcohol consumption patterns, understand the associated risks and options for reducing or eliminating the risk, and make their own decisions. Referral to specialty care for further assessment and treatment is offered if a woman is unable to moderate excessive alcohol use on her own.18 See Box 2 for resources on alcohol SBI.
RECOMMENDATIONS
NPWH affirms that WHNPs and other APRNs who provide healthcare for women of reproductive age have a crucial role in preventing alcohol-exposed pregnancies. They have opportunities to educate women about the risks associated with drinking alcohol during pregnancy at encounters for well-woman, prepregnancy, contraception, prenatal, and other healthcare visits.
NPWH recommends that WHNPs and other APRNs who provide healthcare for reproductive-age women:
- Adopt a nonjudgmental respectful approach when broaching the topic of alcohol use.
- Avoid stereotypes about individuals who drink in an excessive pattern.
- Use language that is not stigmatizing.
- Provide clear, fact-based information on risks associated with drinking alcohol during pregnancy.
- Consistently convey the message that there is no known safe amount of alcohol use at any time during pregnancy.
- Advise women who are pregnant or planning a pregnancy not to drink alcohol.
- Advise sexually active women who drink alcohol and could become pregnant to use effective contraception to prevent pregnancy or stop drinking.
- Screen all adults age 18 years and older including pregnant women for excessive alcohol use with a validated screening tool.
- Provide an evidence-based brief intervention if excessive alcohol use is identified.
- Provide follow-up as needed to monitor the individual’s alcohol use and provide encouragement and support.
- Recognize that not all individuals can stop alcohol use without specialized help.
- Offer referral for additional services as needed and know what services are available in the community.
- Know state reporting laws and policies for alcohol/ substance abuse in pregnancy.
NPWH also encourages WHNPs and other APRNs who provide healthcare for reproductive-age women to be leaders and change agents in their healthcare settings and communities to promote evidence-based strategies to prevent alcohol-exposed pregnancies.
NPWH recommends that WHNPs and other APRNs who provide healthcare for reproductive-age women:
- Champion universal alcohol use screening and brief interventions in their healthcare settings.
- Provide healthcare provider colleagues and students with fact-based information on the risks associated with drinking alcohol during pregnancy.
- Advocate for retraction of legislation that exposes pregnant women with alcohol dependence to criminal or civil penalties.
- Engage with professional organizations and community service providers to promote public awareness campaigns on risks associated with drinking alcohol during pregnancy and available resources.
NPWH LEADERSHIP
NPWH will provide leadership to ensure:
- Educational programs for WHNP and other APRN students, with a population focus that includes reproductive-age women, have resources to impart evidence-based knowledge and skill building for the development of competencies to conduct effective alcohol SBI to prevent or address alcohol use during pregnancy.
- Continuing education programs and resources are available to enhance knowledge and skills needed to convey nonjudgmental, fact-based information about alcohol use and conduct effective alcohol SBI to prevent or address alcohol use during pregnancy.
- Collaboration with professional organizations and community service providers to promote public awareness campaigns about the importance of abstaining from using alcohol during pregnancy.
- Public health policies and legislation regarding alcohol use during pregnancy do not threaten civil or criminal sanctions for alcohol use and/or require reporting.
- Research moves forward in all aspects for the prevention and reduction of harms from alcohol use during pregnancy.
BOX 1. EXCESSIVE ALCOHOL USE19
- Binge drinking (five or more drinks for men and four or more for women within a 2-hour time period)
- Heavy drinking (more than 14 drinks a week for men and more than seven drinks a week for women)
- Any alcohol consumption by pregnant women or people younger than age 21 years
BOX 2. ALCOHOL SCREENING AND BRIEF INTERVENTION RESOURCES
Centers for Disease Control and Prevention. Planning and Implementing Screening and Brief Intervention for Risky Alcohol Use: A Step-by-Step Guide for Primary Care Practices. Atlanta, GA: CDC National Center on Birth Defects and Developmental Disabilities; 2014. cdc.gov/ncbddd/fasd/documents/alcoholsbiimplementationguide.pdf.
Collaborative for Alcohol-Free Pregnancy. NPs, Midwives, and Nurses: Partnering to Prevent Fetal Alcohol Spectrum Disorders. www.sites.google.com/view/nursesmidwivespreventfasds/home.
Substance Abuse and Mental Health Services Administration.
USAUDIT: The Alcohol Use Disorders Identification Test, Adapted for Use in the United States. A Guide for Primary Care Practitioners. www.sbirt.webs.com/USAUDIT-Guide_2016_final-1.pdf.
