
In 2015, the Centers for Disease Control and Prevention (CDC) announced that Mycoplasma genitalium was a public health threat.1 Other sources are now calling it a rising sexually transmitted infection (STI) with similar incidence rates to those for chlamydia and gonorrhea.2–4 Recent population-based studies have found the prevalence of M. genitalium to be higher than all other bacterial STIs.4 The purpose of this article is to provide an update for clinicians on symptoms, associated consequences, screening, diagnostic testing, and treatment for M. genitalium.
Associated consequences and risk factors
M. genitalium has been associated with cervicitis, pelvic inflammatory disease (PID), preterm delivery, spontaneous abortion, infertility, and increased risk of infection with human papilloma virus and human immunodeficiency virus (HIV).1,2,4,5 A meta-analysis found that M. genitalium caused a two-fold increase in preterm birth, spontaneous abortion, infertility, cervicitis, and PID.6 Studies have found M. genitalium to be the culprit in 10% to 30% of clinical cervicitis cases.1 Among men, M. genitalium has been linked to asymptomatic urethritis and recurrent urethritis.1 Further research in men is needed to identify a distinct correlation between M. genitalium and epididymitis, prostatitis, and infertility.1,2 M. genitalium is associated with an increased risk for HIV infection among women and men who have sex with men (MSM).1,2 HIV infection is twice as prevalent in women with M. genitalium as compared to those who are negative for it.4
Risk factors for M. genitalium include African American race, previous pregnancy, current bacterial vaginosis (BV) infection, and being younger than age 21 years.7 One prospective US study found that 20% of women who had asymptomatic BV were positive for M. genitalium.8 Another study conducted in Kenya found that an active BV infection increased susceptibility to M. genitalium.4 There also is a correlated risk with increasing numbers of sexual partners for both males and females.4,9 A Denmark correlational study found shorter duration of sexual relationships and first sexual encounter before age 13 years with the increased rates of M. genitalium in women.9 Coinfection with another STI seems to vary across geographic settings in the United States.4
Clinical presentation
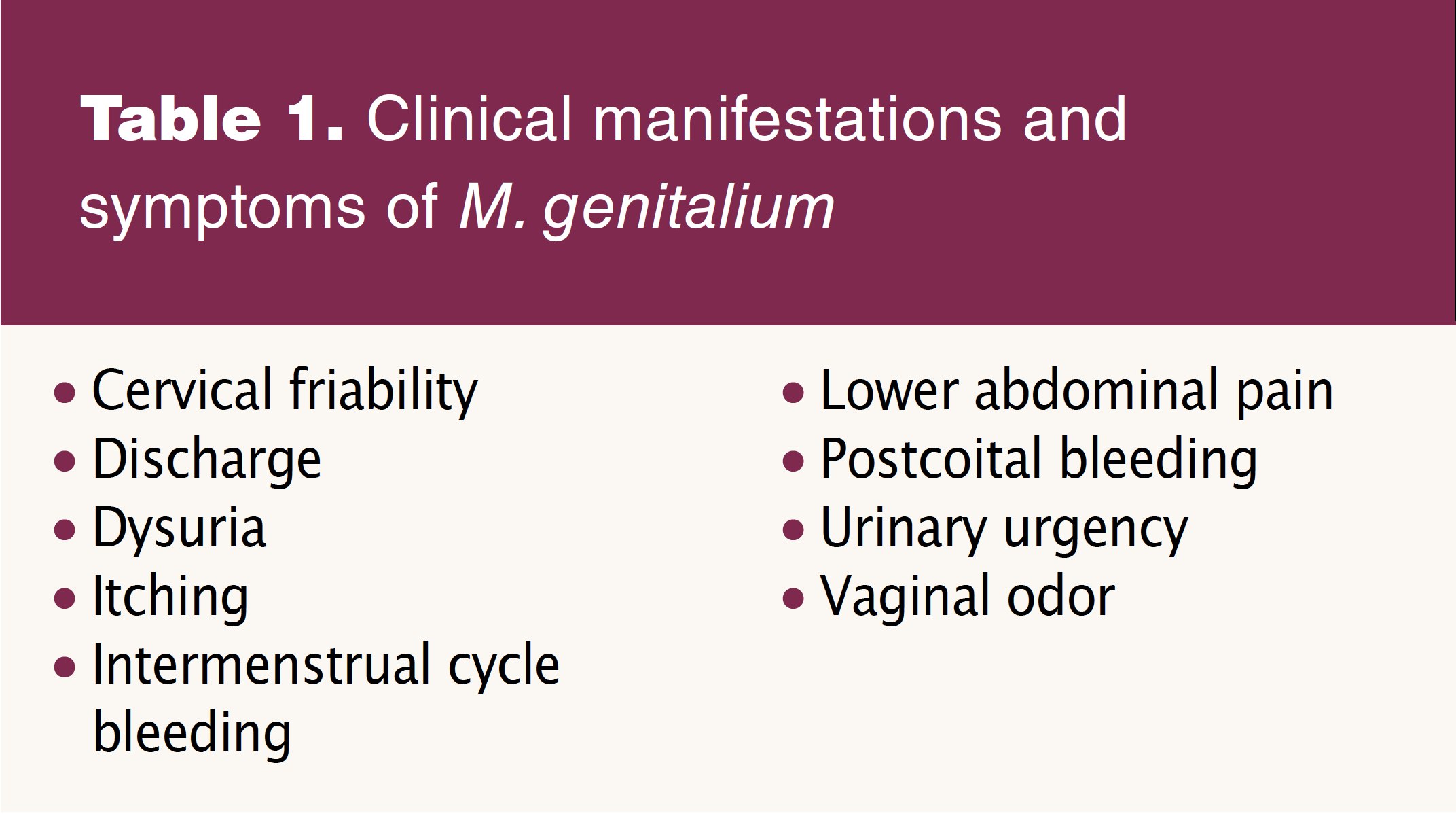
