
Thyroid disorders are fairly common in pregnancy, with the most common being hypothyroidism. Undiagnosed or inadequately treated hypothyroidism during pregnancy can have devastating consequences on the developing fetus. By contrast, early recognition and effective management of thyroid disorders in pregnancy can minimize risk for both maternal and neonatal complications.
Approximately 4% of women seeking prenatal care have previously been diagnosed with hypothyroidism.1 In iodine-sufficient areas such as the United States, the major cause of hypothyroidism in women of childbearing age is chronic autoimmune thyroiditis (Hashimoto’s disease).2 However, worldwide, iodine deficiency remains the most important cause of thyroid insufficiency.2,3 In addition, prior thyroidectomy; radioiodine therapy; use of medications such as amiodarone, anti-thyroid drugs, or lithium; and pituitary or hypothalamic disease can result in hypo-thyroidism.2
The prevalence of hypothyroidism diagnosed during pregnancy is 0.3%-0.5% for overt hypothyroidism and 2%-3% for subclinical hypothyroidism.2 Unrecognized or inadequately treated hypothyroidism during pregnancy has been associated with spontaneous abortion, preeclampsia, intrauterine fetal demise, preterm birth, low birth weight, postpartum hemorrhage, and irreversible detrimental effects on fetal neurodevelopment.2,4 The degree of neurocognitive deficit is related to the severity, duration, and gestational age at which hypothyroidism occurs.2,4,5
To reduce pregnancy complications and enhance optimal pregnancy outcomes, nurse practitioners (NPs) need to understand normal thyroid physiology, changes in thyroid physiology and laboratory values during pregnancy, fetal thyroid development and functioning, and strategies for effective pharmacologic management and thyroid monitoring for women with hypothyroidism during pregnancy. The purpose of this article is to increase this understanding.
Synthesis and regulation of thyroid hormones
The follicular cells are the functional cells of the thyroid gland. The follicular cells, in combination with iodine and the amino acid tyrosine, synthesize and secrete thyroid hormone (TH). TH synthesis is also controlled by serum iodide levels. The first step in TH synthesis is the concentration of iodide within the thyroid. Iodide is the inorganic form of iodine and the form in which iodine enters the thyroid. Iodide is oxidized to iodine by the enzyme thyroidal peroxidase (TPO) in the follicular cells.6
Thyroglobulin, a large glycoprotein synthesized by the follicular cells, is the precursor of TH. Thyroglobulin contains the amino acid tyrosine and is joined with one or two iodine molecules within the follicular cells. This joining, facilitated by TPO, results in the formation of iodotyrosine complexes.6 Two of these iodotyrosine complexes form the active THs: tri-iodothyronine (T3), which has three iodine molecules, and thyroxine (T4 ), which has four iodine molecules.
Thyroid hormone is stored in the thyroid as a colloid compound until needed. Of the TH that is synthesized, 90% is T4 , although T3 is physiologically more potent. Only a small amount of T3 is synthesized in the thyroid, with about 80% formed in the liver, kidneys, and muscles from de-iodination of T4 . T3 and T4 are transported in the circulation for the most part bound to thyroxine-binding globulin (TBG) and other plasma proteins such as albumin.6 Proteinbound TH acts as a reservoir, with free TH released as needed. Only free TH can enter target receptor cells, where it then influences a variety of metabolic processes in the body.
