
An abundance of data and literature indicates that social determinants of health (SDOH) impact individuals and population health.1–3 It is estimated that 30% to 55% of total health outcomes are due to SDOH.4 Data indicate that over half of the deaths in the United States are due to social and behavioral causes.2
Of note, SDOH disproportionately affects those who identify as women. Gender-based health disparities are defined as a social phenomenon in which men and women are not treated equally. The difference in treatment may arise from distinctions about biology, psychology, or cultural norms. People who identify as women face greater barriers to accessing care, including discriminatory attitudes, lower literacy rates, and a lack of both healthcare providers and systems built for the unique needs of women’s health.4,5 From the healthcare provider side, data show a large gap in assessment and lack of understanding in the domain of SDOH.6–8
Advanced practice registered nurses (APRNs) function on the frontline of healthcare and are in a unique position to address SDOH. The American Association of Colleges of Nursing (AACN) promotes the importance of reducing health inequity in the 21st century by mandating SDOH education as a critical part of nursing practice.9 Through increasing the integration of SDOH into nursing curricula and clinical experiences, students will be better prepared to positively impact health equity as future healthcare providers.10 Recognizing lack of understanding and confidence in addressing SDOH along with faculty recommendation, the women’s health (and gender-related) nurse practitioner (WHNP)-specific SDOH clinical toolkit was created. Clinical practice toolkits can allow for greater efficiency in assessment and access to SDOH resources.11
Purpose
The purpose of this quality improvement (QI) project was to support the assessment and addressing of SDOH in the women’s and gender-related healthcare setting. This project aimed to address SDOH concerns specific to women and gender-related health by integrating an SDOH workshop and a clinical toolkit to increase understanding of SDOH concerns in the clinic setting, increase confidence in assessing social determinants, and increase confidence in addressing resources in a women’s health clinic setting.
Setting and population
This project took place at the University of Minnesota (UMN)–Twin Cities using a sample of the DNP cohort APRN students. Implementation of the project occurred during the Covid-19 pandemic, which led to the creation of a virtual toolkit and surveying participants using web-based surveys rather than in-person paper tools. The toolkit was then taken to various sites in the metro area and utilized during their clinical rotations.
Intervention
The project involved implementing an evidence-based toolkit to complement an experiential SDOH workshop created by Dr. Diana Drake and Dr. Barb Peterson. The workshop is a part of the WHNP-DNP curriculum designed to better prepare APRN students to assess SDOH in patient care. The evidence-based toolkit was given to students to utilize in their clinical practicum. The workshop and toolkit worked synergistically to enhance SDOH education in the nursing curriculum. The choice of components and design of the toolkit were