Syphilis is a sexually transmitted infection that manifests as a chronic systemic disease. Each of the different stages of infection involves specific symptoms that can be overlooked or confused with those of other diseases. Adequate screening for syphilis in women at risk, combined with appropriate treatment and follow-up as indicated, is essential to reduce the risk of transmission and disease complications.
Syphilis is a chronic systemic disease caused by the spirochete Treponema pallidum. In the United States, syphilis is a reportable disease whose rates are monitored by the CDC. Since 1944, when syphilis first became a nationally notifiable disease, syphilis rates declined steadily; rates for women were among the lowest of all.1 Despite the lower overall rates of syphilis nationwide over the past seven and a half decades, certain population subgroups started becoming more affected in recent years. For example, from 2000 to 2016, syphilis rates have risen among men who have sex with men (MSM) and who are younger than 34 years; this subgroup had the highest reported rates of syphilis in the country.1 But this subgroup has not been the only one to experience an increase in syphilis incidence. In fact, from 2015 to 2016, syphilis rates rose in the U.S. for all groups of individuals older than 15 years, regardless of race, ethnicity, sexual orientation, or gender—including a 35% increase in women.1 After decades of little fluctuation, the rise in syphilis diagnoses among women is concerning; higher rates of syphilis for women of childbearing age are often linked to higher rates of congenital syphilis (CS) in neonates.1 Although no definitive evidence exists to explain this rise in syphilis incidence, researchers suggest that it may be due to individual-level factors (e.g., multiple partners, partner concurrency) combined with social-level factors such as poverty, homelessness, and lack of access to care.1 In light of these data, this article provides an overview of syphilis and includes information about risk reduction, screening, and diagnosis; treatment options; implications of syphilis in pregnant women; CS; and general implications for healthcare providers (HCPs) who see women in their practices.
Overview
Disease stages
Syphilis presents in several stages over time; signs and symptoms (S/S) in women vary according to disease stage. A primary syphilis infection initially presents with the appearance of a painless ulcer called a chancre (Figure 1), which can be located at the initial site of treponemal infiltration of the skin. Infiltration sites involved with sexual activity include the genitals (vulva, vagina), the rectum/anus, and the oral cavity. Because a chancre does not cause discomfort, women can miss this initial sign, especially if it is in an area not easily noticeable, such as the vaginal wall or anus. The primary stage lasts up to 5 weeks; even with-out treatment, a chancre heals on its own.2 Inguinal lymphadenopathy may be present if the chancre is located in the genital area and cervical lymphadenopathy may be noted if it is in the oral cavity.3
Women who do not receive treatment for primary syphilis progress to secondary syphilis. In this stage, local S/S are absent and systemic S/S such as fever, headache, malaise, lymphadenopathy, and rash may occur. If not treated, the infection enters the latent stage. Latent syphilis is characterized by a positive serologic test for the disease in the absence of S/S. 4,5 The latent stage is further classified into early latent (syphilis acquired in the past year) and late latent (syphilis acquired >1 year previously).5 The latent stage can last for years. Tertiary syphilis is a subset of untreated syphilis that can manifest decades after the infection was acquired. Tertiary syphilis can affect multiple organs, including the liver, heart, brain, joints, bones, and eyes. If the infection involves the nervous system, referred to as neurosyphilis, a wide range of S/S such as head-ache, dementia, altered behavior/mood, and difficulty with muscle coordination and movement can occur. Neurosyphilis is most common in the later stages of the disease but can occur with early infections. The tertiary stage may be fatal.4-6
4,5 The latent stage is further classified into early latent (syphilis acquired in the past year) and late latent (syphilis acquired >1 year previously).5 The latent stage can last for years. Tertiary syphilis is a subset of untreated syphilis that can manifest decades after the infection was acquired. Tertiary syphilis can affect multiple organs, including the liver, heart, brain, joints, bones, and eyes. If the infection involves the nervous system, referred to as neurosyphilis, a wide range of S/S such as head-ache, dementia, altered behavior/mood, and difficulty with muscle coordination and movement can occur. Neurosyphilis is most common in the later stages of the disease but can occur with early infections. The tertiary stage may be fatal.4-6
Transmission and risk factors
Primarily considered a sexually transmitted infection (STI), syphilis is communicated through mucosal surfaces during oral, vaginal, or anal contact. In addition, the disease can be transmitted vertically from mother to child during pregnancy and delivery.7 The incubation period for primary syphilis is 9-90 days, but the average time from inoculation to appearance of a chancre is 2-3 weeks.3 Risk factors for syphilis include history of a previous infection, having more than four sexual partners in the preceding year, and being HIV positive.2 Specific population subgroups are at higher risk, including MSM, individuals who are incarcerated, sex workers, individuals who trade sex for drugs and/or money, and those who identify as black or African American.