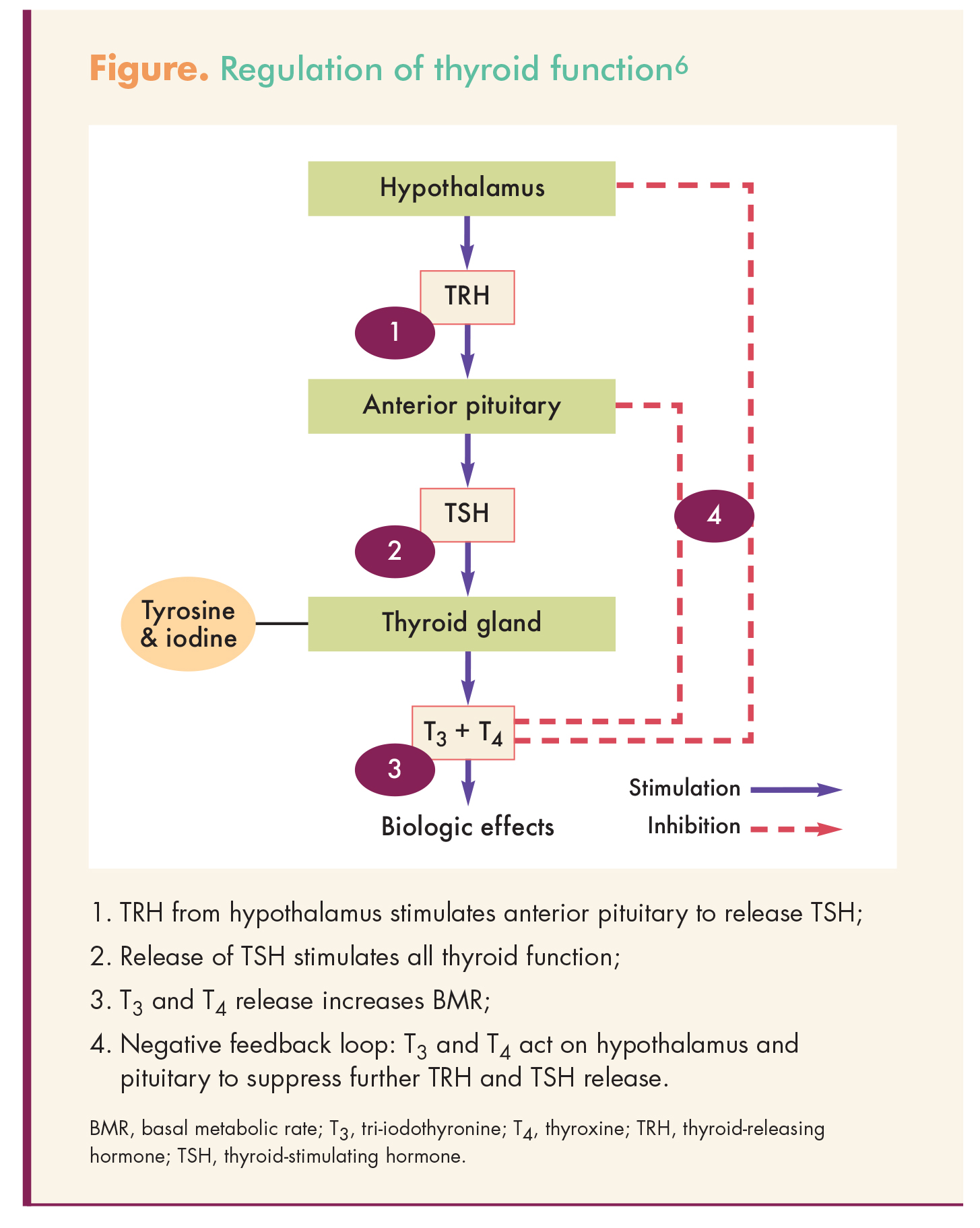
Thyroid hormone is regulated through a negative feedback loop involving the hypothalamus-pituitary- thyroid (HPT) axis. Thyrotropin-releasing hormone (TRH), synthesized in the hypothalamus, circulates via the hypothalamic-pituitary portal system to the anterior pituitary, where it stimulates release of thyroid-stimulating hormone (TSH).6 TRH is released in response to cold, stress, and decreased levels of free T4 (FT4 ). TSH, in turn, binds with receptors on the plasma membrane of the thyroid follicular cells and causes an immediate release and increase in synthesis of TH (Figure).6
{kind=link}
Thyroid changes during pregnancy
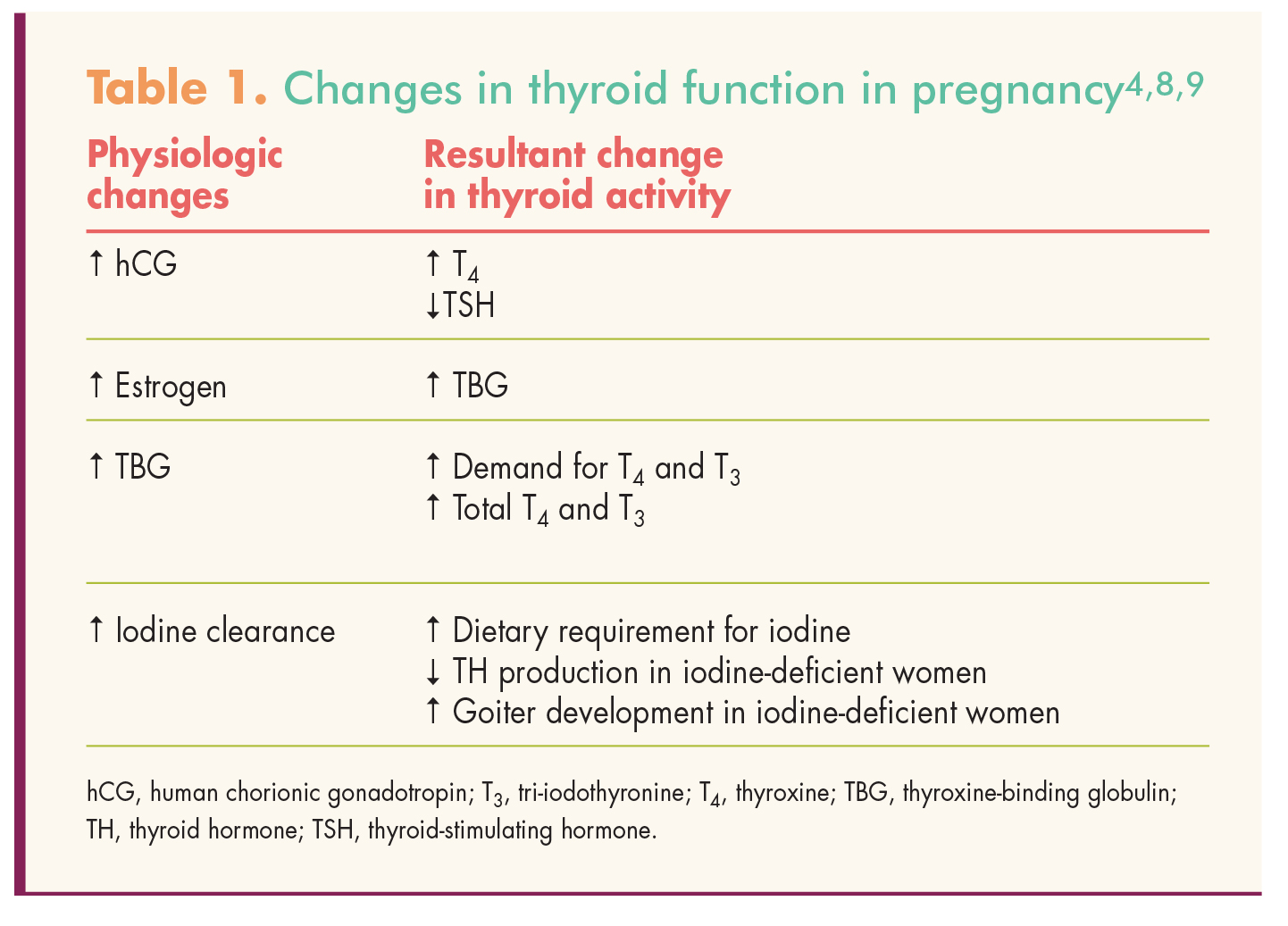
In response to increased metabolic needs during pregnancy, thyroid activity and hormone production increase. The thyroid typically enlarges moderately due to hyperplasia of glandular tissue and increased vascularity. Human chorionic gonadotropin (hCG) secreted by the placenta, similar in structure to TSH, directly stimulates the maternal thyroid to produce TH. TBG levels increase beginning at about 20 weeks’ gestation as a result of increased estrogen levels. These two changes—that is, hCG stimulation of TH synthesis and increased TBG levels—lead to a decrease in TSH levels in the first trimester, with a return to baseline in the second trimester, and an increase in total TH levels* throughout pregnancy. Table 1 shows the physiologic changes in thyroid function during pregnancy.4,8,9
{kind=link}
*Total TH includes both free and protein-bound forms; the increase in total TH is due mainly to the increased protein-bound forms of the hormone. The free circulating form of TH remains relatively unchanged throughout pregnancy.7,8