guided by responses to a baseline survey from students in their second year in the WHNP program. The survey asked questions about student confidence in assessing and addressing SDOH in the clinic setting. Data from that baseline assessment helped identify gaps in understanding and confidence in addressing SDOH. The toolkit consists of two main categories: the primary section, which suggests language for the APRN student to utilize when opening and closing SDOH assessments; and the second section, which contains links for resources organized by category (Figure).
Figure. Image of SDOH toolkit
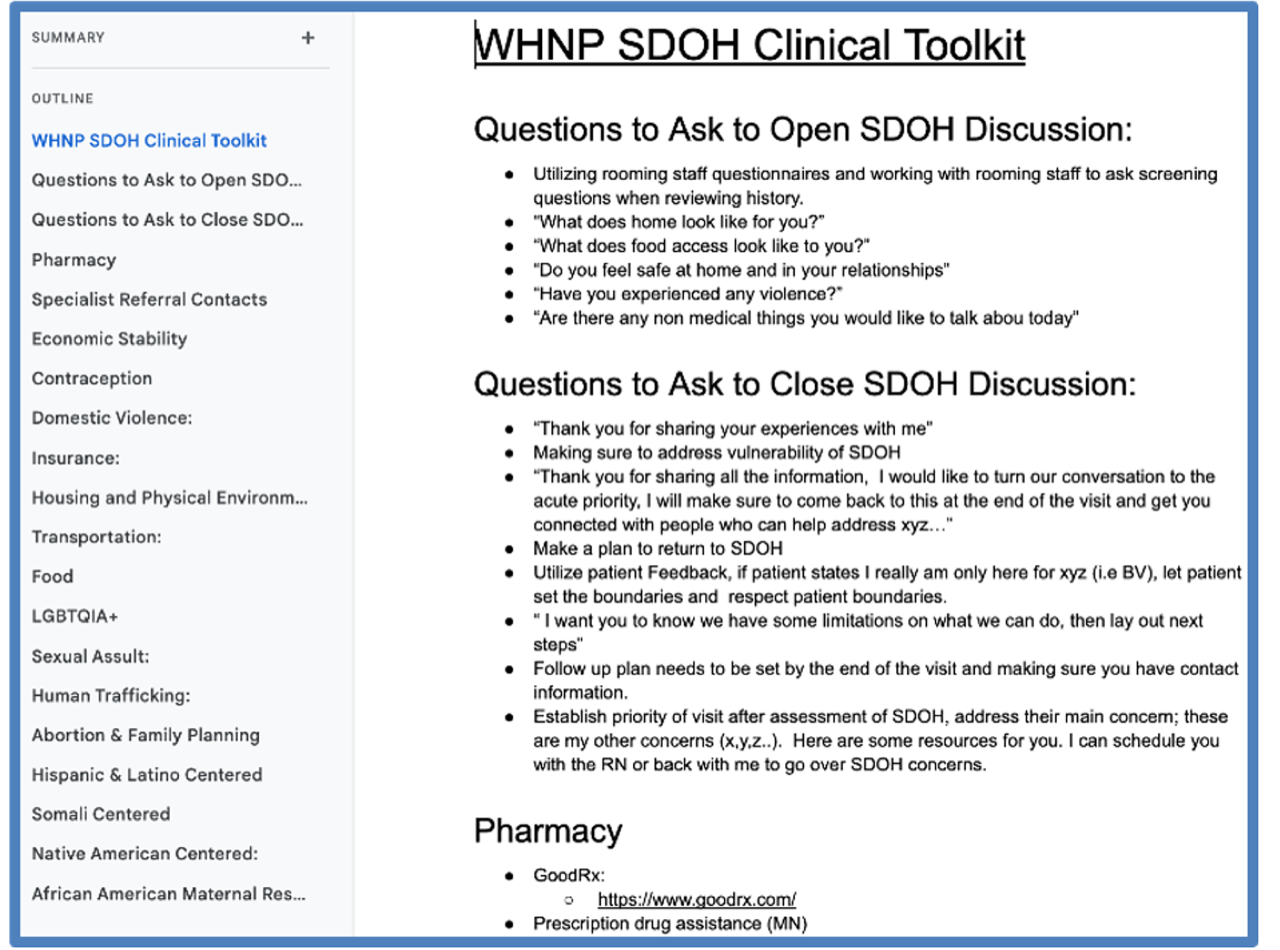
The resource list within the toolkit was created by determining the top 10 SDOH concerns related to women’s and gender-related health in the Twin Cities as identified by clinical experts and WHNP faculty. The categories of concern included: economic stability, domestic violence, contraception, insurance, food, transportation, LGBTQIA+, sexual assault, human trafficking, abortion and family planning, specialties referral contacts, African American maternal health, Hispanic and Latino-centered, Somali-centered, Native American-centered, and Pharmacy. Within each category, at least three community-based referrals were identified and provided as resources. All resources were located in the Twin Cities metro area. Resource identification was done through clinical site recommendations, social work recommendations, faculty recommendations, and web searches, and were verified by the project leader and project advisors. Each resource has a brief description of its primary usage and contact information including phone, email, or webpage with a hyperlink to allow for quick access and immediate referral.
Evaluation methods
This QI project was reviewed for human subjects’ protection using the online Institutional Review Board (IRB) determination tool developed by the University of Minnesota IRB. The responses indicated this was a quality assurance/QI project and did not meet the federal definition of Human Subjects Research. No additional IRB was required for this QI project.
In total, this project used three surveys to assess baseline data and impact of the intervention. All three surveys were anonymous and confidential. Each survey had a question at the beginning to evaluate informed consent and has a description section of what the study was and how the data would be compiled. The primary survey was sent to students in September 2022 prior to participation in the workshop to determine a baseline of where students ranked their confidence in assessing and addressing SDOH in the clinical setting. This baseline survey aided in the design of the toolkit and allowed for the comparison of students’ baseline knowledge with post-intervention data.
The second survey was administered after the SDOH workshop to identify trends in student confidence and knowledge when assessing and addressing SDOH post workshop. The final survey was sent to students after 120 hours of direct clinical experience with the toolkit to determine students’ knowledge and application of SDOH interventions. Surveys contained quantitative and qualitative items. A 5-point Likert scale was used for quantitative items alongside free response for qualitative items.
