
{kind=link}
In this article, the author discusses the presentation and diagnosis of sexually transmitted infections at non-genital sites (eyes, mouth/throat, and skin) and conveys current recommendations for treatment.
According to the CDC, nearly 2.3 million cases of chlamydia, gonorrhea, and syphilis were diagnosed in the United States in 2017.1 This number surpassed the previous record set in 2016 by more than 200,000 cases and marked the fourth consecutive year of sharp increases in these sexually transmitted infections (STIs).1,2 These numbers regarding genital infections are likely low because many patients with STIs such as chlamydia or gonorrhea are asymptomatic and do not seek testing or treatment.1,2
Non-genital sites of infection are not included in the aforementioned CDC statistics, perhaps because many healthcare providers (HCPs) do not identify infections in their patients’ eyes, throat, or mouth as STIs or even consider rashes or other skin lesions as potential signs of STIs. One study showed that 13.8% of Chlamydia trachomatis infections and 30.3% of Neisseria gonorrhoeae infections in women would have been missed if testing of non-genital sites had not been done.3 A study of male college students showed that 26.4% of C. trachomatis infections and 63.2% of N. gonorrhoeae infections would have been missed if screening had not been performed at non-genital sites.4 Undiagnosed and untreated non-genital STIs are a potential reservoir for ongoing transmission and they may also lead to increased risk for HIV acquisition.
Are At-Home Test Kits Reliable?
CDC recommendations for providing quality STD clinical services
Challenges of testing for genital herpes
Background information
Sexually transmitted infections can occur as primary infections in non-genital areas such as the eyes, mouth/throat, or skin. In addition, systemic infections such as secondary syphilis or disseminated gonococcal infection (DGI) may present with non-genital signs and symptoms (S/S). When a patient with STI risk factors presents with ophthalmologic, oropharyngeal, or dermatologic S/S suggestive of an STI, assessment and testing for such infections should be considered.
Non-genital STIs may be transmitted through contact with another individual’s infected genital or anal mucosa or their semen or vaginal/cervical fluids, or they may be spread from a contaminated hand, finger, or sex toy.5 Non-genital infections may or may not be associated with a concomitant urogenital tract STI.5
Signs and symptoms of non-genital STIs
Like urogenital STIs, non-genital STIs can be asymptomatic or they can have characteristic manifestations.
Eyes
 Chlamydia trachomatis is the pathogen likely responsible for 20% of cases of bacterial conjunctivitis in adults.6 The most common means of transmission in these cases is accidental autoinoculation from an individual’s own genital infection.5 Sexually acquired chlamydial conjunctivitis can develop as a result of contact with another person’s infected genital secretions.7 Symptoms of chlamydial conjunctivitis gradually develop 1-3 weeks after exposure to the bacterium. Patients may present with complaints of unilateral itching, a sensation of sand scratching the surface of the eye, or a sensation of a foreign body’s presence in the eye, along with photophobia.8 Common examination findings include mucopurulent discharge, redness, tearing, swelling, matting of the eyelid, and a cobblestone appearance of the tarsal conjunctiva in the affected eye (Photograph 1). Tender enlarged pre-auricular lymph nodes may be noted.
Chlamydia trachomatis is the pathogen likely responsible for 20% of cases of bacterial conjunctivitis in adults.6 The most common means of transmission in these cases is accidental autoinoculation from an individual’s own genital infection.5 Sexually acquired chlamydial conjunctivitis can develop as a result of contact with another person’s infected genital secretions.7 Symptoms of chlamydial conjunctivitis gradually develop 1-3 weeks after exposure to the bacterium. Patients may present with complaints of unilateral itching, a sensation of sand scratching the surface of the eye, or a sensation of a foreign body’s presence in the eye, along with photophobia.8 Common examination findings include mucopurulent discharge, redness, tearing, swelling, matting of the eyelid, and a cobblestone appearance of the tarsal conjunctiva in the affected eye (Photograph 1). Tender enlarged pre-auricular lymph nodes may be noted.
