
In June 2015, the FDA updated its recommendations for the labeling of drugs with respect to their use by pregnant women, lactating women, and females and males of reproductive potential. Healthcare providers caring for these populations, many of whom are taking prescription medications and biologics, need to be alert to these labeling changes.
{kind=link}
Between 64% and 94% of pregnant women use a prescribed medication during their gestation.1,2 Among pregnant women who take prescribed medications, 80% do so during the first trimester,3 when fetal organ systems and structures are being formed. For many women who are managing chronic diseases, discontinuing the medications is not an option. In addition, because more than 50% of pregnancies in the United States are unintended,4 a large group of women are exposing their fetus to medications before they even realize that they are pregnant.
For postpartum patients on medications for chronic conditions, the choice to breastfeed their infant may pose a dilemma. Many of these women are advised to bottle-feed their infants instead, even if they are using medications safely taken by lactating women.5 Likewise, women who become ill during the lactation period may be counseled to stop breastfeeding their child if they need to take certain medications. According to the Centers for Disease Control and Prevention, 77% of infants born in the United States in 2010 were breastfed.6 During the same year, breastfeeding rates were 49% at 6 months and 27% at 1 year. Because many breastfeeding mothers are using prescription medications, these statistics translate to hundreds of thousands of infants potentially being exposed to these same medications for prolonged periods of time.
For reproductive-aged women who could become pregnant, counseling with regard to the potential impact of prescription or over-the-counter medications on pregnancy is often lacking. In the case of drugs that are known teratogens, past research indicates that women who had them prescribed, compared with women for whom safer medications were prescribed, did not receive contraceptive counseling in greater numbers.7 The impact of certain drugs on fertility, including chemotherapeutic medications, may not be discussed unless the effects are catastrophic. Finally, there is scant information on the need for reproductive health counseling for men in terms of medication use. Available counseling has often focused on the impact of illicit drugs on male factor infertility.8
Role of the FDA
The thalidomide tragedy, as it developed in the late 1950s and early 1960s in Europe, provided the impetus for tighter regulation of drugs by the FDA in the United States. In 1979, the FDA adopted a labeling system that rated drugs for pregnant women using the well-known letter system: A, B, C, D, or X. At the time, the FDA did not provide a risk classification system for drugs taken during lactation. Pregnant women and nursing mothers were considered under the precaution areas of the counseling for medication use.9
Early in 1996, the FDA determined that the letter system was too simplistic.3 In addition, many drugs were allocated to different risk categories, depending on how the results of safety studies were being interpreted,10 resulting in confusion for healthcare providers (HCPs) and patients alike. The Teratology Society asked the FDA to develop a more comprehensive risk counseling strategy that would encompass all stages of the childbearing process.1 Changes to the system were proposed in 2008, and multiple public hearings and comment periods ensued. The Pregnancy and Lactation Labeling Rule (PLLR) was adopted and published in December 2014. Immediate compliance with the labeling rule has been required for all prescription drug and biologic products submitted to the FDA after June 30, 2015; phased-in compliance over 3-5 years is required for previously approved prescription drugs and biologics.11