Patients with M. genitalium are often asymptomatic but may present with vaginal odor, discharge, itching, urethritis, dysuria, urinary urgency, intermenstrual cycle bleeding, postcoital bleeding, cervical friability, and lower abdominal pain (Table 1).2–4,10 In men, M. genitalium may present as balanoposthitis, chronic prostatitis, and acute epididymitis.5 Men also demonstrate a strong association between nongonococcal urethritis and M. genitalium.6 M. genitalium has been associated with rectal infections in 3% of women and up to 26% of MSM.1
Screening and diagnosis
Current guidelines for M. genitalium are evolving to identify individuals most appropriate for screening. It is typically found in the cervix or endometrium in women presenting with PID, and it is estimated that about 4% to 22% of women with PID are positive for M. genitalium.1 Women with recurrent cervicitis or PID should be screened with resistance testing if it is available.2 Even if testing is unavailable, M. genitalium should be suspected and potentially treated in these individuals.2 Men with persistent urethritis should be screened for M. genitalium.2 Routine screening for asymptomatic patients is currently not recommended.2
M. genitalium is an extremely slow-growing organism (Figure). Cultures can take up to 6 months to process and are not recommended.2 Because M. genitalium lacks a cell wall, gram staining is ineffective. Serologic testing lacks sensitivity and specificity.4 The US Food and Drug Administration has approved nucleic acid amplification testing (NAAT) with use of urine or urethral, penile meatal, endocervical, and vaginal swab specimens1–4 Given that M. genitalium is rarely seen in the oropharynx, oropharyngeal testing is not necessary.1,4
Treatment
Antibiotics that function by targeting the cell-wall biosynthesis such as beta-lactams or penicillins are ineffective for treatment of M. genitalium.1,2 Metronidazole, the recommended treatment for BV, is not effective.11 The current recommended treatment for PID is not effective against M. genitalium.1
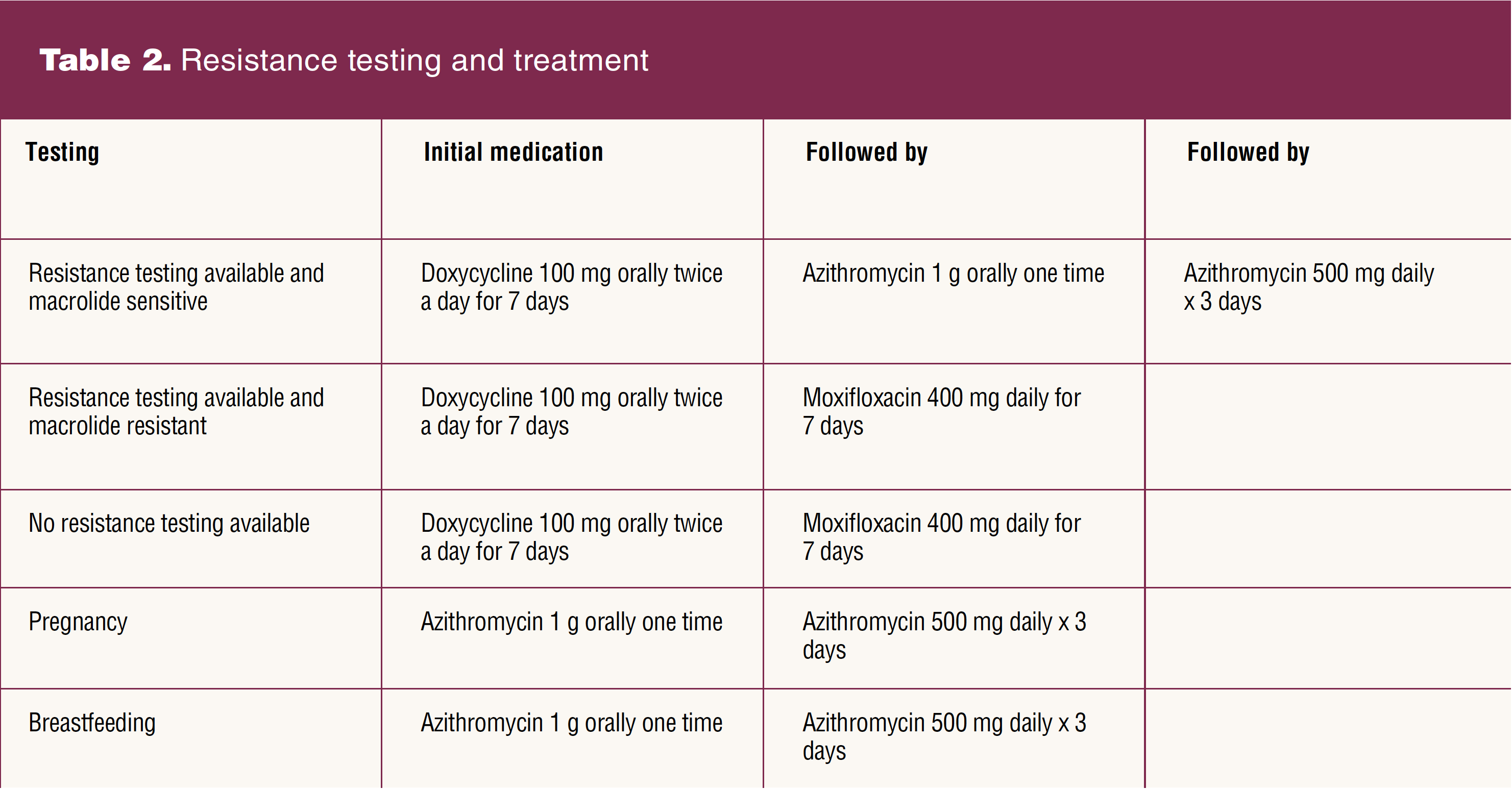
Over the years, treatment for M. genitalium has become more difficult as resistance to microbial therapy is increasing, specifically among macrolides and quinolones.3 Recommended treatment was previously 1 g azithromycin, but multiple studies have found that M. genitalium is showing resistance to azithromycin.1–3 Therefore, two-stage approaches, ideally using resistance-guided