Risk reduction, screening and diagnosis
No vaccine for syphilis exists; therefore, public health initiatives to reduce transmission of the infection and prevent sequelae focus on risk reduction, screening, and diagnosis.
Risk reduction
Syphilis is transmitted primarily through sexual contact. Risk-reduction strategies include practicing safer sexual behaviors such as using condoms, limiting the number of sexual partners, and avoiding partner concurrency. Sexual contact should be avoided with individuals who have untreated syphilis. Individuals who have completed treatment should follow up with their HCP to determine their current status.5
Screening
The U.S. Preventive Services Task Force recommends that MSM or men who are HIV+ undergo syphilis screening every 3 months, but it did not find evidence to support the efficacy of this frequency of screen-ing in non-pregnant adult women or in men who have female sexual partners.4 Increased screening for women who are HIV+ is advised, but no definitive screening interval has been recommended. In addition to MSM and HIV+ individuals, the CDC recommends syphilis screening for all pregnant women and for individuals who are incarcerated in a facility or geographic area with high prevalence of syphilis.5 These recommendations notwithstanding, decisions about syphilis screening are based on history, patient concerns, and examination findings.
Diagnosis
The gold standard for definitive detection of syphilis is a dark-field microscopy examination of exudate from a primary lesion to identify T. pallidum.5 However, because few clinical practice settings have the capacity or equipment for this type of testing, serologic screening is most commonly utilized. To decrease the possibility of false-negative or false-positive results, two serologic tests are necessary to establish a diagnosis of syphilis. As part of the traditional screening algorithm (Figure 2),4,5 initial serology is often completed with a rapid plasma reagin (RPR) or venereal disease research laboratory (VDRL) nontreponemal test. If the result is positive, it must be followed by a 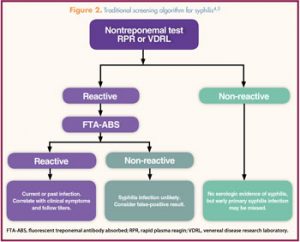 treponemal test such as a fluorescent treponemal antibody absorbed (FTA-ABS) test.5 Initial false positive RPR test results can occur in patients with HIV infection, an autoimmune disease, injection drug use, recent vaccination, or pregnancy when no syphilis infection is present. All positive RPR tests must be followed by a treponemal test before a diagnosis of syphilis can be confirmed.
treponemal test such as a fluorescent treponemal antibody absorbed (FTA-ABS) test.5 Initial false positive RPR test results can occur in patients with HIV infection, an autoimmune disease, injection drug use, recent vaccination, or pregnancy when no syphilis infection is present. All positive RPR tests must be followed by a treponemal test before a diagnosis of syphilis can be confirmed.