Nurse practitioners should note that non-pregnancy laboratory reference ranges do not apply to pregnant women. In fact, reference ranges change throughout pregnancy to reflect the physiologic changes occurring in thyroid function. Therefore, NPs should use trimester-specific, assay-specific normal ranges. If these ranges are unavailable, then these ranges for TSH should be used:3,4
• First trimester: 0.1-2.5 mIU/L
• Second trimester: 0.2-3.0 mIU/L
• Third trimester: 0.3-3.0 mIU/L
In addition, the elevated TBG seen in pregnancy interferes with immunoassays for FT4 levels. TSH is the most sensitive indicator of thyroid status in pregnant women.7
Fetal thyroid development and function
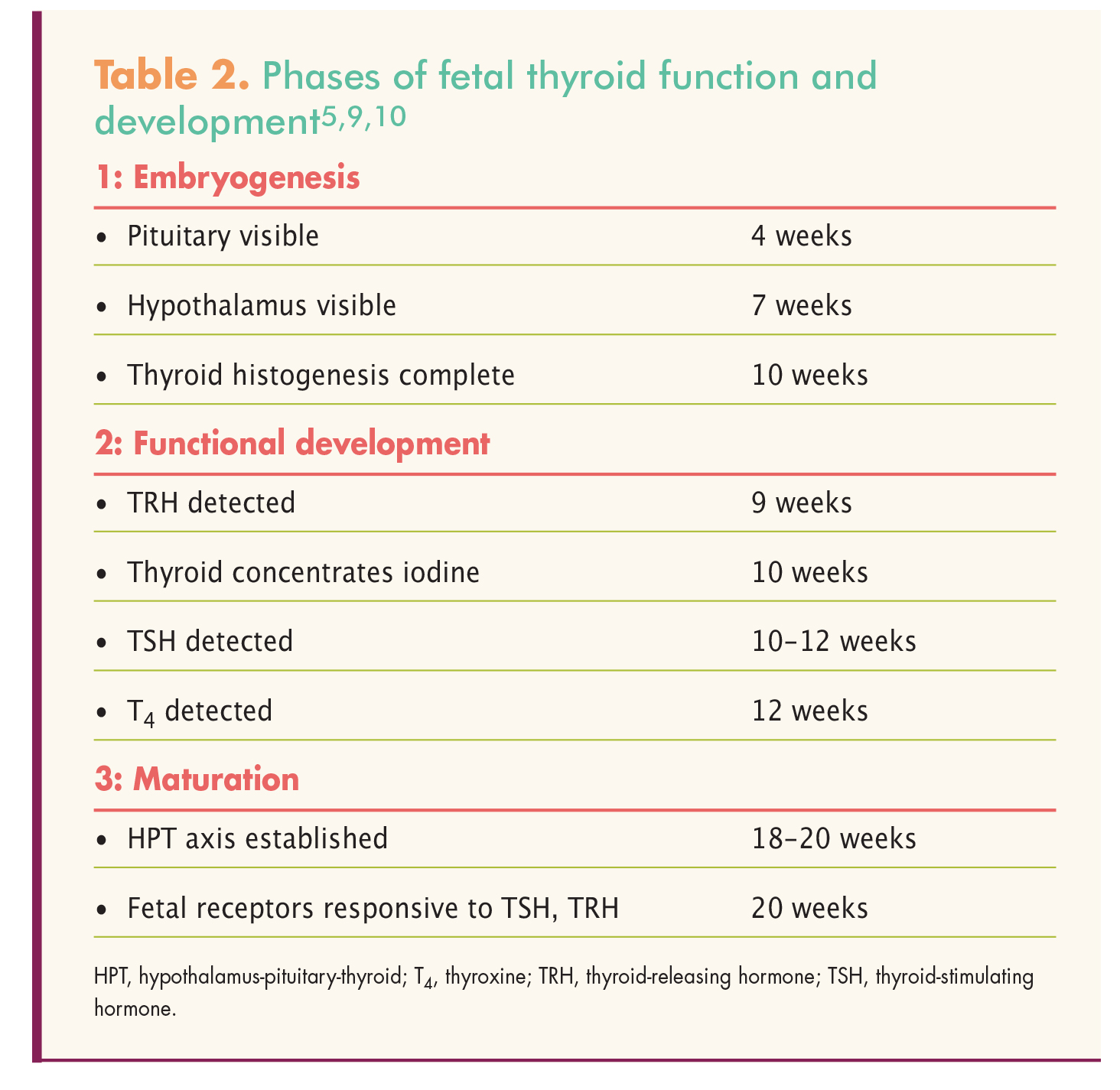
Fetal thyroid development and function can be divided into three overlapping phases: embryogenesis (phase I), functional development (phase II), and maturation (phase III) (Table 2).5,9,10 The thyroid is the first fetal endocrine gland to develop. It starts as a thickening at the base of the tongue and migrates down the neck to reach its final position in front of the trachea by 7 weeks’ gestation.9,10 Follicle cells form and begin thyroglobulin production by 8 weeks’ gestation. Although the fetal thyroid is able to start concentrating iodine and synthesizing iodothyronines by about 10 weeks’ gestation, little TH synthesis occurs until about 18 weeks’ gestation.9 During fetal development, T4 is the major TH being produced; T3 is not detected until the third trimester.9,10
{kind=link}