therapy, should be used to treat M. genitalium (Table 2). However, antimicrobial resistance testing for macrolide or quinolone markers is not currently available in the US.2 Molecular assays that incorporate detection of mutations associated with macrolide resistance are pending.2 The CDC recommends that where resistance testing is not available, the macrolide-resistant regimen should be used.2 If M. genitalium is detected in the presence of PID, moxifloxacin 400 mg once daily for 14 days should be added to the treatment regimen.1 Using resistance-guided treatment for M. genitalium can increase cure rates to more than 90%.2 Once the patient has been treated with the recommended medications, a test of cure is generally not indicated.1,2
M. genitalium has been found to affect 1% to 8.5% of pregnancies.12 Azithromycin without doxycycline is recommended for M. genitalium in pregnancy and during lactation. Macrolides have not been shown to have adverse fetal or infant effects.12,13 Doxycycline may cause dental enamel staining and growth restriction in the long bones.13 Moxifloxacin is contraindicated in pregnancy and has not been studied in breastfeeding, although fluoroquinolones are typically avoided due to potential risk to the infant’s developing joints.13
Partners of patients diagnosed with M. genitalium can be tested and treated accordingly.1 If testing is unavailable, the partner can be treated with the same regimen as the patient. During the time that partners are being treated, they should abstain from sexual intercourse to reduce the risk of reinfection. Further research is needed to accurately determine rates of reinfection.1
Patient counseling and education
Because patients with M. genitalium may have coinfections, counseling and education should center on discussion of other testing including for HIV, STI prevention, and safer sex practices.4 Providers should encourage condom use for STI protection. STI testing should be encouraged with each new sexual partner to minimize infection risk, ideally before any sexual encounter has occurred. Providers may also encourage patients to have open and honest conversations about their sexual health with their current partner as long as they feel safe and comfortable in doing so. Providers should also educate patients about possible pregnancy implications from M. genitalium including increased risk of infertility, spontaneous abortion, and preterm labor.