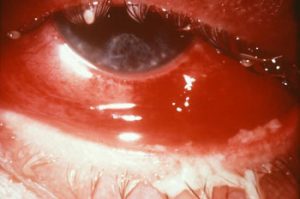 Symptoms of eye infection caused by N. gonorrhoeae are similar to those caused by C. trachomatis but are likely to have a sudden, rather than gradual, onset; to be more severe; and to be bilateral.9 Photograph 2 shows gonorrheal conjunctivitis. Patients with N. gonorrhoeae-related keratitis or corneal infection may also experience moderate to severe eye pain, decreased visual acuity, corneal clouding, and a ciliary flush. Untreated gonococcal conjunctivitis can lead to complications such as corneal perforation, endophthalmitis, and blindness.5
Symptoms of eye infection caused by N. gonorrhoeae are similar to those caused by C. trachomatis but are likely to have a sudden, rather than gradual, onset; to be more severe; and to be bilateral.9 Photograph 2 shows gonorrheal conjunctivitis. Patients with N. gonorrhoeae-related keratitis or corneal infection may also experience moderate to severe eye pain, decreased visual acuity, corneal clouding, and a ciliary flush. Untreated gonococcal conjunctivitis can lead to complications such as corneal perforation, endophthalmitis, and blindness.5
If Treponema pallidum, the bacterium causing syphilis, infects the eye, it can cause inflammation of the conjunctiva, cornea, uvea (inner coat of the eye), episclera (outer coat of the eye), optic nerve, or retina.10 Intraocular inflammation or uveitis is the most common manifestation of ocular syphilis.11 Because of the variation in presentation, patients may complain of blurry vision, double vision, eye pain, floaters, foreign body sensation, or light sensitivity. If these symptoms persist, causing damage to eye structures, then serious, long-lasting visual problems may ensue. If coexisting neurologic S/S are observed (e.g., cognitive dysfunction, sensorimotor deficits, ophthalmic or auditory symptoms, cranial nerve palsies, S/S of meningitis or stroke), cerebrospinal fluid (CSF) testing should be performed.
Mouth/throat
 Most chlamydial and gonorrheal infections of the throat are asymptomatic, but they may manifest with mild soreness or with discomfort when swallowing food.12 Photograph 3 shows chlamydial pharyngitis and Photograph 4, gonorrheal pharyngitis. Examination may reveal pharyngeal erythema and possibly mucopurulent exudate, white spots, and bilateral cervical lymphadenopathy.12 Untreated chlamydial or
Most chlamydial and gonorrheal infections of the throat are asymptomatic, but they may manifest with mild soreness or with discomfort when swallowing food.12 Photograph 3 shows chlamydial pharyngitis and Photograph 4, gonorrheal pharyngitis. Examination may reveal pharyngeal erythema and possibly mucopurulent exudate, white spots, and bilateral cervical lymphadenopathy.12 Untreated chlamydial or  gonorrheal pharyngitis, even if asymptomatic, can be passed to sexual partners through oral sex; in addition, the pharynx may be the site of antibiotic-resistant gonorrhea strains.3
gonorrheal pharyngitis, even if asymptomatic, can be passed to sexual partners through oral sex; in addition, the pharynx may be the site of antibiotic-resistant gonorrhea strains.3
A chancre associated with primary syphilis may develop 10 90 days after exposure at the area of treponemal entry, which may involve the lips (Photograph 5), tongue, gums, or oral mucosa. Typical chancres are painless, indurated, eroded, and a few millimeters to 2 cm in diameter. They may appear red, yellow, or gray. Nontender, enlarged, firm submandibular,  submental, and cervical lymph nodes may be present. Most chancres resolve in 2-8 weeks without treatment.10
submental, and cervical lymph nodes may be present. Most chancres resolve in 2-8 weeks without treatment.10
Oral mucous membrane lesions or mucous patches are a common manifestation of secondary syphilis (Photograph 6). These lesions present as nontender plaques or oval ulcerations. They may be white,  gray, or red. They appear about 6 weeks after onset of the primary chancre and resolve in 2-10 weeks, but they may recur if the infection is not treated.13
gray, or red. They appear about 6 weeks after onset of the primary chancre and resolve in 2-10 weeks, but they may recur if the infection is not treated.13
Skin
Disseminated gonococcal infection is a rare systemic complication of untreated gonorrhea. Patients with DGI may present with fever, rash, and painful swollen joints—most commonly pauciarticular arthritis of the wrists, fingers, elbows, knees, or ankles.14 Photograph 7 depicts a DGI rash of the foot. The rash typically appears as pink or red macules  on the extremities and, over time, may progress to pustules and petechiae and then to tender hemorrhagic abscesses, cellulitis, necrotizing fasciitis, and vasculitis.14
on the extremities and, over time, may progress to pustules and petechiae and then to tender hemorrhagic abscesses, cellulitis, necrotizing fasciitis, and vasculitis.14
Although the external genitalia are the most frequent site of syphilis infection, primary lesions around and/or in the anal canal and mouth are not uncommon. In addition, T. pallidum can gain entry through small abrasions in areas of the body where hair is shaved (e.g., the pubic area, upper aspects of the trunk).15 Secondary syphilis is often characterized by skin rash, mucocutaneous lesions, and lymphadenopathy 4-8 weeks after onset of the primary lesion. Most notable is a maculopapular, non-itchy eruption on the face, trunk, and/or extremities, including the palms and soles.15 Circular lesions around body orifices such as the genital area, perianal area, and mouth are typical of secondary-stage syphilis.
