
Chlamydia trachomatis (CT) is among the most prevalent of all infectious diseases in the United States, with over 1.7 million reported cases and a steadily increasing rate of cases over the previous 5 years.1 CT infections in women are often asymptomatic and, if left
untreated, can cause pelvic inflammatory disease, ectopic pregnancy, and infertility.2 CT can be successfully treated with oral antibiotics.3
Research has shown that as many as 60% of men and 73% of women are reinfected with CT only 7 months after being treated for it.3 In order to prevent reinfection and further spread, providers must ensure not only that patients are being treated for CT but also their partners. This can be done by implementing the practice of expedited partner therapy (EPT), which is recommended by the Centers for Disease Control and Prevention (CDC) in states where it has been legalized.4
EPT is the process of giving certain patients being treated for CT an additional treatment regimen (in the form of additional medication or additional prescriptions to be filled) for each untreated partner in the past 60 days when the provider cannot reasonably assume that the partner(s) will seek treatment.4 Patient-delivered EPT (PDEPT) is a specific form of EPT in which the provider gives the patient extra medication doses. PDEPT is generally viewed as the preferable form of EPT, because clinics with readily available PDEPT packs are found to have a higher uptake of EPT.5
Project purpose
The overall purpose of this project was to implement PDEPT as the new standard of care at one clinic to increase the number of patients with CT whose partners received treatment from the clinic. The goal of this project was to align clinic PDEPT practices with the CDC EPT guidelines from the CDC. Prior to this project, PDEPT was rarely used, as no clinic protocol was established following its legalization in Florida. The clinic relied on unassisted partner referral as standard practice for partner treatment. In unassisted partner referral, patients have the responsibility of notifying the partner(s), with the hope that the partner(s) will receive treatment in a timely fashion. Although rates of CT infection have gradually increased over time in the US, states where EPT has been legalized show a slower rate increase, suggesting that EPT is more successful than unassisted partner therapy.6
Description of the setting and population
The project implementation site was a central Florida urban youth clinic that provided sexually transmitted infection (STI) testing and treatment, along with other reproductive services, for adolescents and young adults age 13 to 24 years. This clinic operated under the umbrella of a local university, where it was included in the department of adolescent medicine. Over the past 3 years, the urban youth clinic provided care to nearly 6,000 patients and CT was the most commonly diagnosed and treated STI at this clinic. For the purpose of this project, only patients age 18 years and older were considered for the administration of PDEPT. Clinic team members involved in this project included several physicians from both adolescent medicine and infectious disease specialties, as well as two advanced practice registered nurses (APRNs) and one registered nurse (RN).
Description of the quality improvement project
A clinical algorithm directing the indications and administration of PDEPT was created based on CDC guidelines current at the time of the project (Figure 1).4
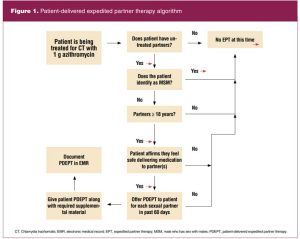
The algorithm presented a sequence of clinical decision prompts to ensure that eligible PDEPT patients were not missed and to confirm that each occurrence of PDEPT administration was appropriate and safe, including two questions important in helping to determine this: Does the patient identify as a male who has sex with males (MSM)? Does the patient affirm feeling safe delivering medication to partner(s)? Per CDC guidelines, EPT is not recommended in the MSM population due to their increased risk of contracting human immunodeficiency virus (HIV). Anyone who identifies as MSM should not be treated for an STI without being seen by a provider to ensure that HIV testing is completed.1 Additionally, this clinic works to ensure the safety and wellbeing of all patients, so each provider is instructed to verify whether each patient feels safe contacting previous partners prior to administering EPT.
Prior to implementation of the algorithm, clinic providers and staff were educated on its use, as well as the purpose, indications, and effects of successful EPT implementation. One day prior to the “go-live” date, educational material was presented virtually via a 30-minute PowerPoint presentation followed by distribution of the algorithm with time for discussion. The algorithm itself was hung in several different locations in the medical workroom where it was easily accessible by providers. The use of the algorithm and the decision to provide PDEPT was the responsibility of the provider, while the RN dispensed medication and provided the patient with educational material. Educational material provided to patients accepting EPT for each partner included clinic contact information with instructions on how to make an appointment, as well as treatment instructions, medication warnings (allergy, pregnancy), and the recommendation to seek testing and treatment with any STI-related symptoms.
This algorithm was implemented over a 6-week time period, while a simultaneous retrospective chart review for the prior 6-week period was done. The University of South Florida Institutional Review Board (IRB) determined that this quality improvement (QI) project was exempt from IRB review and approval, as research with human subjects was not involved.