Conclusion
M. genitalium is a rising STI that providers should be aware of because it may present as recurrent vaginal infection, intermenstrual bleeding, lower abdominal pain, postcoital bleeding, urinary urgency, and other symptoms similar to vaginitis in women. In males, M. genitalium may present as recurrent urethral or testicular infections. Although current guidelines do not recommend routine screening for M. genitalium, patients with suspected symptoms should be tested and treated according to CDC guidelines. Providers should remain up to date on the most current screening, diagnosis, and treatment guidelines.
Jessica N. Wellette is an Assistant Professor of Nursing at Vanderbilt University School of Nursing and WHNP at VUSN Faculty Nurse-Midwife and Primary Care Practice in Nashville, Tennessee. Shelza J. Rivas is an Assistant Professor of Nursing at Vanderbilt University School of Nursing and WHNP/AGPCNP at VUSN Faculty Nurse-Midwife and Primary Care Practice. Melissa G. Davis is an Associate Professor at Vanderbilt University School of Nursing and the Clinical Director of VUSN Faculty Nurse-Midwife and Primary Care Practice. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
Womens Healthcare. 2023;11(1):33-35. doi: 10.51256/WHC022333
References
1 Mycoplasma genitalium. Centers for Disease Control and Prevention. Updated July 22, 2021. https://www.cdc.gov/std/treatment-guidelines/mycoplasmagenitalium.htm.
2 Workowski KA, Bachmann LH, Chan PA, et al. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Rep. 2021;70(4):1-187.
3 Bowers R. FDA approves new test for Mycoplasma genitalium. Contraceptive Technology Update. April 1, 2019.
4 Manhart LE, Maria T. Mycoplasma genitalium: a review of current issues and challenges. Contemporary OB/GYN. 2017;62(7):1-6.
5 Kent BN. Emerging sexually transmitted disease. Clin Lab Sci. 2017;30(2):124-128.
6 Lis R, Rowhani-Rahbar A, Manhard LE. Mycoplasma genitalium infection and female reproductive tract disease: a meta-analysis. Clin Infect Dis. 2015;61(3);418-426.
7 Nye MB, Harris AB, Pherson AJ, Cartwright CP. Prevalence of Mycoplasma genitalium infection in women with bacterial vaginosis. BMC Womens Health. 2020;20(1):62.
8 Seña AC, Lee JY, Schwebke J, et al. A silent epidemic: the prevalence, incidence and persistence of Mycoplasma genitalium among young, asymptomatic high-risk women in the United States. Clin Infect Dis. 2018;67(1):73-79.
9 Andersen B, Sokolowski I, Østergaard L, et al. Mycoplasma genitalium: prevalence and behavioural risk factors in the general population. Sex Transm Infect. 2007;83(3):237-241.
10 Kronemyer B. Mycoplasma genitalium as prevalent as Chlamydia trachomatis at clinic. Contemporary OB/GYN. 2021;66(9):36.
11 Taylor-Robinson D. Mollicutes in vaginal microbiology: Mycoplasma hominis, Ureaplasma urealyticum, Ureaplasma parvum and Mycoplasma genitalium. Res Microbiol. 2017;168(9-10):875-881.
12 Donders G, Ruban K, Bellen G, Petricevic L. Mycoplasma/ureaplasma infection in pregnancy: to screen or not to screen. J Perinatal Med. 2017;45(4): 505-515.
13 Drugs and Lactation Database (LactMed). US National Library of Medicine. https://www.ncbi.nlm.nih.gov/books/NBK501922/.