
Persistent genital arousal disorder (PGAD) is a perplexing and elusive health condition of unknown prevalence. Until recently, little was known about its etiology or amenability to treatment. However, re- cent advances in sexual medicine research provide a better understanding of PGAD, enhancing health- care providers’ ability to properly diagnose and manage it. In part 1 of this two-part series, diagnosis and management of PGAD are discussed; in part 2, the focus is on the patient experience of PGAD.
Medical models of sexual response represent arousal as a desirable and pleasurable experience.1-3 In some women, however, genital arousal occurs in the absence of sexual interest or desire. First described in the literature by Leiblum and Nathan,4 persistent genital arousal disorder (PGAD), previously referred to as persistent genital arousal syndrome, is manifested by intrusive and unwanted symptoms such as persistent genital arousal, vulvar congestion, discomfort, and even pain.5 In such cases, orgasm provides little or only short-lived relief. Markos and Dinsmore6 liken the presentation of PGAD to that of vulvodynia. Of note, although cases of male PGAD have been reported as well,7 this article focuses on female PGAD.
Many healthcare providers (HCPs) are unaware of the existence of PGAD, leaving many women who have this condition without a timely diagnosis or treatment. Even if some HCPs are aware of PGAD, their patients may hesitate to mention their symptoms because the condition is so highly stigmatized. In fact, approximately 25% of women with PGAD wait more than 10 years to report symptoms to their HCP or they never report their symptoms.8
Prevalence and etiology
Little is known about PGAD prevalence. Most research on PGAD is in the form of case studies or surveys of limited populations.9,10 PGAD is likely under-reported because of patient embarrassment and fear of being labeled as hypersexual.11 A survey of a sexual health practice in the United Kingdom identified a PGAD prevalence of approximately 1% with all the diagnostic characteristics of the condition, although 33% of participants reported at least one identifying characteristic of PGAD.12 PGAD appears to affect women of all ages.4 A recent survey of more than 100 women with PGAD indicated an age range of 18-79 years (mean age, 47 years).10
No consensus exists regarding the etiology of PGAD, although it is thought that symptoms may arise as a result of dysregulation at central and peripheral levels.11 In addition, psychological conditions and external factors such as diet and pharmacologic agents may elicit symptoms of persistent arousal.11 Antidepressant use is cited as a trigger in 20% of women with PGAD.13 Vascular anomalies of the pelvis and compression of the pudendal nerve, as with Tarlov cysts, may play a role in some cases.14-16
Diagnosis
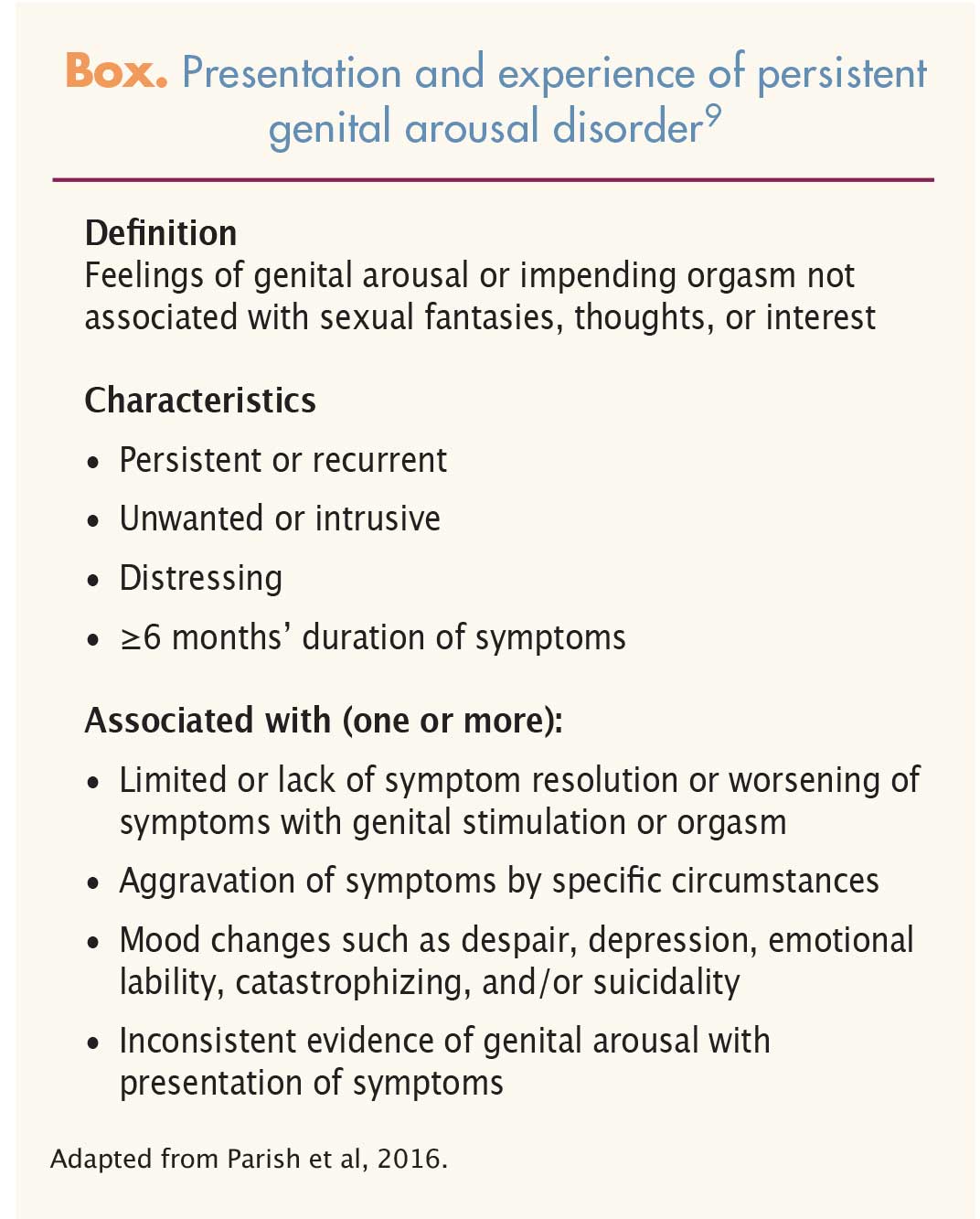
Women vary in terms of the presentation and experience of PGAD (Box).9 Because women may hesitate to disclose information about PGAD, HCPs should consider asking those presenting for annual checkups about whether they experience any genital pain, discomfort, persistent arousal, numbness, tingling, or throbbing.13,17 If PGAD is suspected, HCPs should review the patient’s health history, with a focus on potential co-morbidities and past/ current medication use, supplement use, and illicit drug use. Diet and exercise are important factors when assessing for PGAD.17 In addition, women should be asked about past and current sexual practices and partner(s), as well as a possible history of sexual abuse or trauma.