A reverse sequence screening agorithm can be used in which treponemal antibody tests are obtained first and then followed by nontreponemal tests. This approach has been suggested for geographic areas and populations with high syphilis rates (e.g., MSM). The advantage of the reverse algorithm is a more rapid identification of persons who have the disease. The positive predictive value of using treponemal testing first in a lower-risk population may not be as robust and yield a higher amount of false-positive results.2,4,5 Limited data suggest that a reverse sequence algorithm could be implemented with men or women at low or average risk of having syphilis, although incidences of false-positive results might be higher.4
Once a diagnosis of syphilis has been made, a nontreponemal test is used to follow response to treatment. Titers are expressed as a ratio; a fourfold change is required to demonstrate existence of a clinically significant difference.5 A fourfold decrease should be expected with adequate treatment, whereas a fourfold rise in titers can occur in untreated syphilis. For example, if the initial nontreponemal titer is 1:32, HCPs should expect to see a titer of 1:8 or less after completion of treatment. Both the RPR and VDRL are appropriate to monitor treatment response, but sequential nontreponemal titers should be done with the same test for accurate interpretation of results. Because syphilis is a nationally notifiable disease, HCPs must report all positive results to their state department of public health.
Treatment
Benzathine penicillin G, administered intramuscularly (IM), is the preferred treatment for individuals with syphilis in any stage. Dosage and length of treatment depend on the stage and the clinical manifestations of the disease (Box).5 For late latent syphilis and tertiary syphilis, including tertiary-stage neurosyphilis, a longer duration of therapy is indicated. Effectiveness of penicillin for treatment of syphilis was established not only through clinical trials and observational studies but also over many decades of clinical experience.5
• Primary, secondary, or early latent stage: 2.4 million U IM in a single dose
• Late latent, tertiary stage, or disease of unknown duration: 2.4 million U IM/week x 3 weeks (total dose, 7.2 million U)
• Neurosyphilis without clinical neurologic symptoms: treat based on disease stage
• Neurosyphilis with neurologic symptoms: 18-24 million U/day aqueous crystalline penicillin G, administered as 3-4 million U IV every 4 hours or by continuous IV infusion, for 10–14 days
IM, intramuscularly; IV, intravenously.
In addition, HCPs need to con-sider the management of patients who have had sexual contact with individuals diagnosed with syphilis. Sexual transmission of T. pallidum is thought to occur only when mucocutaneous syphilitic lesions are present, but such manifestations are uncommon after the first year of infection.5 Patients who have had sexual contact in the past 90 days with a person infected with primary, secondary, or early latent syphilis should be presumptively treated for syphilis even if the serologic testing result is negative. If sexual contact with an infected individual occurred more than 90 days prior, the patient should undergo serologic testing and be treated based on results. If serologic testing is unavailable or not possible or if the patient is un-likely to return for treatment after testing, then presumptive treatment should be initiated.5
Patients who are treated for syphilis at any stage need to be followed after treatment. Clinical and serologic evaluation should be per-formed 6 and 12 months post-treatment, but more frequent evaluation may be needed if follow-up is uncertain or repeat infection is suspected. Follow-up results are compared with the original serologic test results to determine response to treatment or possibility of a new infection.5
Syphilis treatment may precipitate the Jarisch-Herxheimer reaction. This acute febrile reaction results from destruction of spirochetes and an increase in proinflammatory cytokines and endotoxins. Along with fever, patients may develop myalgia, chills, and headache. Onset of the reaction is often rapid, occurring within the first 8 hours after treatment with antibiotics. The reaction resolves within 24-48 hours. The Jarisch-Herxheimer reaction is more common among individuals with an early syphilis infection.5 Treatment is supportive.5
Implications for pregnant women
More than 1 million pregnant women around the world are infected with syphilis.8 Pregnancy provides a unique opportunity to screen women for syphilis and review risk factors and risk reduction.9 All women should be screened for syphilis at their initial prenatal visit. Women who have risk factors for acquisition of syphilis during pregnancy, including a history of prior syphilis infection, uninsured status or low income, diagnosis of an STI during pregnancy, residence in a high morbidity area (primary or secondary syphilis rate >2/100,000 persons), substance use/abuse, and/or transactional sex (i.e., sex exchanged for drugs and/or money) should be tested again at 28 weeks’ gestation and at delivery.5,7,9 All women treated for a syphilis infection during pregnancy should receive follow-up serologic testing at 1, 3, 6, 12, and 24 months. Treatment failure or reinfection should be suspected in women who have persistent symptoms or who have not achieved a fourfold reduction in titers.5,9 Testing for syphilis should be done for all women who experience an intrauterine fetal demise after 20 weeks’ gestation.5
More than 40% of pregnant women experience the Jarisch-Herxheimer reaction.7 For non-pregnant women, this reaction is unpleasant but does not result in adverse outcomes. However, pregnant women who experience this reaction are at risk for preterm labor/birth, fetal heart rate decelerations, and fetal death.7 Decisions about location of treatment for pregnant women should be individualized and based on overall maternal health, pre-existing conditions, and gestational age. If a high level of concern about preterm labor and fetal heart rate abnormalities exists, HCPs may want to initiate treatment for syphilis in the labor and delivery unit, where fetal monitoring and close maternal assessment can occur.7 Treatment of syphilis should not be delayed because of concerns about a Jarisch-Herxheimer reaction.
