
Advanced health assessment skills training is an integral part of advanced practice nursing education.1 The educational curriculum for women’s health nurse practitioner (WHNP) students includes skills training in physical assessment of women. Pelvic health assessment is an essential skill in achieving women’s health/gender related core competencies for nurse practitioners.2 Components of pelvic health assessment include external genitalia inspection, vaginal speculum examination, and vaginal, cervical, and external genitalia specimen collection.
Competencies are observed demonstrations of abilities. Demonstration of beginning competency in pelvic health assessment is foundational for WHNP students entering clinical practica.3 To ensure clinical competency, faculty-observed demonstration of essential skills by students is necessary. Traditional methods for demonstration of skills during in-person classes include the use of simulation models or surrogate patients. Virtual classes typically lack access to these resources. To facilitate student learning and clinical competency demonstration, a vaginal simulation model was developed for use in the virtual learning format. This article describes development of the model, evaluation of use with WHNP students enrolled in an introductory women’s health (WH) skills course, and considerations for future applications.
Model design
Inspiration for this design was the move from in-person to virtual teaching necessitated by the Covid-19 pandemic. The initial goal of the model development was to facilitate virtual teaching of speculum examination skills by providing student learners with tools for hands-on application. Essential components of the model needed to include a cervix with a cervical os, vaginal walls to simulate the vault, as well as external anatomic features. Identification of low-cost, readily accessible supplies was also a key component in what was planned to be a student-assembled model. Original plans were to provide students a supply list for individual model assembly prior to the first class.
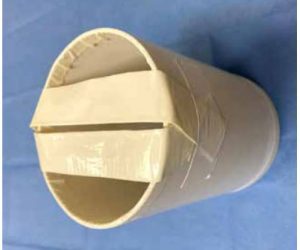
The initial prototype was a cardboard cylinder sized to approximate the vaginal opening, a skein of yarn to simulate internal musculature, and a rubber dog toy to simulate the cervix. The limitation of cervical placement in this design quickly led to replacement of the cardboard with a larger PVC cylinder. The 4-inch diameter PVC cylinder drain pipe was readily available at low cost in plumbing departments from local building supply companies. To ensure equitable access of supplies for all enrolled students and consistency in model assembly, the original plan for self-purchase and assembly by students was changed to a school-funded plan with faculty assembly and mailing of models and supplies to each student. The PVC cylinder had the additional advantage of durability during mailing. Additional materials and tools used to construct the model are listed here:
- 4” diameter PVC drain pipe cut into 6” long sections –need one section per model
- Alternate: 4” diameter mailing tube cut into 6” sections
- Fine grit sandpaper to smooth the rough PVC cut edges
- Duct tape for anatomic shaping
- ¾” to 1” thick foam roll or Poly-fil dry polyester packing fiber fill
- 24” latex balloon
- Paddle ball red rubber game ball only
- Super glue w/brush attachment to affix paddle ball to latex balloon
- Foam board or cardboard
- Alternate: if using mailing tube, end caps can be used instead of foamboard/cardboard
- Flesh-colored trouser sock to cover latex balloon for latex-allergic students
Tools
- Drill with 3/16” bit, ¼” bit
- Scissors
- Box cutter
- Ink pen
- Hacksaw or band saw to cut drain pipe/cardboard mailer tube
After supplies and tools were gathered, model construction began. Sequential steps included the following:
- Cut drain pipe to 6” lengths.
- Sand the rough ridges and cover with duct tape to prevent any injury when handling the pipe. Preference is 120 grit sandpaper. Advantage of using alternate cardboard mailer tube is elimination of need to sand edges and reduction of overall weight of model.
- Tear two strips of duct tape approximately 8” long
- Fold tape over on itself so that you have two 4” nonsticky strips of tape. These will serve to give some structure at the opening of the pipe, simulating vaginal introitus. Secure strips across middle of pipe opening.

- Using scissors, cut a half-circle in the top portion of the deflated balloon. Note: cutting a simple slit encourages unwanted tearing when manipulating the balloon over the pipe opening.

- Obtain paddle ball toy and remove ball portion from paddle and string. Using a 3/16” bit, drill hole in the ball so that cytobrush may fit. Note: the rubber ball is very soft. Using smaller bits and gradually opening the hole will allow for a more uniform os.

- Place newly drilled ball into the spout of the balloon so that the os opens near the middle of balloon spout. Note: the easiest and cleanest way to secure the ball into the balloon spout is using super glue with a brush attachment to slide between the ball and balloon after placement.

8. Allow a few seconds for the super glue to cure.
9. Place the balloon spout with the secured ball through the tape slit opening so that the top of the balloon with the halfcircle cut is now at the level of duct tape pipe slits.