The fetal hypothalamus is visible by 7 weeks’ gestation, with levels of TRH detectable by 9 weeks.10 The fetal pituitary is visible by 4 weeks, with TSH starting to become detectable at 10-12 weeks.10 The fetal HPT axis begins to function mid-gestation (18-20 weeks), with the fetus beginning to implement feedback mechanisms for TH production.9,10 During this time, fetal receptors for TRH and TSH become responsive. Further maturation of the HPT axis continues throughout the remainder of pregnancy.10
Maternal hypothyroidism is particularly harmful to the fetal brain in the first half of pregnancy, when fetal T4 production is low. TH is critical for neuron development and neural pathway organization.5,9 It is the transplacental transfer of T4 and iodine in the first trimester that promotes fetal brain development until the fetal thyroid becomes functional.5 Even during the second and third trimesters, when the fetal thyroid is producing T4 , much of the T4 needed for development is still of maternal origin.5,9
Overt hypothyroidism
Overt hypothyroidism (OH) in pregnancy, evidenced by elevated TSH and low serum FT4, is linked to adverse fetal/obstetric outcomes. Stillbirth, preterm delivery, postpartum hemorrhage, and infants with neuropsychological and cognitive impairment have been reported in women with inadequately treated OH.2,4,5 OH should be treated with levothyroxine (LT4), with the goal of normalizing trimester-specific TSH values.4 Women who have been euthyroid on their LT4 dosages pre-pregnancy will need dosage changes throughout pregnancy in order to maintain the euthyroid state.
Subclinical hypothyroidism