Centers for Disease Control and Prevention. Fetal alcohol spectrum disorders (FASDs): training and education. April 30, 2020. www.cdc.gov/ncbddd/fasd/training.html.
REFERENCES
- US Preventive Services Task Force; Curry SJ, Krist AH, Owens DK, et al. Screening and behavioral counseling interventions to reduce unhealthy alcohol use in adolescents and adults: US Preventive Services Task Force recommendation statement.
JAMA. 2018;320(18):1899-1909. - American College of Obstetricians and Gynecologists. Committee on Health Care for Underserved Women. Committee opinion no. 496: At-risk drinking and alcohol dependence: obstetric and gynecologic implications. Reaffirmed 2013. Obstet Gynecol. 2011;118(2 pt 1):383-388.
- Seiler NM. Alcohol and pregnancy: CDC’s health advice and the legal rights of pregnant women. Public Health Rep. 2016;131(4):623-627.
- Gupta KK, Gupta VK, Shirasaka T. An update on fetal alcohol syndrome–pathogenesis, risks, and treatment. Alcoholism Clin Exp Res. 2016;40(8):1594-1602.
- Coles C. Critical periods for prenatal alcohol exposure: evidence from animal and human studies. Alcohol Health Res World. 1994;18(1):22-29.
- Sokel RJ, Delaney-Black V, Nordstrom B. Fetal alcohol spectrum disorder.
JAMA. 2003;290(22):2996-2999. - Centers for Disease Control and Prevention. Fetal alcohol spectrum disorders (FASDs). Data & statistics. February 4, 2021. www.cdc.gov/ncbddd/fasd/data.html.
- Bailey BA, Sokol RJ. Prenatal alcohol exposure and miscarriage, stillbirth, preterm delivery, and sudden infant death syndrome. Alcohol Res Health. 2011;34(1):86-91.
- US Department of Health and Human Services. U.S. Surgeon General Releases Advisory on Alcohol Use in Pregnancy. February 21, 2005.
http://come-over.to/FAS/SurGenAdvisory.htm. - Denny CH, Acero CS, Naimi TS, Kim SY. Consumption of alcoholic beverages and binge drinking among pregnant women age 18- 44 years–United States, 2015-2017. MMWR Morb Mortal Wkly Rep. 2019;68(16):365-368.
- Flak AL, Su S, Bertrand J, et al. The association of mild, moderate, and binge prenatal alcohol exposure and child neuropsychological outcomes: a meta-analysis. Alcohol Clin Exp Res. 2014;38(1):214-226.
- Green PP, McKnight-Eily LR, Tan CH, et al. Vital signs: alcohol-exposed pregnancies—United States, 2011-2013. MMWR Morb Mortal Wkly Rep. 2016;65(4):91-97.
- Chiodo LM, Cosmian C, Pereira K, et al. Prenatal alcohol screening during pregnancy by midwives and nurses. Alcohol Clin Exp Res. 2019;43(8):1747-1758.
- Shogren MD, Harsell C, Heitkamp T. Screening women for at-risk alcohol use: an introduction to screening, brief intervention, and referral to treatment (SBIRT) in women’s health. J Midwifery Womens Health. 2017;62(6):746-754.
- Bertholet N, Daeppen JB, Wietlisbach V, et al. Reduction of alcohol consumption by brief alcohol intervention in primary care: systematic review and meta-analysis. Arch Intern Med. 2005;165(9):986-995.
- Jonas DE, Garbutt JC, Amick HR, et al. Behavioral counseling after screening for alcohol misuse in primary care: a systematic review and meta-analysis for the U.S. Preventive Services Task Force. Ann Intern Med. 2012;157(9):645-654.
- Wright TE, Terplan M, Ondersma SJ, et al. The role of screening, brief intervention, and referral to treatment in the perinatal period. Am J Obstet Gynecol. 2016:215(5):539-547.
18. Centers for Disease Control and Prevention. Planning and Implementing Screening and Brief Intervention for Risky Alcohol Use: A Step-by-Step Guide for Primary Care Practices. Atlanta, GA: CDC National Center on Birth Defects and Developmental Disabilities; 2014. cdc.gov/ncbddd/fasd/documents/alcoholsbiimplementationguide.pdf.
19. Centers for Disease Control and Prevention. What is excessive alcohol use? www.cdc.gov/alcohol/pdfs/excessive_alcohol_use.pdf
Approved by the NPWH Board of Directors: July 25, 2016
Updated and reaffirmed by the Board of Directors: April 6, 2021