NPWH advocates for legislation, policies, and initiatives that promote access to care, establishment and implementation of evidence-based healthcare practices to improve maternal outcomes, and ongoing research into the contributing factors to maternal mortality and effective preventive strategies.
Reducing racial and ethnic disparities in maternal mortality must be a priority. The most recent data have shown that, compared with non-Hispanic white women, non-Hispanic black women had PRMRs that were 3.3 times higher and American Indian/Alaska Native women had PRMRs that were 2.5 times higher.1 NPWH supports action at all levels that address socioeconomic factors, barriers to access to quality healthcare, and implicit bias on the part of healthcare providers (HCPs), all of which contribute to disparities in healthcare services and health outcomes.
Women’s health nurse practitioners (WHNPs) who provide care for women before, during, and in between pregnancies are uniquely qualified to address the known contributing factors for preventable maternal mortality and to optimize health outcomes. WHNPs who specialize in high-risk antepartum and postpartum care are particularly well suited to enhance health outcomes for women with identified maternal morbidity and mortality risks.
Background
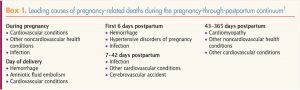
In the U.S., a pregnancy-related death is defined as one that occurs during pregnancy or within 12 months of the end of a pregnancy that is causally related to the pregnancy. This causality refers to deaths related to a pregnancy complication, a chain of events initiated by pregnancy, or the aggravation of an unrelated condition by the physiologic effects of pregnancy.1 A death is considered preventable if it is determined that a chance existed that the death could have been averted by one or more changes to community, health facility, patient, provider, and/or systems-level factors.2
Beyond gathering data on causes of maternal mortality, a concerted effort to understand contributing factors and the potential for prevention of maternal deaths is critical. State-level multidisciplinary maternal mortality review committees (MMRCs) are expanding across the nation, with the goal to identify and analyze maternal deaths using a standardized, systematic process. For each death, the committees make six key decisions: Was the death pregnancy related? What was the cause of death? Was the death preventable? What were the critical contributing factors to the death? What are the recommendations and actions that address the contributing factors? What is the anticipated impact of these actions, if implemented?3
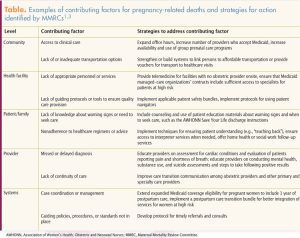
In a recent collaborative report, 13 state MMRCs identified 251 pregnancy-related deaths that occurred between 2013 and 2017.1 The committees were able to make a determination on preventability for 232 (92.4%) of the 251 deaths. Among these 232 deaths, 139 (60.0%) were determined to be preventable.1 The MMRCs categorized contributing factors for these preventable pregnancy-related deaths into five levels: community factors, health facility factors, patient factors, provider factors, and systems-level factors. Preventive strategies were identified for each level, with recognition that most deaths had more than one contributing factor and required more than one preventive strategy (Table).1,3
Translation of recommendations from MMRCs and other evidence-based sources into action, along with the study of outcomes, is
 crucial to eliminate preventable maternal deaths. The Alliance for Innovation on Maternal Health (AIM)—a national partnership of HCPs, public health professionals, and advocacy organizations under the auspices of the Council on Patient Safety in Women’s Health Care— provides resources for this purpose with the creation of safety bundles focused on high-risk maternal conditions.7,8 Safety bundles are evidence-based practices that, when consistently acted upon by the healthcare team, have been shown to improve patient outcomes.9 Each AIM safety bundle has four domains: readiness, recognition, response, and reporting/systems learning. AIM provides support and technical assistance at state and healthcare system levels to implement the bundles. Other resources for translating evidence into action include the American College of Obstetricians and Gynecologists, the California Maternal Quality Care Collaborative, the Center for Reproductive Rights and Black Mamas Matter Alliance, and the Society for Maternal-Fetal Medicine. A list of resources is provided in Box 2.10-26
crucial to eliminate preventable maternal deaths. The Alliance for Innovation on Maternal Health (AIM)—a national partnership of HCPs, public health professionals, and advocacy organizations under the auspices of the Council on Patient Safety in Women’s Health Care— provides resources for this purpose with the creation of safety bundles focused on high-risk maternal conditions.7,8 Safety bundles are evidence-based practices that, when consistently acted upon by the healthcare team, have been shown to improve patient outcomes.9 Each AIM safety bundle has four domains: readiness, recognition, response, and reporting/systems learning. AIM provides support and technical assistance at state and healthcare system levels to implement the bundles. Other resources for translating evidence into action include the American College of Obstetricians and Gynecologists, the California Maternal Quality Care Collaborative, the Center for Reproductive Rights and Black Mamas Matter Alliance, and the Society for Maternal-Fetal Medicine. A list of resources is provided in Box 2.10-26Legislation and policies are needed to facilitate action that promotes maternal health and reduces maternal morbidity and mortality. Federal and state legislation has expanded support for MMRCs, the work of the Council on Patient Safety in Women’s Health Care, and other maternal health initiatives. Federal-level bills have been introduced to extend Medicaid coverage eligibility to include 1 year of postpartum care. This coverage is particularly important because the 2011-2015 PMSS data indicated that 51.7% of pregnancy-related deaths occurred in the postpartum period, with 18.6% occurring 1-6 days postpartum, 21.4% occurring 7-42 days postpartum, and 11.7% occurring 43-365 days postpartum.1 Extended Medicaid coverage could change postpartum care to an ongoing process tailored to each woman’s own needs rather than a single encounter. The American College of Obstetricians and Gynecologists’ recommendations for a first postpartum visit at 3 weeks and a second visit no later than 12 weeks postpartum would be facilitated.18 A first visit earlier than the traditional 6 weeks, with follow-up at 12 weeks, would allow for better monitoring of risk factors and signs/symptoms of maternal complications, including mental health concerns. HCPs would have more opportunity to provide education, counseling, and any needed referrals, as well as a coordinated transition to well-woman care in the first year postpartum.