{kind=link}
A comprehensive vulvovaginal and pelvic examination, including a neurologic and musculoskeletal assessment, can identify or exclude overt structural defects. In some cases, laboratory testing (e.g., thyroid panel, prolactin level, testosterone panel) and imaging studies (e.g., pelvic ultrasonography, magnetic resonance imaging) may provide useful diagnostic information.15 Women with PGAD should be screened for symptoms of restless leg syndrome (RLS) and overactive bladder (OAB). If symptoms of RLS and/or OAB co-exist with those of PGAD, a diagnosis of restless genital syndrome should be considered.5,18
Treatment
No medications are currently indicated specifically for the treatment of PGAD. All pharmacologic interventions for PGAD discussed in this article are investigational. Of note, HCPs should address potentially reversible causes of PGAD before pursuing further intervention.4 As with many complex and poorly understood health conditions, the treatment for PGAD necessitates an interdisciplinary approach, with consideration of all potential biopsychosocial causes.4 Further supporting the multifactorial causation of PGAD is the fact that clitoridectomy does not appear to benefit patient outcomes.19
Dysregulation of sensory excitation remains the focus of pharmacologic intervention for PGAD.20 Off-label use of medications such as selective serotonin reuptake inhibitors, varenicline, zolpidem, and tramadol appears to reduce PGAD symptoms in some cases, although further research is needed.17,20 Of interest, withdrawal from the aforementioned medications has been implicated in the onset of PGAD.17 Surgical correction of Tarlov cysts may effectively treat PGAD, whereas periclitoral injections of botulinum toxin do not appear to improve symptoms long term.14,16,21 Electroconvulsive therapy may ameliorate PGAD symptoms in patients with co-morbid bipolar disorder.22
Recommendations
Persistent genital arousal disorder is a legitimate health condition that warrants increased HCP awareness.10 Although PGAD is often represented in a comedic light, it is no laughing matter to women who carry the daily burden of the embarrassing and debilitating symptoms that accompany it. Women with PGAD report insensitive comments from their HCPs such as “You should be a porn star” or “Your symptoms are every husband’s dream.”10 Comments from a trusted HCP that embarrass, insult, or ridicule an already vulnerable woman can have devastating consequences. Compared with the general population, patients with PGAD have a two-fold increase in suicidal ideation.13 Care of patients with PGAD begins by providing a safe and nonjudgmental atmosphere in which to facilitate an open and honest discussion. If PGAD is suspected, HCPs can consider referral to a sexual medicine provider or visit the International Society for the Study of Women’s Sexual Health (ISSWSH) website for more resources.