Diagnostic testing
Some laboratories have met regulatory requirements for using nucleic acid amplification testing (NAAT) on oropharyngeal specimens. However, NAAT is not yet FDA cleared for general use in detecting C. trachomatis or N. gonorrhoeae at non-genital sites16 Instead, culture is the current CDC-recommended testing modality for both C. trachomatis and N. gonorrhoeae at non-genital sites5 Use of Gram stain on oropharyngeal specimens for detection of gonococcal infection is not recommended.5
If an infection of the conjunctiva with C. trachomatis or N. gonorrhoeae is suspected, a specimen from an everted lid collected using a Dacron swab should be sent for culture. Special culture media are required.5 Identification of intracellular Gram-negative diplococci on Gram stain of conjunctival exudate justifies presumptive treatment for gonorrhea while awaiting culture and antimicrobial susceptibility testing results.17
Current CDC recommendations for testing should be followed when non-genital manifestations of primary or secondary syphilis are present.18 This process may include dark-field microscopy of non-genital chancres or other lesions and serologic testing.
Treatment
Current CDC guidelines regarding treatment of non-genital chlamydia, gonorrhea, and syphilis are similar to those treating urogenital infections. Of note, ocular syphilis is treated with a different approach.
Eyes
Because of its high prevalence and association with genital tract infection, chlamydial conjunctivitis should be treated systemically with oral antibiotics.19 The World Health Organization advocates use of oral azithromycin as part of its SAFE (Surgery for trichiasis [inturned eyelashes], Antibiotics, Facial cleanliness, and Environmental improvement) strategy for control of trachoma worldwide.20 The CDC recommends a single dose of azithromycin 1 g orally OR a 7-day course of doxycycline 100 mg orally twice daily.5
Few studies have been conducted on the treatment of gonococcal conjunctivitis in adults. Based on a 1989 study, participants responded to a single intramuscular (IM) injection of ceftriaxone 1 g.21 Because of antibiotic resistance problems with gonorrhea, dual treatment with ceftriaxone 1 g IM PLUS one dose of azithromycin 1 g orally may improve treatment efficacy and potentially slow the emergence of resistant bacteria.5 Addition of one-time lavage of the infected eye with saline solution is recommended, and referral to an eye specialist is advised.
Treatment for ocular syphilis is aqueous crystalline penicillin G 18-24 million U/day, administered as 3-4 million U intravenously (IV) every 4 hours or by continuous IV infusion for 10-14 days.18 For patients considered likely to be compliant, an alternate regimen of penicillin G procaine 2.4 million U/day IM and probenecid 500 mg orally 4 times daily, both for 10-14 days, is recommended.18
Mouth/throat
Whereas a single dose of azithromycin has been effective in treating urogenital chlamydial infection, doxycycline may have a slightly greater efficacy for pharyngeal chlamydial infection.22 Single-dose azithromycin may not lead to sustained drug concentrations capable of curing non-genital infection. The CDC recommendation for oropharyngeal chlamydia is either one dose of azithromycin 1 g orally OR doxycycline 100 mg orally twice daily for 7 days.5
Gonococcal infections of the pharynx, as compared with urogenital and anorectal sites, are more difficult to eliminate.5 The CDC still recommends treating N. gonorrhoeae-related pharyngeal infection with a single dose of ceftriaxone 250 mg IM PLUS a single dose of azithromycin 1 g orally.5 Retesting for urogenital or non-genital infections less than 3 weeks post-treatment is not recommended and can result in false-positive results because of the highly sensitive nature of NAAT and the possibility of detection of nonviable organisms.
Syphilis
For treatment of primary or secondary syphilis in adults, including pregnant women, the CDC recommends benzathine penicillin G 2.4 million U IM in a single dose.5 Recommended treatment for tertiary syphilis (i.e., gummas and cardiovascular syphilis, but not neurosyphilis) is benzathine penicillin G 7.2 million U, administered in three divided doses of 2.4 million U IM each, at 1-week intervals.5 Ocular syphilis should be managed in collaboration with an ophthalmologist and according to the treatment and other recommendations for neurosyphilis, even if CSF findings are normal.