Results
In total, 10 students completed all three surveys (N = 10). Data were deidentified and then analyzed using Microsoft Excel. Data were then split into qualitative and quantitative sections.
The quantitative data were analyzed on a 1 to 5 Likert scale with 1 indicating strongly disagree and 5 indicating strongly agree and averaged among the 10 participants. Increased Likert scores were reported across the board. Three questions were chosen for full analysis (Table). The first question analyzed was “I am confident when assessing and addressing SDOH in the clinical setting.” Data revealed a baseline score of 2.9 and a post-workshop and toolkit score of 4.5, showing a 55% increase in confidence when assessing and addressing SDOH.
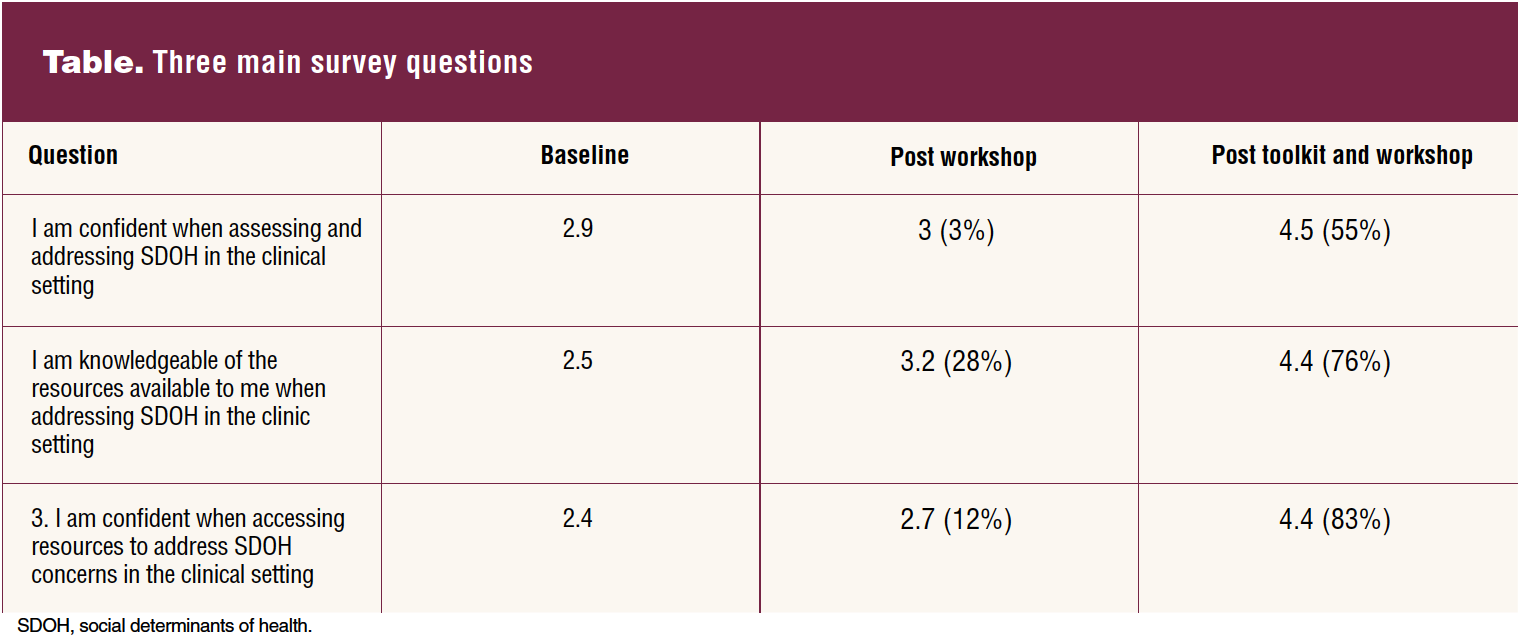
The second quantitative question was, “I am knowledgeable of the resources available to me when addressing SDOH in the clinic setting.” Baseline Likert scores were averaged at 2.5, increasing by 76% to a score of 4.4.
The final question was “I am confident when accessing resources to address SDOH concerns in the clinical setting.” Students’ baseline score averaged 2.4, and there was an 83% increase reported to a post-workshop and toolkit score of 4.4.