Preventive strategies that address community, health facility, patient, provider, and systems-level factors must give utmost priority to reducing the racial and ethnic disparities in pregnancy-related mortality that have persisted over time. Although the overall PRMR in the U.S. in 2011-2015 was 17.2 deaths per 100,000 live births, racial/ ethnic comparisons revealed significant differences. Non-Hispanic black women and American Indian/Alaska Native women had PRMRs of 42.8 and 32.5 deaths per 100,000 live births, respectively, as compared with 13.0 deaths per 100,000 live births for non-Hispanic white women.1 Causes of these disparities in maternal mortality are not fully understood and are likely multifactorial. Data have indicated that racial and ethnic minority women, compared with non-Hispanic white women, are less likely to (1) receive early and regular prenatal care, (2) have access to maternal-fetal medicine specialists, (3) give birth in higher-quality hospitals, and (4) attend a postpartum visit.27,28 Compared with non-Hispanic white women, non-Hispanic black women are more likely to have health conditions that place them at risk for maternal morbidity and mortality and they have twice the rate of unplanned pregnancies.28
Substantial evidence indicates that implicit racial/ethnic bias exists among HCPs—as it does in the general population—and that this bias can affect patient–HCP interactions, treatment decisions, treatment adherence, and patient outcomes.29,30 (Implicit biases are unconscious attitudes that can influence affect, behavior, and cognitive processes.) More research is needed to fully understand how implicit bias affects patient care and outcomes and whether certain intervention strategies can help address this bias within healthcare.
Implications for women’s healthcare and WHNP practice
 WHNPs provide healthcare for women before, during, and in between pregnancies in a variety of settings. The care they provide before and in between pregnancies places them at the forefront to assess for and address known risk factors for maternal complications prior to pregnancy. Box 3 highlights risk factors that can be identified prior to a pregnancy and mitigated by care tailored to each woman’s needs. WHNPs provide essential routine and high-risk pregnancy and postpartum care that includes identification of factors that may place a woman at an increased risk for maternal complications, implementation of care to mitigate risks, and collaboration within the healthcare team when complications occur to foster the best patient outcomes.
WHNPs provide healthcare for women before, during, and in between pregnancies in a variety of settings. The care they provide before and in between pregnancies places them at the forefront to assess for and address known risk factors for maternal complications prior to pregnancy. Box 3 highlights risk factors that can be identified prior to a pregnancy and mitigated by care tailored to each woman’s needs. WHNPs provide essential routine and high-risk pregnancy and postpartum care that includes identification of factors that may place a woman at an increased risk for maternal complications, implementation of care to mitigate risks, and collaboration within the healthcare team when complications occur to foster the best patient outcomes.
With the recognition that up to one-half of pregnancy-related deaths occur in the first year postpartum, the role of WHNPs in the transition from postpartum to well-woman care is crucial to continue to monitor risks and provide appropriate care, including attention to mental health. A concerted effort at community, health facility, patient, provider, and systems levels is critical to make progress in the goal to eliminate preventable pregnancy-related deaths.
Recommendations
NPWH recommends that WHNPs who provide healthcare for women before, during, and in between pregnancies should:
• be aware of their state’s status regarding existence of or plans for an MMRC and monitor data reports.
• seek active involvement in planning and implementing evidence-based maternal mortality preventive strategies at community, provider, patient, health facility, and systems levels to address MMRC-identified causes and contributing factors.
• engage in self-reflection regarding potential for implicit bias and seek educational activities that increase awareness and enhance patient–provider interactions.
• participate in research to more fully understand contributing factors to preventable maternal mortality.