Conclusion
Although the prevalence of non-genital chlamydia and gonorrhea is highest in men who have sex with men, a large proportion of cases of either of these STIs in women would be overlooked with genital-only testing.3 HCPs should assess all sexually active patients for STI risk factors, including asking questions about both genital and non-genital sexual behaviors. When patients present with S/S of urogenital chlamydia or gonorrhea, HCPs should ask about possible infection exposure or infection symptoms at non-genital sites and conduct an appropriate physical exam. When sexually active individuals present with S/S of an eye infection, a sore throat, or skin lesions, HCPs should include an STI risk assessment. When risk, S/S, and/or physical exam findings indicate a possible non-genital STI presentation, additional testing should be considered. Furthermore, HCPs should discuss non-genital STI risks and S/S in patient education efforts regarding safer sex. Finally, HCPs should follow CDC guidelines regarding treatment for non-genital STIs.
Shelagh B. Larson is a woman’s health nurse practitioner. She serves on the NPWH Board of Directors (BOD) and the Texas Nurse Practitioners BOD. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
1. CDC. New CDC Analysis Shows Steep and Sustained Increases in STDs in Recent Years. August 28, 2018. cdc.gov/nchhstp/newsroom/2018/press-release-2018-std-prevention-conference.html
2. CDC. STDs at Record High, Indicating Urgent Need for Prevention. September 26, 2017. cdc.gov/media/releases/2017/p0926-std-prevention.html
3. Trebach JD, Chaulk CP, Page KR, et al. Neisseria gonorrhoeae and Chlamydia trachomatis among women reporting extragenital exposures. Sex Transm Dis. 2015;42(5):233-239.
4. Drinkard LN, Huxta RA, Halbritter A, et al. The case for extragenital screening of Chlamydia trachomatis and Neisseria gonorrhoeae in the college health setting. Sex Transm Dis. 2017;44(5):274-277.
5. CDC. 2015 Sexually Transmitted Diseases Treatment Guidelines. cdc.gov/std/tg2015/default.htm
6. Petrovay F, Németh I, Balázs A, Balla E. Chlamydial conjunctivitis: prevalence and serovar distribution of Chlamydia trachomatis in adults. J Med Microbiol. 2015;64(9):967-970.
7. CDC. Chlamydia – CDC Fact Sheet (Detailed). Page last updated September 26, 2017. cdc.gov/std/chlamydia/stdfact-chlamydia-detailed.htm
8. Sitpathy G, Behera HS, Ahmed NH. Chlamydial eye infections: current perspectives. Indian J Ophthalmol. 2017;65(2):97-102.
9. McAnena L, Knowles SJ, Curry A, Cassidy L. Prevalence of gonococcal conjunctivitis in adults and neonates. Eye. 2015;29(7):875-880.
10. CDC. Syphilis – CDC Fact Sheet. Page last updated June 13, 2017. cdc.gov/std/syphilis/stdfact-syphilis.htm
11. Barber LG, Gudgel DT. How Sexual Activity Can Affect Your Vision. 2018. aao.org/eye-health/tips-prevention/sex-stds-and-eye-health
12. CDC. STD Risk and Oral Sex – CDC Fact Sheet. Page last updated January 4, 2017. cdc.gov/std/healthcomm/stdfact-stdriskandoralsex.htm
13. de Paolo LF, Servato JP, Oliveira MT, et al. Oral manifestations of secondary syphilis. Int J Infect Dis. 2015;35:40-42.
14. Travis L, Glick S, Lowenstein E. Sexually transmitted diseases: recognizing telltale skin lesions disseminated gonococcal infection. Patient Care. 2005;1:45.
15. de Vries HJ. Skin as an indicator for sexually transmitted infections. Clin Dermatol. 2014;32(2):196-208.
16. CDC. Recommendations for the Laboratory-Based Detection of Chlamydia trachomatis and Neisseria gonorrhoeae— 2014. MMWR Recomm Rep. 2014;63(RR-02):1-19.
17. CDC. Gonococcal Infections in Adolescents and Adults. Page last updated January 4, 2018. cdc.gov/std/tg2015/gonorrhea.htm
18. CDC. Syphilis – CDC Fact Sheet (Detailed). Page last updated November 30, 2017. cdc.gov/std/syphilis/stdfact-syphilis-detailed.htm
19. Nakagawa H. Treatment of chlamydial conjunctivitis. Ophthalmologica. 1997;211:25-28.
20. World Health Organization. World Health Assembly Resolution WHA 51.11. Global Elimination of Blinding Trachoma. Geneva, Switzerland: WHO; 1998. who.int/blindness/causes/WHA51.11/en/
21. Haimovici R, Roussel TJ. Treatment of gonococcal conjunctiviti with single-dose intramuscular ceftriaxone. Am J Ophthalmol. 1989;107(5):511-514.
22. Chan PA, Robinette A, Montgomery M, et al. Extragenital infections caused by Chlamydia trachomatis and Neisseria gonorrhoeae: a review of the literature. Infect Dis Obstet Gynecol. 2016;2016:5758387.