10. Pull the cut opening of the balloon over the outside of the pipe.
11. Turn the model over so that you may begin to fill the inside of the model with foam and/or poly-fil. Fill the void with poly-fil to desired consistency of the vault.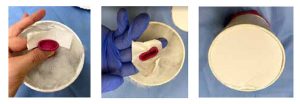
12. Anchor the balloon to the back of the model. If using PVC drain pipe, use cardboard/foam board circle and duct tape as described and shown in this illustration. Cut the foam board circle to fit the inner diameter of the pipe. Pre-tear an approximate 2” strip of duct tape and split it lengthwise into two strips to attach the balloon to the foam board circle. Place the tape strips around the balloon spout opening sticky side up. Press the foam board cutout against the tape to secure the tape/balloon and provide a barrier for the poly-fil to not leak out. If using cardboard mailer tube end cap, drill a ¼” hole in the center of the cap that the balloon spout opening may be threaded into to secure in place.
13. Once you have a completed model, do a quality check. Use water-soluble lubrication on the model to preserve the latex balloon lining when inserting the speculum. For sustained use, the lubricant should be cleaned from the model at the conclusion of the practice session. This is intended to be a “normal” speculum cervical exam. The os should be midline and centered within the model. Insert the endocervical
brush to ensure adequate entry and removal and to ensure the rubber ball remains in place on endocervical brush removal.
14. Modifications may be made to the model by slipping the latex balloon off of the front of the model and adding/removing stuffing. The duct tape strips providing structure to the model may also need adjustment to allow for improved speculum insertion.
15. If a person is allergic to latex, a nylon trouser sock may be used to cover the latex balloon. Cut off the seam at the toes then slip it over the outside of the model to provide an added layer of protection.
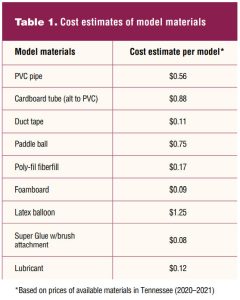
Cost estimates for all materials are listed in Table 1.
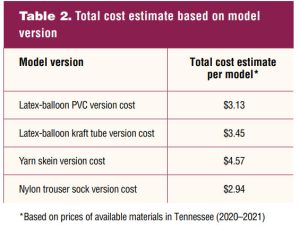
The total cost estimates based on model versions are listed in Table 2.
Use of model
Students received assembled simulation models and specimen collection supplies prior to the first virtual lab scheduled at the beginning of their WH specialty year. Supply kits included disposable gloves; a plastic speculum; individually packaged lubricant; collection vials for Pap, chlamydia/gonorrhea, herpes simplex virus, and group B strep testing; cytobrush; spatula; spatula broom; long and short cotton-tipped applicators; ph paper; individual saline and KOH [potassium hydroxide] ampules; and a biohazard bag. Four virtual lab sessions were scheduled involving use of the simulation model. Themes for the four sessions were: introduction, practice, demonstration, and reinforcement. Faculty posted self-recorded videos of lab skills for student review before the initial introductory lab.
During the initial virtual session, faculty demonstrated assessment skills using the model, which was followed by student practice in small faculty-led groups of 5 to 6 students per group. Students were instructed on the use of smart phones as a secondary camera to aid faculty observation during skills practice. The second virtual session focused on group and individual practice, with each student demonstrating skills under faculty guidance. The third virtual session was devoted to faculty evaluation of individual student performance of beginning proficiency in pelvic health assessment skills using the simulation model. The fourth and final virtual session focused on remediation as required and reinforcement of skills. Between each session, independent student practice was encouraged.
Evaluation
Feedback on pre and post use of the model was collected from students via REDCap survey after receiving Institutional Review Board approval. The survey included demographic data on program entry level and practice experience. The entry levels to our MSN program include pre-RN licensure or pre-specialty, direct entry with a BSN, and Post-Master’s Certificate (PMC). Direct entry students may enter the program with nursing experience since BSN completion or directly upon graduation from BSN programs without nursing experience. The PMC students may enter as APRNs with certification in another specialty or MSN-prepared nursing leaders or educators. Survey questions regarding program entry provided selection options for each of the entry levels.
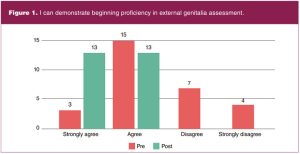
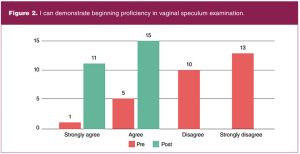
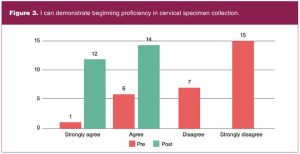
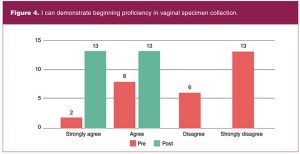
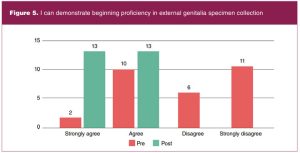
Practice experience was assessed with a yes or no response option for direct entry and PMC students. Those indicating prior practice experience received a drop-down menu to indicate months or years in practice. Students’ current level of preparation in external genitalia assessment, vaginal speculum assessment, cervical specimen collection, vaginal specimen collection, and external genitalia specimen collection was assessed using five statements regarding demonstration of beginning proficiency. Beginning proficiency was defined as basic knowledge. A 4-point Likert scale with responses ranging from strongly agree to strongly disagree was provided for student responses.