Subclinical hypothyroidism (SH) is by far the most frequent thyroid dysfunction occurring during pregnancy.11 SH is associated with elevated TSH and normal FT4. SH represents early, mild thyroid dysfunction. Sixty percent to 80% of these cases demonstrate the presence of antithyroid peroxidase antibodies, a marker of chronic thyroiditis (Hashimoto’s disease).12 Because of limited and conflicting data, controversy exists regarding the effects of SH on fetal/obstetric outcomes, including the need to screen or treat women with SH. Several obstetric complications have been associated with SH, with pregnancy loss being one of the most frequent.11,12 Other reported complications include gestational hypertension, preeclampsia, low birth weight, placental abruption, and postpartum hemorrhage, albeit at lower frequencies than those recorded in pregnant women with untreated OH.11,12
Early studies reported impaired cognitive development in infants born to mothers whose SH was inadequately treated, but not in infants born to women with adequately treated SH.12,13 However, in 2012, a large randomized controlled trial, the Controlled Antenatal Thyroid Screening Study, revealed no difference in the neurocognitive development of infants born to women who were screened and treated for SH versus those whose SH status was not revealed until after delivery.14 As a result, the American Congress of Obstetricians and Gynecologists (ACOG), the Endocrine Society, and the American Thyroid Association (ATA) do not recommend universal screening for thyroid disease in pregnancy.4,7 Instead, screening is recommended only in women who are at increased risk for OH, those with symptoms of thyroid disease, and those with a personal history of thyroid disease.