Methods to evaluate outcomes
Data collection from both the pre- and post-implementation period was required to determine whether the implementation of the algorithm was able to increase the offering and patient acceptance of PDEPT, as compared to offering and acceptance of partner treatment prior to algorithm implementation. Patient charts were reviewed over the total 12-week period to determine the number of PDEPT-eligible patients as well as the number of patients who accepted PDEPT when it was offered. Supplementary descriptive statistics were collected including age, sex, race, and sexual orientation. Additionally, patients who were offered and accepted PDEPT for at least one partner during the implementation period agreed to be contacted via phone call by the clinic RN to verify whether the PDEPT was successfully delivered to the partner(s). Data were collected in a password-protected Excel workbook, in which names of qualifying patients were replaced with numbers to ensure that all personal health information remained protected.
Outcomes
In total, 17 patients were found to qualify for PDEPT during the implementation period. There was an increase in PDEPT being offered and accepted with implementation of the algorithm (Figure 2).
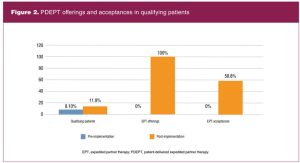
Reasons for refusal of PDEPT included feeling uncomfortable/unsafe approaching partner(s), inability to contact partner(s), and prior treatment of partner(s). In total, 10 patients accepted PDEPT and were given treatment for 12 untreated partners. Follow-up contact was made with each of the patients who accepted PDEPT, and delivery of medication to partners occurred at a rate of 91%.
Discussion and implications for practice
Although the efficacy of EPT has been proven, it is important that healthcare providers understand when and how to safely offer EPT to patients.5 One of the main barriers associated with the effective implementation of EPT is the legality of EPT, specifically regarding providers who are unaware of the legality or are unsure of how to offer EPT legally.7 This concern can be alleviated by visiting the CDC website, where the legality of EPT is broken down by state, along with resources to help facilitate the implementation of EPT. For more specific legal concerns, providers are encouraged to visit their individual state statutes, which should outline any restrictions regarding EPT. Healthcare providers and organizations can use a standardized algorithm to reference when determining whether EPT is indicated, so that each opportunity to offer EPT to a patient is recognized. Offering EPT to qualifying patients ensures that every patient receives the highest quality care, as directed by evidence-based practice guidelines.
Because medications at the project implementation site are supplied by the Department of Health, there was no negative financial impact associated with this project. Additionally, the offering and dispensing of PDEPT had minimal effects on workflow.
The biggest barrier to this project was that both the pre- and post-implementation periods occurred during the height of the Covid-19 pandemic. Because of this, the clinic had fewer patients than in prepandemic times. The effects of Covid-19 on STIs have yet to be understood. Furthermore, the pre-implementation period fell during the winter holidays, during which the clinic was closed for several days.
Conclusion
One limitation for this project was the short period of time for project implementation and the small number of patients who met criteria. Another limitation of the project was that only patients 18 years or older were included. The CDC does not restrict its EPT recommendations by age.4 Providers will need to know and follow their state regulations on STI treatment and EPT provision for patients under 18 years of age. This project warrants further implementation over a longer period of time with no restrictions on patient age.
Since the time of completion of this project the CDC has updated the STI treatment guidelines. First-line treatment for chlamydia is now 100 mg doxycycline orally twice daily for 7 days.8
These new guidelines will be reviewed to make any needed changes in treatment protocols and to explore the possibility of inclusion of indications and instructions for gonorrhea PDEPT as part of the algorithm.
In conclusion, the implementation of a specific algorithm directing PDEPT can be implemented to increase the rate of PDEPT offerings and subsequent acceptance by patients. This algorithm can be used by healthcare organizations and providers as a guide to successfully implement EPT in states where it is legal.
Shannon M. Nash is a nurse practitioner in Sarasota, Florida. Amy L. Weiss is Associate Professor, Pediatrics and Adolescent Medicine; and Lisa Istorico Sanders is Executive Director of the Ybor Youth Clinic, Department of Pediatrics, at the University of South Florida in Tampa, Florida. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
References
- Centers for Disease Control and Prevention. Sexually Transmitted Disease Surveillance 2018.
- Vacca SH, Salsgiver EL, Gold MA, Neu N. Patient-delivered expedited partner therapy for Chlamydia trachomatis infection among female adolescents using school-based health centers. J Pediatr Health Care. 2019;33(3):e18-e24.
- Gannon-Loew K, Holland-Hall C, Bonny AE. A review of expedited partner therapy for the management of sexually transmitted infections in adolescents. J Pediatr Adolesc Gynecol. 2017;30(3):341-348.
- Workowski KA, Bolan GA; Centers for Disease Control and Prevention. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(RR-03):1-137.
- Wong J, Zakher B, Consolacion T, et al. Facilitators and barriers to expedited partner therapy: results from a survey of family physicians. Sex Transm Dis. 2020;47(8):525-529.
- Mmeje O, Wallett S, Kolenic G, Bell J. Impact of expedited partner therapy (EPT) implementation on chlamydia incidence in the USA. Sex Transm Infect. 2017;94(7):545-547.
- Hopson LM, Opiola McCauley S. Expedited partner therapy: a review for the pediatric nurse practitioner. J Pediatr Health Care. 2017;31(5):525-535.
- Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187.