• participate in maternal health quality improvement projects that facilitate translation of evidence to practice with outcomes evaluation
• advocate for local, state, and federal policies and legislation that address known contributing factors, including racial/ethnic disparities related to maternal mortality.
• continuing education(CE)programs and other evidence-based resources are available for NPs to learn and update knowledge regarding causes, contributing factors, and strategies to eliminate preventable maternal mortality.
• CE programs and other evidence-based resources on strategies for NPs to recognize and address racial/ethnic biases in themselves and at their healthcare facilities are available.
• collaborative engagement with other professional organizations continues to advance the development, implementation, and evaluation of multidisciplinary best practices that will eliminate the preventable maternal mortality.
• polices at all levels support access to quality care for women throughout the reproductive-age continuum.
• research moves forward in all aspects of prevention of maternal mortality.
References
1. Petersen EE, Davis NL, Goodman D, et al. Vital signs: pregnancy-related deaths, United States, 2011-2015, and strategies for prevention, 13 States, 2013-2017. MMWR. 2019;68(18):423-429. cdc.gov/mmwr/volumes/68/wr/mm6818e1.htm
2. Metz TD. Eliminating preventable maternal deaths in the United States: progress made and next steps. Obstet Gynecol. 2018;132(4):1040-1045.
3. Building U.S. Capacity to Review and Prevent Maternal Deaths. Report from nine maternal mortality review committees. 2018. reviewtoaction.org/Report_from_Nine_MMRCs
4. Metz TD, Rovner P, Hoffman MC, et al. Maternal deaths from suicide and overdose in Colorado, 2004-2012. Obstet Gynecol. 2016;128(6):1233-1240.
5. Smid MC, Stone NM, Baksh LP, et al. Pregnancy-associated death in Utah: contribution of drug-induced deaths. Obstet Gynecol. 2019;133(6):1131-1140.
6. 115th Congress. H.R. 1318 – Preventing Maternal Deaths Act of 2018. congress.gov/bill/115th-congress/house-bill/1318.
7. Mahoney J. The Alliance of Innovation in Maternal Health Care: a way forward. Clin Obstet Gynecol. 2018;61(2):400-410.
8. Council on Patient Safety in Women’s Health Care website. 2019. safehealthcareforeverywoman.org/
9. Resar R, Griffin FA, Haraden C, et al. Using Care Bundles to Improve Health Care Quality. IHI Innovation Series White Paper. Cambridge, MA: Institute for Healthcare Improvement; 2012.
10. Council on Patient Safety in Women’s Health Care. Patient Safety Bundles. 2019. safehealthcareforeverywoman.org/patient-safety-bundles/
11. California Maternal Quality Care Collaborative. Maternal Quality Improvement Toolkits. cmqcc.org/resources-tool-kits/toolkits
12. ACOG. Postpartum Toolkit. Racial Disparities in Maternal Mortality in the United States: The Postpartum Period Is a Missed Opportunity for Action. 2018. http://acog.org/-/media/Departments/Toolkits-for-Health-Care-Providers/Postpartum-Toolkit/ppt-racial.pdf?dmc=1&ts=20190613T1434044080
13. Black Mamas Matter Alliance. Advancing the Human Right to Safe and Respectful Maternal Health Care. Center for Reproductive Rights. 2018. blackmamasmatter.org/wp-content/uploads/2018/05/USPA_BMMA_Toolkit_Booklet-Final-Update_Web-Pages-1.pdf
14. ACOG. Practice Bulletin No. 212: Pregnancy and Heart Disease. Obstet Gynecol. 2019;133(5):e320-e356.
15. ACOG. Practice Bulletin No. 203: Chronic Hypertension in Pregnancy. Obstet Gynecol. 2019;133(1):e26-e50.
16. ACOG Practice Bulletin No. 202: Gestational Hypertension and Preeclampsia. Obstet Gynecol. 2019;133(1):e1-e25.
17. ACOG. Committee Opinion No. 762: Prepregnancy Counseling. Obstet Gynecol. 2019;133(1):e78-e89.
18. ACOG. Committee Opinion No. 736: Optimizing Postpartum Care. Obstet Gynecol. 2018;131(5):e140-e150.
A. reviewtoaction.org/content/mmr-map
B. safehealthcareforeverywoman.org/patient-safety-bundles/C.cmqcc.org/resourcestool-kits/toolkits
D. acog.org/-/media/Departments/Toolkits-for-Health-Care-Providers/Postpartum-Toolkit/ppt-racial.pdf?dmc=1&ts=20190613T1434044080
E. blackmamasmatter.org/wp-content/uploads/2018/05/USPA_BMMA_Toolkit_Booklet-Final-Update_Web-Pages-1.pdf
F. s3.amazonaws.com/cdn.smfm.org/publications/267/down-load-80817ee958474b8c4cc857fab01e53de.pdf
G. ajog.org/article/S0002-9378(19)30246-7/fulltext