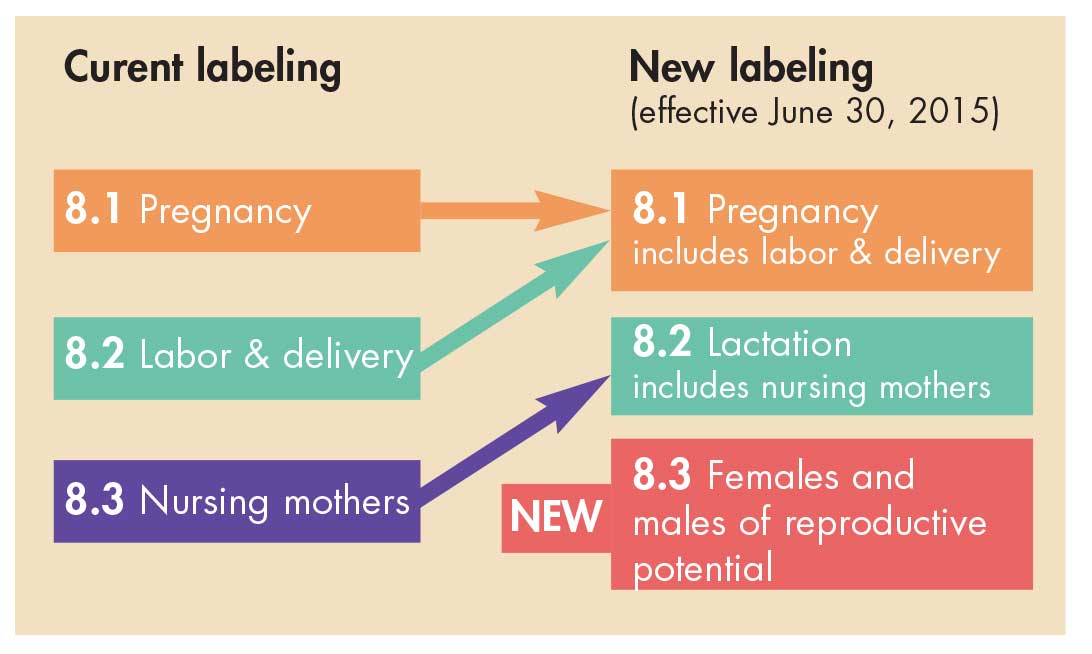
The 2015 Pregnancy and Lactation Labeling Rule.12
The PLLR requires changes to the content and format for information presented in prescription drug labeling in the Physician Labeling Rule format to assist HCPs in assessing benefit versus risk and in subsequent counseling of pregnant women and nursing mothers who need to take medication, thereby enabling them to make informed decisions for themselves and their children. Subsections for pregnancy, lactation, and females and males of reproductive potential are required in the Use in Specific Populations section. Pregnancy letter categories have been removed.
Pregnancy subsection
Specific subheadings required in the pregnancy subsection include contact information for a pregnancy exposure registry for the drug (if one is available), a risk summary, clinical considerations, and available human and animal data. Some subheadings may be excluded if no relevant information is available.
Risk summary
This subheading is always required. If a drug is contraindicated in pregnancy, this fact must be listed first. Statements that describe risks for adverse developmental outcomes based on relevant human data, animal data, and the drug’s pharmacology are required. A cross-reference to additional details in the data subheading is included when applicable. Drugs not absorbed systemically following a particular route of administration include a statement that maternal use is not expected to result in fetal exposure to the drug. Drugs with more than one route of administration must include information related to each route.
Clinical considerations
This subheading provides information to further assist HCPs in prescribing decisions and risk–benefit counseling. When relevant, this subheading includes information about disease-associated maternal and/or embryo/fetal risk, dose adjustments during pregnancy and postpartum, maternal adverse reactions, fetal/neonatal adverse reactions, and labor/delivery. Inclusion of any disease -associated maternal and/or embryo/fetal risks is important for patient counseling and informed decision making. After all, HCPs and patients need to weigh the risks and benefits of not treating a disease/condition in pregnancy (e.g., depression, hyperlipidemia) versus the risks and benefits of taking a given drug during pregnancy.
When pharmacokinetic data support dose adjustment during pregnancy and/or postpartum, a summary of this information is provided. When applicable, cross-referencing to other labeling sections (e.g., Clinical Pharmacology, Dosage and Administration) for additional information is included.
Drug-associated adverse reactions that are unique to pregnancy or that occur with increased frequency or severity in pregnant women are described. When available, information on any clinical interventions to monitor or reduce maternal drug-associated adverse reactions is provided.
The fetal/neonatal adverse reactions described in this subsection are those based on the drug’s pharmacologic activity. The potential severity and reversibility of the adverse reaction, as well as interventions for monitoring and mitigation of the adverse reaction, are included.
If a drug is expected to affect labor or delivery, the labeling must provide available information about the drug’s effects on the mother, the fetus/neonate, and the duration of labor and delivery. An example is the use of an opioid during labor that may cause respiratory depression in the neonate. The labeling information includes the effect of dose, timing, and duration of exposure on the risk to the neonate and the use of naloxone to mitigate the reaction.
Data
Data that provide the scientific basis for the information in the risk summary and clinical consideration subheadings are included. Human and animal data are presented separately. Data regarding adverse developmental outcomes, adverse reactions, and other adverse events related to the drug must be included.