For the qualitative section of the data, students reported that the resources included in the toolkit were applicable to their sites and that if one resource did not work for their patient, they could refer to other categories for other options. Students reported the format of the toolkit was convenient but could be improved if integrated into the electronic health record (EHR) or an application on their mobile phones (Figure).
Discussion
Researchers showed that there is an overall gap in knowledge and resources when addressing SDOH in the clinic setting that leads to worse health outcomes.7 This project aimed to increase the understanding of SDOH in the clinic setting for WHNP students. The goal was to increase confidence when assessing and addressing SDOH by 20%.
We found a 55% increase overall in confidence when assessing and addressing SDOH in the clinic setting after the workshop and the use of the clinical toolkit. We also saw a 76% increase from baseline in the knowledge of resources and 83% increase in confidence when using resources. These results support a potential addition of this intervention into the women’s health and gender-related specialty curriculum to address SDOH.
Conclusion
The main limitations of this project were the small sample size and the toolkit format. The small sample size limits the generalizability of the results, but due to a lack of previous projects with SDOH toolkits as their interventions, this project provides a strong foundation for future inquiries on SDOH toolkits in the clinical setting. The toolkit was distributed to the students via university emails and could be pulled up anytime they had internet access, although several students provided feedback that it would be more convenient if the toolkit was integrated into the EHR at their selected sites.
Other students found the online shared document to be a strength because it allowed for easy searching using the finding feature and an electronic table of contents. Another strength of this project was the collection of quantitative and qualitative data, as the quantitative data allowed us to analyze the interventions and their effect on students’ confidence while the qualitative data supported those conclusions and also allowed us to use the feedback from students to further improve the toolkit in the future.
Finally, this QI project paved the way for an SDOH clinical toolkit to be included in WHNP curriculum and strengthened student’s confidence and knowledge in addressing SDOH in the clinical setting. This project has potential for growth and impact. It will be passed on to a future DNP student to streamline its delivery and further improve its efficacy. The toolkit can be readily adapted to any primary care focus and any location within the US. Clinical sites and health systems could utilize this toolkit in their EHR and customize it to the particular patient population or clinical specialty.
Arazu Kian has recently completed a doctorate in nursing practice–women’s health and gender-related nurse practitioner program at the School of Nursing at the University of Minnesota, Twin Cities. The author has no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(5):37-40,IBC. doi: 10.51256/ WHC102337
References
1 Snyder-Mackler N, Burger JR, Gaydosh L, et al. Social determinants of health and survival in humans and other animals. Science. 2020;368(6493):eaax9553.
2 McGinnis JM, Williams-Russo P, Knickman JR. The case for more active policy attention to health promotion. Health Aff (Millwood). 2002;21(2):78-93.
3 Braveman P, Gottlieb L. The social determinants of health: it’s time to consider the causes of the causes. Public Health Rep. 2014;129(suppl 2);19-31.
4 World Health Organization. Gender and health. 2023. https://www.who.int/health-topics/gender#tab=tab_1.
5 Commonwealth Fund. Transforming primary health care for women – Part 1: A framework for addressing gaps and barriers. Fund Re-ports. July 16, 2020. https://www.commonwealthfund.org/publications/fund-reports/2020/jul/transforming-primary-health-care-women-part-1-framework.
6 Palacio A, Tamariz L. Provider perspectives when integrating social determinants of health in response to Schickedanz A, Hamity C, Rogers A, et al. Clinician experiences and attitudes regarding screening for social determinants of health in a large integrated health system. Med Care. 2020;58(2):192.
7 Schickedanz A, Hamity C, Rogers A, et al. Clinician experiences and attitudes regarding screening for social determinants of health in a large integrated health system. Med Care. 2019;57(suppl 6 2):S197-S201.
8 Lewis JH, Whelihan K, Navarro I, Boyle KR; SDH Card Study Implementation Team. Community health center provider ability to identify, treat and account for the social determinants of health: a card study. BMC Family Practice. 2016;17(1):121.
9 American Association of Colleges of Nursing. The Essentials: Core Competencies for Professional Nursing Education. 2021. https://www.aacnnursing.org/portals/42/downloads/essentials/essentials-draft-document.pdf.
10 Thornton M, Persaud S. Preparing today’s nurses: social determinants of health and nursing education. Online J Issues Nurs. 2018;23(3).
11 American Academy of Family Physicians. Assessment and action. 2023. https://www.aafp.org/family-physician/patient-care/the-everyone-project/toolkit/assessment.html.