However, a lack of consensus exists regarding the need to treat SH in pregnant women. ACOG recommends against treatment for pregnant woman with SH because of a lack of research showing benefit.7 However, the Endocrine Society and the ATA recommend LT4 therapy for all women with SH.4,7
Levothyroxine therapy
Levothyroxine, a Pregnancy Category A medication, remains the drug of choice for the treatment of all types of hypothyroidism. In typical cases, the LT4 dosage is increased as the pregnancy advances because of the hypermetabolic state that pregnancy induces.3,4 In fact, dosage requirements may increase by as much as 30%-50% during pregnancy, and these increases may be needed as early as the fifth week of gestation.3 Replacement therapy in dosages of 1-2 mcg/kg/day, or about 100 mcg/day, is recommended.12,137 NPs should check patients’ TSH levels every 4-6 weeks during pregnancy so that dosages can be adjusted as necessary. The goal is to maintain maternal serum TSH in the trimester-specific range.3,4 Because only minimal amounts of LT4 cross the placenta after the first trimester, the fetus is not at risk for thyrotoxicosis from maternal LT4 replacement.4,8
Because of differences, albeit subtle, in bioavailability among LT4 formulations, patients should stay with one formulation when possible. NPs should educate patients to take LT4 on an empty stomach—45 minutes before consumption of food, beverages, or other medications—for optimal absorption.3,15 Prenatal vitamins, calcium, and iron can interfere with the absorption of LT4 and should be avoided within 4 hours of taking LT4.3 Likewise, medications used to treat gastroesophageal reflux, including histamine-2 blockers, proton pump inhibitors, and antacids, can decrease LT4 absorption.15 Finally, NPs need to ascertain whether pregnant women are using any herbal products that contain lemon balm, also known as bee balm, honey plant, or sweet balm.16 Lemon balm, used as a tea or oil to treat anxiety, insomnia, and indigestion, is known to have anti-TSH effects, and can prevent T4 absorption from the small intestine.15,16
After delivery, the LT4 requirement drops immediately; women who were on LT4 prior to pregnancycan revert to their pre-pregnancy dosage.3,5 Women who were started on LT4 to treat OH during their pregnancy can likely reduce their dosage to half that taken just before delivery.3,4,7 If they were receiving LT4 to treat SH, the medication can be stopped and thyroid function tests performed in 6 weeks to determine whether further treatment is required.3,4,7 LT4 is considered safe to use during lactation.3,17
Iodine requirements and pregnancy
Iodine is a critical trace element required for TH synthesis; both maternal and fetal TH production depends on an adequate dietary intake of iodine.7 Iodine deficiency may be a factor contributing to concurrent maternal and fetal hypothyroidism. In the United States, iodized salt is an important source of iodine. (About 70% of salt sold for household use is iodized.) Other common dietary sources of iodine in the U.S. are dairy products, seafood, eggs, meat, and poultry.4 The prevalence of iodine deficiency is lowest in the Americas (10%) and highest in Europe (59.9%).3,8
In pregnancy, because of an increase in renal excretion of iodine and transfer of iodine to the placenta and fetus, the thyroid triples its uptake of iodine.8 Dietary iodine requirements are therefore increased during pregnancy. Although most U.S. women have adequate iodine intake to meet the increased demand for both maternal and fetal TH production, it is difficult to identify those who are at risk for or who may have mild to moderate iodine deficiency.4
In cases of mild to moderate iodine deficiency, the thyroid decreases synthesis of T4 in favor of T3 , the T3 levels remain normal, and circulating TSH does not rise. Thyroid function tests may indicate euthyroidism even though the amount of T4 available to the fetus may be insufficient.3 Severe iodine deficiency in pregnancy can cause hypothyroidism, poor pregnancy outcome, irreversiblemental retardation, and cretinism. Recent studies show that even mild iodine deficiency has been associated with impaired neurologic outcomes in children.3,8,9
The World Health Organization recommends an intake of 250 mcg/day of iodine during pregnancy and breastfeeding.4,18,19 To achieve this level, the ATA recommends that women in North America who are planning pregnancy or are pregnant or breastfeeding take a daily supplement containing 150 mcg of iodine.1,4 Among the roughly 200 prenatal vitamin brands marketed in the U.S., only half contain iodine, and among the products that do contain iodine, not all contain the recommended dose.4 In addition, studies have shown about 20% of pregnant woman do not take their prenatal vitamin supplement.1,4 NPs need to educate their pregnant patients about why they need to take all the supplements that are prescribed for them.