Lactation subsection
This subsection must include a risk summary, applicable clinical considerations, and any available human and animal data. The term lactation refers to the biologic state during which the body produces and excretes milk. The term breastfeeding is used to refer to all human milk, whether received directly from the breast or as expressed milk.
Risk summary
This subheading is always required. If a drug is contraindicated during breastfeeding (e.g., radioisotopes), this fact must be stated first. Drugs not absorbed systemically by the mother following a particular route of administration must include a statement that maternal use is not expected to result in the child’s exposure to the drug during breastfeeding. Drugs with more than one route of administration must include information related to each route. For drugs absorbed systemically, available information on whether the drug and/or its active metabolites are present in human milk, effects of the drug on the breastfed child, and effects of the drug on milk production and/or excretion must be included. If a drug and/or its active metabolites are present in human milk, detailed information on actual or estimated infant daily dose based on exclusive breastfeeding must be provided. The risk summary must acknowledge when data are lacking.
Clinical considerations
A description of ways to minimize exposure of the breastfed child to systemically absorbed drugs that are used intermittently, in a single dose, or short term must be included. This description may include information on timing of administration of the drug relative to feeding, pumping sessions, or expressing for discarding. Specified time periods are based on the half-life of the drug and/or its active metabolite(s). Information on monitoring for adverse reactions must be included if available.
Data
As with the pregnancy subheading, data on which the risk summary and clinical considerations are based for lactation and breastfeeding are provided.
Females and males of reproductive potential subsection
This subsection is included if there are human or animal study data of potential drug-associated effects on fertility and/or pre-implantation loss. Recommendations for pregnancy testing and/or contraception may be based on concerns for adverse developmental outcomes if the drug is taken during pregnancy.
Relevance to practice
Healthcare providers can use the information provided in the new labeling to be better informed and enhance discussions about the benefits and risks of specific drugs with women who are pregnant or lactating or with patients of reproductive potential. The information contained in the PLLR may or may not be the same as that included in patient drug information.