Congenital syphilis
Congenital syphilis occurs when an infected pregnant woman transmits syphilis to her unborn child prior to or at the time of delivery.10 Active syphilis infections during pregnancy can have a wide range of effects not only on the outcome of the pregnancy but also on the health of the newborn. Syphilis that is untreated or treated extremely late in gestation leads to CS in more than 50% of births and can cause stillbirth, neonatal death, or morbidities such as visceral or neurologic damage in the infants who survive.10 By contrast, if pregnant women receive treatment for syphilis at least 30 days prior to delivery, CS is less likely to occur.11 However, not all cases of CS or fetal death can be prevented, especially if the infection has been present for the entire pregnancy.11 In general, the sooner a pregnant women is treated, the lower the risk of fetal compromise. Congenital syphilis prevention in the U.S. is challenging because of difficulty in diagnosis, lack of HCP awareness, and lack of patient access to prenatal care. Diagnosis of CS can be complicated because maternal antibodies can be transferred through the placenta to the fetus, confounding interpretation of the results of serologic tests. As such, treatment decisions are based on identification of syphilis in the mother, adequacy of maternal syphilis treatment, presence of evidence (clinical, laboratory, or radiographic) of syphilis in the neonate, and com-parison of maternal and neonatal serologic titers at delivery.5 Neonates born to women with reactive serologic test results should be examined thoroughly for signs of CS. These signs include, but are not limited to, nonimmune hydrops, jaundice, hepatosplenomegaly, rhinitis, skin rash, anemia, edema, pseudoparalysis of an extremity, or an elevated cerebrospinal fluid white blood cell count.10 Infants who exhibit signs of CS, once a confirmed diagnosis or suspected diagnosis has been made, should be treated with penicillin for 10 days, and all reactive neonates should be followed every 2-3 months with careful examination and serologic testing until the testing result be-comes nonreactive.5
Long-term outcomes of CS vary, depending on when diagnosis was made and when treatment was initiated. Neonatal outcomes of CS include bone abnormalities, severe anemia, enlarged liver and spleen, jaundice, skin rashes, and neurologic sequelae such as blindness, deafness and meningitis.12 Of note, a neonate with CS could possibly have no S/S at birth but develop them later on. Without adequate treatment, neonates with CS can experience developmental delays and even death.
Practice implications
Comprehensive sexual history taking is essential for identification of women who are at risk for syphilis and who would benefit from screening. To glean this information, HCPs need to ask sensitive questions about patients’ sexual practices and sexual partners, as well as about other risk factors for syphilis such as injection drug use. All questions should be posed in a nonjudgmental fashion and approached in a health-promotion framework to preclude women from feeling as though they are being targeted based on race, ethnicity, age, sexual orientation, gender identification, relationship status, or any other sociodemographic characteristic. Resources for HCPs to assist with discussions regarding sexual health and sexual history can be found here.