Analysis
A non-parametric Wilcoxon signed rank test was used to evaluate if there was a change in scores between pre and post surveys. The P-values were all less than 0.05 indicating that the distribution in post-test scores were statistically different from the pre-test scores with increased proficiency indicated post test.
Results
All 29 students enrolled in the course completed the pre-test. Fourteen students identified as pre-specialty entry, 14 as BSN-prepared direct entry, and one as PMC. Of the 15 combined direct and PMC entry students, seven indicated no practice experience. The remaining eight with practice experience indicated lengths of practice time ranging from 1 month to greater than 12 years. Of 28 students enrolled at course completion, 26 completed the post-test. Pre-and post-test proficiency survey data are shown in Figures 1 through 5.
Lessons learned
Survey results demonstrated student learning during virtual teaching was achieved in each of the 5 competencies that were assessed. Provision of the simulation model afforded students structured, hands-on practice during scheduled class times and unlimited, independent practice time outside of class. The model also allowed faculty the opportunity to observe student demonstration of essential skills in a virtual format.
Between initial introduction and subsequent use, the model evolved in design materials and assembly leading to a more stream-lined process. The original PVC pipe has been replaced with a cardboard mailing tube that is easier to cut into 6” lengths. Use of a hacksaw for cutting the tubes has been replaced with a band saw, which greatly decreased the time and effort required for cutting the tubes. The 12” mailing tubes require only one cut for the desired 6” length leaving the rim at one end clean and eliminating the need for filing then taping that the PVC pipe required. Additionally, the mailing tubes come with end covers that eliminate the need for cutting cardboard to size for the PVC pipe openings.
The cylindrical design requires stabilization of the model prior to use. With the initial models, a cardboard stand was included for stabilization and elevation of the model. Cardboard was cut by hand and taped together to form the stands. The stands were designed to fold flat for mailing. Rubber drawer liner for stabilization of the stand itself was included in each supply kit.
Due to the time-intensive requirements of stand construction, they were eliminated in the second year of use. Instead, students were advised to elevate the model with textbooks or yoga blocks and stabilize it with modeling putty included in the supply kit. We also found that sufficient wedging of the rubber paddle ball into the mouth of the latex balloon eliminated the need for gluing the ball in place. It also allowed for alternate positioning of the ball to change the os location as desired.
Future plans
As students progress in skills training, more challenging models may be substituted. Cervical os placement may be changed from an anticipated midline uterine location to simulate ante/retroverted or ante/retroflexed placements. Firmer rubber balls may be substituted for the paddle balls to simulate a stenotic cervical os.
A trouser sock is currently used in model modification for the latex-allergic student. Elimination of the latex component remains an ongoing goal for future models. We continue to search for suitable alternatives to the latex balloons.
Applications for model use in other settings include sexual assault nurse examiner training, proficiency maintenance for providers with limited opportunities for pelvic examinations, and as a low-cost training method for institutions with limited resources for simulation or surrogate training experiences.
Assembly of all the initial models that were mailed to students was accomplished by one faculty member. Although overall costs of the model are low, the workload required was not sustainable. To address this barrier, an end of the year party will be scheduled with WH faculty and soon-to-be graduates assembling models for the incoming cohort of WHNP students. Current students may also return models for recycling once the intended clinical competencies are achieved. In addition to accomplishing the goal of time-efficient and cost-effective model assembly, we anticipate this annual event will become a welcomed source of community building for faculty and students.
Conclusion
The Covid-19 pandemic presented challenges but also provided opportunities for development of innovative teaching strategies. The vaginal simulation model was initially conceived as a strategy to enhance student learning during virtual teaching. Continued use of the model beyond the pandemic will provide students with a method for unlimited, independent practice not previously available.
Ginny Moore is Associate Professor and Director of the WHNP specialty at Vanderbilt University School of Nursing in Nashville, Tennessee. JoEllen Holt is Assistant Professor and Director of the skills and simulation lab at Vanderbilt University School of Nursing. Rameela Raman is Associate Professor of biostatistics at Vanderbilt University School of Medicine. The authors have no actual or potential conflicts of interest in relation to the contents of this article.
References
- American Association of Colleges of Nursing. The Essentials: Core Competencies for Professional Nursing Education. 2021.
- National Organization of Nurse Practitioner Faculties. Population-focused nurse practitioner competencies. 2013.
- Nurse Practitioners in Women’s Health. Women’s Health Nurse Practitioner: Guidelines for Practice and Education, 8th ed. Washington, DC: National Association of Nurse Practitioners in Women’s Health; 2020.