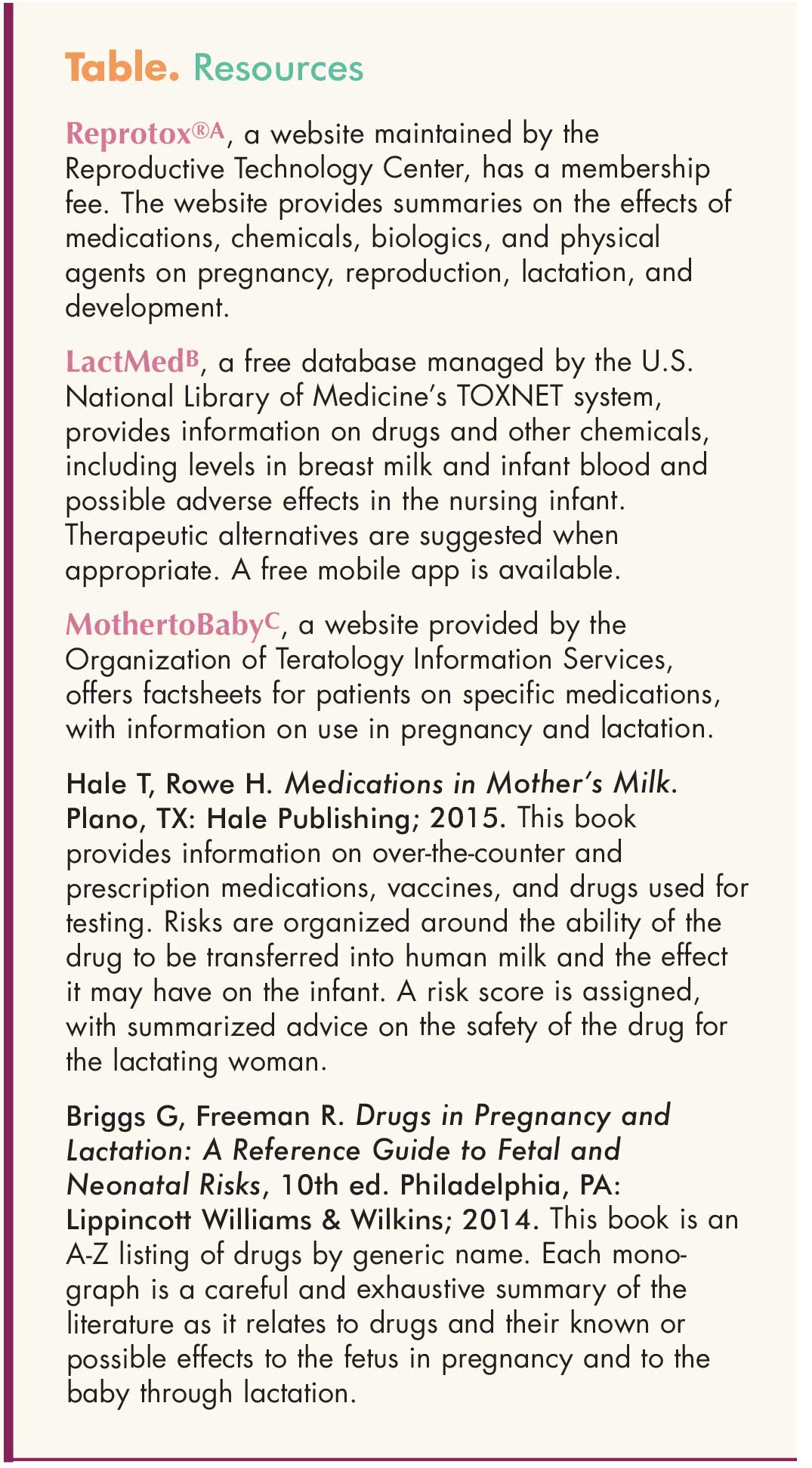
Providers can utilize websites, mobile apps, and reference texts to focus counseling or answer patients’ questions (Table). These resources may be especially useful until the PLLR changes are fully implemented, as well as for supplemental information. As always, HCPs can consult with pharmacists regarding the pharmacokinetics and pharmacodynamics of a drug.
{kind=link}
Kathleen M. Mahoney is a perinatal clinical nurse specialist at Robert Wood Johnson University Hospital in New Brunswick, New Jersey. The author states that she does not have a financial interest in or other relationship with any commercial product named in this article.
References
1. Ramoz LL, Patel-Shori NM. Recent changes in pregnancy and lactation labeling: retirement of risk categories. Pharmacotherapy. 2014;34(4):389-395.
2. Fantasia H, Harris A. Changes to pregnancy and lactation risk labeling for prescription drugs. Nurs Womens Health. 2015;19(3):266-270.
3. Mazur-Amirshahi M, Samiee-Zafarghandy S, Gray G, Van den Anker JN. Trends in pregnancy labeling and data quality for US-approved pharmaceuticals. Am J Obstet Gynecol. 2014;211(6):690e1-11.
4. Guttmacher Institute. Unintended Pregnancy in the United States. March 2016.
5. Saha MR, Ryan K, Amir LH. Postpartum women’s use of medicines and breastfeeding practices: a systemic review. Int Breastfeed J. 2015;10(28):1-10.
6. Centers for Disease Control and Prevention. Breastfeeding Report Card, 2013.
7. Schwartz EB, Postlethwaite DA, Hung YY, Armstrong MA. Documentation of contraception and pregnancy when prescribing potentially teratogenic medications for reproductive age women. Ann Intern Med. 2007;147(6): 370-376.
8. Fronczak CM, Kim ED, Barqawi AB. The insults of illicit drug use on male fertility. J Androl. 2012;33(4):515- 528.
9. Mosley JF 2nd, Smith LL, Dezan MD. An overview of upcoming changes in pregnancy and lactation labeling information. Pharm Pract (Granada). 2015;13(2):605.
10. Addis A, Sharabi S, Bonati M. Risk classification systems for drug use during pregnancy: are they a reliable source of information? Drug Saf. 2000;23(3):245-253.
11. Food and Drug Administration. Pregnancy and Lactation Labeling (Drugs) Final Rule. December 3, 2014.
12. Food and Drug Administration. Pregnancy, Lactation, and Reproductive Potential: Labeling for Human Prescription Drug and Biological Products — Content and Format. Washington, DC: Food and Drug Administration; 2015.
Web resources
A. reprotox.org