Providers who care for women need to be aware of risk factors for syphilis and current screening recommendations. Because syphilis is less common than other STIs, HCPs may be less confident about how to interpret laboratory results and initiate treatment. Not all pharmacies have benzathine penicillin G in stock. HCPs should be aware of medication availability and consult with their local department of public health or an infectious disease specialist if questions about treatment arise. In addition, HCPs can request a consultation through a service provided by the National Network of STD Clinical Prevention Training Centers.
Patient education is essential for successful treatment of syphilis. First-line treatment is given by IM injection, which requires patients to return to the clinic or office after confirmation of the diagnosis. Although most cases of syphilis can be treated in one visit, returning to an HCP can present a barrier to care, especially if patients have concerns regarding insurance co-pays, lack of insurance, transportation, and time off from work. Second-line oral treatments are less effective and require a prolonged course
of antibiotics and dosing up to 4 times/day. Missed doses and inability to complete the entire treatment regimen contribute to treatment failure.5 HCPs must provide patients with the rationale for IM administration and acknowledge that acquiring the medication and returning to the office for administration may be burdensome. HCPs should work with office staff and patients to find scheduling options that promote access to care.
Conclusion
Although syphilis is a relatively less common STI, the incidence of the disease has recently risen after decades of decline. Diagnosis may be challenging because of S/S that can be missed or confused with those of other diseases. Screening is essential to prevent disease transmission and sequelae. HCPs who see women in their practices should be aware of risk factors, screening tests, and treatment for syphilis to reduce disease burden.
References
1. CDC. Sexually Transmitted Disease Surveillance 2016. Atlanta, GA: U.S. Department of Health and Human Services; 2017.
2. Cantor A, Nelson HD, Daeges M, Pappas M. Screening for Syphilis in Nonpregnant Adolescents and Adults: Systematic Review to Update the 2004 U.S. Preventive Services Task Force Recommendation. Evidence Synthesis No. 136. AHRQ Publication No. 14-05213-EF-1. Rockville, MD: Agency for Healthcare Research and Quality; 2016.
3. Watts PJ, Greenberg HL, Khache-moune A. Unusual primary syphilis: presentation of a likely case with a review of the stages of acquired syphilis, its differential diagnoses, management, and current recommendations. Int J Dermatol. 2016;55(7):714-728.
4. Cantor AG, Pappas M, Daeges M, Nelson HD. Screening for syphilis: updated evidence report and systematic review for the US Preventive Services Task Force. JAMA. 2016;315(21):2328-2337.
5. Workowski KA, Bolan, GA. Sexually transmitted diseases treatment guidelines, 2015. MMWR Recomm Rep. 2015;64(No. RR-3):1-137.
6. Barragan NC, Moschetti K, Smith LV, et al. Differential declines in syphilis-related mortality in the United States, 2000-2014. Am J Infect Control. 2017;45(4):417-420.
7. Rac MW, Revell PA, Eppes CS. Syphilis during pregnancy: a preventable threat to maternal-fetal health. Am J Obstet Gynecol. 2017;216(4):352-363.
8. Gomez GB, Kamb ML, Newman LM, et al. Untreated maternal syphilis and adverse outcomes of pregnancy: a systematic review and meta-analysis. Bull World Health Organ. 2013;91(3):217-226.
9. Tsimis ME, Sheffield JS. Update on syphilis and pregnancy. Birth Defects Res. 2017;109(5):347-352.
10. Su JR, Brooks LC, Davis DW, et al. Congenital syphilis: trends on mortality and morbidity in the United States, 1999-2013. Am J Obstet Gynecol. 2016;381.e1-381.e9.
11. CDC. Pocket Guide for Providers. 2017. Atlanta, GA: U.S. Department of Health and Human Services; 2017. cdc.gov/std/syphilis/Syphilis-Pocket-Guide-FINAL-508. pdf
12. CDC. Congenital Syphilis-CDC Fact Sheet 2017. Atlanta, GA: U.S. Department of Health and Human Services; 2017. cdc.gov/std/syphilis/stdfact-congenital-syphilis.htm