Conclusion
The normal physiologic changes in the thyroid during pregnancy occur to compensate for increased maternal metabolic demands and to provide adequate TH and iodine for fetal brain development. Hypothyroidism in pregnant women presents unique challenges related to these changes. The physiologic changes affect both interpretation of thyroid studies and dosing of LT4 during pregnancy. The goal of treatment is to restore euthyroidism as soon as possible and to maintain TSH in the trimester-specific reference range. NPs need to consider these key practice points:
• Thyroid disease is the second most common endocrine disorder of pregnancy (following diabetes).
• Iodine requirements increase in pregnancy and lactation. Women should be advised to take a prenatal vitamin that contains 150 mcg of iodine in its formulation.
• Under ideal circumstances, women with hypothyroidism should have their LT4 dose optimized prior to pregnancy and then reviewed each trimester.
• The dosage of LT4 needed to maintain a euthyroid state increases during pregnancy.
• Women with OH should be treated to maintain serum TSH in the trimester-specific goal range.
• Controversy exists regarding whether SH in pregnant women should be treated.
• T4 drops immediately following delivery; the LT4 dosage will need to be readjusted.
Carol A. Botwinski is Director/Chair of the Department of Nursing at the University of Tampa in Tampa, Florida. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
1. Haddow JE. The new American Thyroid Association Guidelines for thyroid disease during pregnancy and postpartum: a blueprint for improving prenatal care. Thyroid. 2011;21(10): 1047-1048.
2. Negro R, Mestman JH. Thyroid disease in pregnancy. Best Pract Res Clin Endocrinol Metab. 2011; 25(6):927-943.
3. Klubo-Gwiezdzinska J, Burman K, Van Nostrand D, Wartofsky L. Levothyroxine treatment in pregnancy: indications, efficacy, and therapeutic regimen. J Thyroid Res. 2011;1-12.
4. Stagnaro-Green A, Abalovich M, Alexander E, et al; American Thyroid Association Taskforce on Thyroid Disease during Pregnancy and Postpartum. Guidelines of the American Thyroid Association for the diagnosis and management of thyroid disease during pregnancy and postpartum. Thyroid. 2011;21(10):1081-1104.
5. Mann N. Congenital hypothyroidism – what’s new? Paediatr Child Health. 2011;21:295-300.
6. Matfin G. Disorders of endocrine control of growth and metabolism. In: Porth C, ed. Essentials of Pathophysiology. 4th ed. Philadelphia, PA: Wolters Kluwer; 2015:767-792.
7. American College of Obstetricians and Gynecologists. Practice bulletin No. 148: Thyroid disease in pregnancy. Obstet Gynecol. 2015; 125(4):996-1005.
8. Girling J, Sykes L. Thyroid disorders and other endocrinological disorders in pregnancy. Obstet Gynaecol Reprod Med. 2013;23:171-179.
9. Blackburn S. Maternal, Fetal, & Neonatal Physiology: A Clinical Perspective, 4th ed. St. Louis, MO: Saunders; 2012.
10. Rose S. Thyroid disorders. In: Martin R, Fanaroff A, Walsh M, eds. Neonatal-Perinatal Medicine: Diseases of the Fetus and Infant. 9th ed. St. Louis, MO: Elsevier; 2011:1556-1584.
11. McLeod D, McIntyre H. Subclinical hypothyroidism and related biochemical entities in pregnancy: implication and management. Obstet Med. 2010;3:139-144.
12. Cooper D, Biondi B. Subclinical thyroid disease. Lancet. 2012; 379(9821):1142-1154.
13. Behrooz HG, Tohidi M, Mehrabi Y, et al. Subclinical hypothyroidism in pregnancy: intellectual development of offspring. Thyroid. 2011;21(10): 1143-1147.
14. Lazarus JH, Bestwick JP, Channon S, et al. Antenatal thyroid screening and cognitive function. N Engl J Med. 2012:366(6):493-501.
15. Eligar P, Eligar V. Levothyroxine: factors affecting its intestinal absorption and metabolism. W London Med J. 2011;3:9-14.
16. University of Maryland Medical Center. Lemon Balm. Updated May 7, 2013.
17. National Institute of Health. Toxnet. Substance Name: Levothyroxine.
18. World Health Organization. Iodine Supplementation in Pregnant and Lactating Women. 2015.
19. World Health Organization. Joint statement by the WHO and UNICEF: Reaching optimal iodine nutrition in pregnant and lactating women and young children. 2007.