Brooke M. Faught is a nurse practitioner and the Clinical Director of the Women’s Institute for Sexual Health (WISH), A Division of Urology Associates, in Nashville, Tennessee. She is an ISSWSH Fellow. The author states that she serves as a speaker and advisory board member for Shionogi and Valeant and an advisory board member for the Female Health Company.
References
- Masters WH, Johnson VE. Human Sexual Response. Boston, MA: Little Brown; 1966.
- Kaplan HS. The New Sex Therapy. New York, NY: Brunner/Mazel; 1974.
- Basson R. Using a different model for female sexual response to address women’s problematic low sexual desire. J Sex Marital Ther. 2001;27(5):395-403.
- Leiblum SR, Nathan SG. Persistent sexual arousal syndrome: a newly discovered pattern of female sexuality. J Sex Marital Ther. 2001;27(4):365-380.
- Waldinger MD, Schweitzer DH. Persistent genital arousal disorder in 18 Dutch women: part II. A syndrome clustered with restless legs and overactive bladder. J Sex Med. 2009;6(2):482-487.
- Markos AR, Dinsmore W. Persistent genital arousal and restless genitalia: sexual dysfunction or subtype of vulvodynia? Int J STD AIDS. 2013;24(11):852-858.
- Waldinger MD, Venema PL, van Gils AP, et al. Stronger evidence for small fiber sensory neuropathy in restless genital syndrome: two case reports in males. J Sex Med. 2011;8(1):325-330.
- Jackowich R, Pink L, Gordon A, Pukall C. Prevalence of persistent genital arousal disorder criteria in a sample of Canadian undergraduate students. Poster session presented at: Annual Meeting of the International Society for the Study of Women’s Sexual Health; February 23-26, 2017; Atlanta, GA.
- Parish S, Goldstein A, Goldstein S, et al. Toward a more evidence-based nosology and nomenclature for female sexual dysfunction-part II. J Sex Med. 2016;13(12):1888-1906.
- Jackowich R, Pink L, Gordon A, Pukall C. Health care experiences of women with symptoms of persistent genital arousal. Poster session presented at: Annual Meeting of the International Society for the Study of Women’s Sexual Health; February 23-26, 2017; Atlanta, GA.
- Jackowich R, Pink L, Gordon A, Pukall C. Persistent genital arousal disorder: a review of its conceptualizations, potential origins, impact and treatment. Sex Med Rev. 2016;4(4);329-342.
- Garvey LJ, West C, Latch N, et al. Report of spontaneous and persistent genital arousal in women attending a sexual health clinic. Int J STD AIDS. 2009;20(8):519-521.
- Pukall CF, Jackowich R. Persistent genital arousal disorder: when is pain assessment relevant? Presented at: International Society for the Study of Women’s Sexual Health Annual Meeting. February 23-26, 2017; Atlanta, GA.
- Komisaruk BR, Lee HJ. Prevalence of sacral spinal (Tarlov) cysts in persistent genital arousal disorder. J Sex Med. 2012;9(8):2047-2056.
- Pink L, Rancourt V, Gordon A. Persistent genital arousal disorder in women with pelvic and genital pain. J Obstet Gynaecol Can. 2014;36(4):324-330.
- Feigenbaum F, Boone K. Persistent genital arousal disorder caused by spinal meningeal cysts in the sacrum. Obstet Gynecol. 2015;126(4):839-843.
- Facelle TM, Sadeghi-Nejad H, Goldmeier D. Persistent genital arousal disorder: characterization, etiology, and management. J Sex Med. 2013;10(2):439-450.
- Aquino CC, Mestre T, Lang AE. Restless genital syndrome in Parkinson disease. JAMA Neurol. 2014;71(12):1559-1561.
- Waldinger MD, Venema PL, van Gils AP, et al. Restless genital syndrome before and after clitoridectomy for spontaneous orgasms: a case report. J Sex Med. 2010;7(2 pt 2):1029-1034.
- Pfaus JG. Persistent genital arousal disorder-fact or fiction? J Sex Med. 2017;14(3):318-319.
- Rubin R, Winter A, Minton J, et al. Peri-clitoral botulinum toxin as a treatment for persistent genital arousal disorder (PGAD). Poster session presented: Annual Meeting of the International Society for the Study of Women’s Sexual Health. February 23-26, 2017; Atlanta, GA.
- Yero SA, McKinney T, Petrides G, et al. Successful use of electroconvulsive therapy in 2 cases of persistent sexual arousal syndrome and bipolar disorder. J ECT. 2006;22(4):274-275.